
Abstract
Background:
One of the fundamental pillars of integrating a palliative approach in nursing home care is increasing professional competencies and institutional capacity. However, conventional training designs have been proven to fall short of supporting this integration. This paper details the results of a practice development intervention that used critical companionship as a learning design to facilitate the integration of a palliative approach in the care of nursing home residents in France.
Objectives:
This study aimed to explore the perceived outcomes of Padi-Palli critical companionship in supporting the integration of a palliative approach in the care of residents in nursing homes in France.
Design:
Qualitative multiple case study situated within a constructivist theoretic lens.
Methods:
This qualitative multiple case study is part of a larger interventional mixed-method study. Nurses with palliative care clinical expertise facilitated experiential learning with nursing home professionals for 10 months spread across three phases. At the end of the intervention, a purposive sampling method was used to select professionals from six nursing homes that participated, including leaders and critical companions. Focus groups and individual interviews were used to collect data between February 2023 and March 2024. Data analysis followed Braun and Clarke’s reflexive thematic analysis.
Results:
Four interrelated themes explained how Padi-Palli critical companionship enhanced the palliative care competencies of professionals, improved nursing home palliative care practices, supported organisational practices for palliative care and facilitated collaborative learning at the bedside. The collaborative and co-creative principles that informed the delivery of the Padi-Palli critical companionship program facilitated a culture shift towards integrating a palliative approach in resident care at individual, team and organisational levels.
Conclusion:
Critical companionship offers an innovative practice development approach that can support the delivery of timely palliative care for residents in nursing homes.
Trial registration:
ID-RCB 2020-A01832-37.
Keywords
Introduction
To enhance the quality of life for frail older adults with life-limiting conditions, the World Health Organization strongly recommends integrating a palliative approach into the continuum of care for older persons who spend significant time in a nursing home (NH) and ultimately die in this setting. 1 A palliative approach to care encompasses a comprehensive, person-centred approach that adapts and integrates palliative care principles across care settings and involves early identification and proactive response to the evolving needs of residents and their families facing life-limiting conditions throughout their illness trajectory, to enhance the overall quality of life, dignity and comfort.2–4 Palliative care has traditionally been provided to people dying from incurable cancer; therefore, its principles have been insufficiently applied to residents in NHs dying of non-cancer multiple morbidities. 5 However, during the last decade, significant policy initiatives have been undertaken globally to support the development of palliative care within NHs.1,6
As a result of these initiatives, tailored approaches to the provision of palliative care in the ageing context have been developed. These approaches include NHs solely relying on external palliative care specialists, using their in-house professionals and building in-house capacity combined with external support from palliative care specialists.7,8 The in-house capacity-building model combined with external support has been found to broaden access to palliative care for all NH residents through the support of external specialists. 8 This aligns with a palliative care approach as professionals who best know the residents can identify their needs early and external support is still available for complex situations. As a result, the residents can remain in the NH until their death if they prefer and their relatives can receive ongoing support from professionals they already have a relationship with.8,9
Since palliative care is rarely the primary area of expertise for NH professionals, the success of the in-house palliative care model requires strong capacity-building strategies to develop a skilled, competent, compassionate and knowledgeable interprofessional workforce. 10 Several studies have revealed NH professionals have suboptimal knowledge of basic palliative care principles, including symptom management such as pain and anxiety, oral care, nutritional needs, dyspnoea, communication strategies and the dying process. 11 This competencies gap constitutes a significant barrier to the successful integration of palliative care into NHs and may likely make these professionals unfit for the role as well as hinder interprofessional collaborative palliative practices.10,12
The NH workforce in France consists of a mix of professionals with different levels of training and competencies under the supervision of a medical coordinator. Nurses and nurse assistants provide front-line palliative care to residents with the support of other regulated professionals such as physiotherapists, occupational therapists and psychologists. Non-health professionals like personal support workers and recreational and dietary aids actively collaborate with nurses and nurse assistants to support residents’ quality of life. In the majority of cases, however, this workforce is unprepared to provide palliative care. 13
Currently, the majority of NHs in France have adopted the palliative care consult service model. 8 When a resident requires palliative care, the NH requests support from a specialised palliative care team. However, this request is often delayed until the last days of the resident’s life, and in most cases, the lack of availability of the specialised palliative care team does not allow the provision of needed support. Consequently, palliative care needs are typically unmet and the risk of emergency hospitalisation is extremely high. 14 To advance a palliative care approach into NH resident care, it is critical to create a caring culture that prioritises early palliative care and empowers professionals with the competencies required to effectively deliver this approach.
To optimise the knowledge and skills of their professionals, most long-term care settings rely on traditional learning strategies for key topics such as geriatric symptom management, palliative care and complex cognitive decline support. 3 However, strategies that involve sending a few professionals to classroom-based training or bringing trainers into the workplace to provide didactic courses are less effective within the complex environment of the NH, especially given its human resource shortage and high staff turnover rate.15,16 The learning benefits only a few professionals who attended the training, and the transfer of acquired knowledge into the workplace to advance organisational outcomes is challenging. 17 Moreover, traditional learning strategies ineffectively support interprofessional collaborative learning for diverse occupational groups with differing educational needs across groups. 10 Additionally, the high turnover rate makes it difficult to retain trained professionals and creates an ongoing need to retrain newly recruited staff.
Hence, despite the proven benefits of traditional learning strategies in other settings, they fail to meet the complex professional development needs in the NH context to deliver effective palliative care. There is a need to design innovative interprofessional work-based learning strategies that may help address this competency gap and support the effective integration of palliative care in NH. One of the work-based learning approaches that holds significant promise in meeting ongoing professional learning needs is critical companionship. This relational-based practice development approach involves an experienced practitioner sharing their expertise with less-experienced practitioners over an extended time period to impart knowledge, enhance competencies and improve day-to-day practice. 18
This paper reports a practice development program that used a critical companionship approach to promote the integration of timely palliative care in the NHs in France. It has a threefold aim. Firstly, it describes the philosophical underpinnings of Padi-Palli critical companionship and its core principles. Secondly, it illustrates the application of critical companionship for palliative care practice development in NH contexts. Lastly, it draws on the findings of our empirical qualitative study to demonstrate the perceived outcomes of critical companionship intervention as narrated through the experiences of NH professionals, leaders and critical companions.
Philosophical underpinnings and core principles of Padi-Palli critical companionship
Padi-Palli (Personne Agée Demarche PALLIative Intégrée) is a French multicentre interventional research project that aims to support the integration of timely palliative care in the care of older persons in NHs and ultimately improve the quality of life and care outcomes for residents and their families. 19 The project involved 21 NHs across three geographical French regions. The Padi-Palli project was informed by the consolidated Framework for Implementation Research 20 and followed three steps: the pre-implementation phase, the implementation phase and the post-implementation phase. Further descriptions of phases can be found elsewhere. 19 The implementation phase consisted of an intervention that utilised ‘Padi-Palli critical companionship’.
The design and delivery of Padi-Palli critical companionship was informed by the critical companionship framework. 18 Critical companionship is understood as a supportive relationship in which an experienced facilitator, the critical companion, accompanies a less-experienced practitioner through an experiential learning process using ‘high challenge’ and ‘high support’ techniques within a trusting two-way relationship. 18 Throughout this learning journey, critical companions utilise their practical expertise to support the co-learners in addressing their learning needs as they perceive them, aiming to facilitate a person-centred, evidence-based practice.18,21
The critical companionship framework draws on the premises of empowerment and engagement from the social sciences to enable professionals to create a culture that prioritises practice improvement, facilitates practitioners’ critical reflection on their practice, encourages taking ownership of one’s learning and supports collaborative and participative learning and care.18,22 We chose to situate our project within these philosophical underpinnings to align with the goals of Padi-Palli that go beyond merely developing the knowledge and skills of the NH professionals to co-creating an environment and organisational culture that integrates palliative care within the care approach in a timely manner and embeds learning and professional growth within the everyday practices and organisation of the NH. To reach these goals, the critical companionship approach appeared to be the most pertinent practice development strategy as it enables not the act of teaching and imparting knowledge to a few professionals but rather work-based experiential learning and knowledge co-creation with a focus on skills transmission and collaboration. 18 Critical companionship has served as a framework in some professions to facilitate learning like nursing,23–25 but rarely has it been used with practitioners working in institutions for older people. 22
The Padi-Palli critical companionship model was built on three fundamental pillars: (1) sharing knowledge and experiential clinical experience, co-constructing new knowledge, facilitating reciprocity in learning and transferring acquired learning immediately into practice; (2) valuing what already exists such as practices, workplace culture, resources and the organisation, and caring for other professionals; and (3) encouraging new initiatives, challenging the status quo, reflecting on one’s practice, participating in role-modelling and providing emotional and cognitive support. The humanistic educative values of respect, openness, creativity, emphatic understanding and person-centredness not only act as a resource and facilitate learning that responds to learner needs 26 but also form the key principles that guide the critical companions as they provide training and support. To better align with the particular work environment of the NH with its diverse professional groups, we added an interprofessional dimension to Padi-Palli critical companionship to enable interprofessional dialogue as it is key to palliative care practices. Hence, unlike the original critical companionship framework that recommends a dual relationship, 18 the Padi-Palli critical companionship model privileged the interplay between dual and multidisciplinary facilitative relationships. The learning environment emphasised experiential learning 27 at the bedside of residents and within care units instead of formal classroom-based education. Figure 1 represents the Padi-Palli critical companionship model.

Padi-Palli critical companionship model.
At the core centre of Padi-Palli critical companionship is the goal to co-create a collaborative experiential learning culture that supports the early integration of a palliative approach in the care of residents. Three key pillars form the foundation of the framework, interconnecting all layers that compose it. The middle layers represent the facilitative relationship required of the critical companions and facilitative strategies to utilise to reach the intended goals. The last layer represents the achieved outcomes of facilitating a competent NH workforce that would support an early-integrated palliative approach in the care of NH residents.
Application of the Padi-Palli critical companionship model within French NHs
In the original critical companionship framework, a companion is an experienced practitioner who supports less-experienced professionals on their experiential learning journey; this can be an insider (from within the organisation) or an outsider practitioner. 18 Whereas in the Padi-Palli critical companionship model, the critical companions were three outsider palliative care nurses with between 8 and 11 years of clinical expertise in palliative care and oncology. In addition to their nursing education, they had university degrees in palliative care, psycho-oncology and pain management, respectively, and other palliative care in-service training. The three nurses also worked in the specialised mobile palliative care teams, offering palliative care expertise and support to the hospital and home care clinical teams. In addition to their clinical expertise, they had pedagogic and leadership experience as facilitators of learning for nursing students and in-service professionals.
To recruit critical companions for this study, we advertised for the positions through palliative care networks. Of the candidates who applied, we selected three based on their rich clinical experiences and their professional references. Two of the nurses worked in two palliative care units associated with the Padi-Palli coordinating centre, while the third nurse worked in a collaborating hospital with a palliative care mobile unit. Before starting their role, the critical companions received additional training on the pillars of Padi-Palli critical companionship, its goals and the principles guiding their role.
Each critical companion was allocated to one participating region, covering seven NHs in total. While the implementation of Padi-Palli critical companionship was flexible and strived to suit each participating NH and team, three foundational activities were common to all: (1) the co-construction of a shared vision of a palliative approach to care, (2) the proactive identification of resident palliative care needs using the Palliative Care Indicator Tool (PICT), 28 and (3) the assessment of resident needs and care planning using the InterRAI Palliative Care (InterRAI-PC) instrument. 29 The rest of the activities varied depending on the specific needs of each NH, agreed upon collaboratively and based on the findings from phase I of the project.
The Padi-Palli critical companionship intervention evolved into three phases: (1) the getting-in phase, which began in March 2021 for the first NHs; (2) the co-creating and co-learning phase; and (3) the sustaining phase, which concluded in the last NH in March 2024. Table 1 displays a summary of the key actions for each of these phases.
Phases and actions of Padi-Palli critical companionship.

PICT, Palliative Care Indicator Tool.
Getting-in
The purpose of this phase was relationship and trust building. During the first 2 months, companions spent on average 10 days in each NH; they immersed themselves in day-to-day routine care and activities to value what exists, observe current workplace culture and familiarise themselves with it. Through observing professionals during care provision and engaging in informal dialogue during care, meetings and casual encounters, they sought to gain an understanding of current practices and needs in terms of the knowledge and skills required for palliative care. They built a relationship of trust and partnership with NH professionals and became accepted as members of the NH team. The observations made in this phase informed the refinement of the planning for the second phase.
Co-creating and co-learning
This phase was the core, active companionship. It started with a 2-day workshop in each participating NH, themed ‘co-creating a shared vision for a palliative approach in a nursing home’. During this workshop, which is a milestone step of the companionship process, NH staff from different professional categories, the leadership team, the critical companions, members of the external palliative care support team and the research team, engaged in a co-construction of a shared understanding and common vision for a palliative approach to care. A palliative care approach involves adapting and integrating palliative care principles into the care received by persons who have life-limiting conditions, irrespective of their age, place of care or illness, with the focus on improving their quality of life and of their families. 2 During a 2-day workshop, various professionals (nurses, nurse assistants, personal support workers, psychologists, physical therapists, occupational therapists) met with the critical companions and the research team to identify the educational and supportive needs required to provide palliative care to residents in NH. Depending on the size and the staffing level of each NH, 10–15 participants from various professional groups attended each day of the workshop. The NH leadership team identified professionals to attend based on either their current responsibilities (e.g. focal person for pain management, for palliative care, for fall prevention) or their future roles. On the first day of the workshop, the leadership team and the members of the external palliative care team joined the workshop discussions whenever possible. The expertise shared at the workshop assisted in the development of the companionship plan and the designation of the in-house focal person/team to lead the intervention activities in their setting. The information gathered from this workshop was also complemented by observations made by the critical companions in the first phase.
Next, each critical companion spent at least 30 full-time days in their assigned NH, spread through 3 months. During this phase, they worked alongside the NH professionals either as peers with one professional or in a group of professionals to provide care, identify resident needs and develop care plans. They accompanied professionals, sharing their expertise in the provision of care such as oral care, wound care, pain assessment and management, massage, care planning, and communication with residents and relatives regarding end-of-life wishes and care to the deceased resident. Critical companions used both formal and informal learning situations in the workplace, organised flash training on coffee breaks to share knowledge with other professionals and encouraged teams in the use of relevant clinical assessment tools. Formal multidisciplinary palliative rounds and meetings were encouraged to assess residents using the early identification tool PICT and the InterRAI-PC instrument to support comprehensive needs assessment and develop care plans. At the organisational level, critical companions worked with the leadership team to review work organisation, order new materials, provide space for interprofessional dialogues and renew partnerships with external palliative care support teams. Debriefing meetings were held twice a month throughout the phases between critical companions and the research team to monitor the progress of the intervention, adjust strategies to the emerging needs of the NHs and offer support to critical companions.
Sustaining
The third phase lasted for 5 months during which the companions remained in each NH for approximately 10 days, gradually reducing their presence during care but remaining available to provide advice and to intervene from time to time at the request of the NH teams. During this time, the companions observed the sustainability of the changes initiated and touched with professionals on their remaining needs. They progressively prepared for their departure by encouraging and supporting the insider resource who would assume their role to continue the journey with professionals. The phase then concluded when the companionship officially ended and the companions departed in the NH.
Perceived outcomes of critical companionship: Qualitative experiences of NH professionals, leaders and critical companions
Between 3 and 6 months after the critical companionship concluded in each NH, a qualitative study was conducted in six purposively selected NHs. The study sought to answer the following research questions: (1) How does Padi-Palli critical companionship support the advancement of a palliative approach in the care of residents in NHs? (2) What perspectives are held by professionals, leaders and companions on the appropriateness of critical companionship as a practice development strategy to support the palliative care competency development of professionals in NHs?
Methods
Study design and participants
A constructivist theoretical lens 30 informed the design and implementation of this study. The main feature of critical companionship is the co-construction of knowledge; therefore, it was assumed that participant perspectives would be shaped by how they conceptualised the experience of critical companionship through their interactions with critical companions and co-workers. We conducted a qualitative study using a multiple case study approach 31 to allow for examining individual, team and organisational dynamics and processes that pertain to how the critical companionship approach was implemented in the participating NHs, and the outcomes of the intervention as perceived by NH professionals, managers and critical companions.
The results presented in this manuscript are based on data from six NHs purposively selected based on geographic diversity; rural and urban locations; private, associative and public ownership; and varying in terms of large and small facilities. We purposively included all professionals who participated in the Padi-Palli intervention and were still employed within the NH at the time of interviews. A list of professionals who participated in the critical companionship was made available to the research team. The nurse coordinator helped to organise the focus group (FG) on a convenient day and time that facilitated their attendance.
Data collection
We conducted six FGs with NH professionals from different professional groups, each group ranging between 6 and 10 individuals. We held individual interviews with the three critical companions, key NH professionals (psychologist and occupational therapist) who were not available for FG, and with the leadership team members (the nurse coordinator, the medical coordinator and the directors) from the selected NHs. The FG discussion allowed for exploration of group dynamics, consensus and diversity 32 of experiences with critical companionship from different professionals meeting together once with minimal disruption of their work. To allow professionals to be more comfortable in expressing their experiences and to avoid any hierarchical issues, we held individual interviews with critical companions and the leadership team members. Each interview lasted between 30 and 45 min, while FGs lasted between 60 and 90 min. All interviews were audio-recorded and were held in each NH at a convenient time for participants and the service. FG discussions took place in meeting rooms in each NH, while individual interviews were held in the office of each participant. We used a semi-structured interview guide (Supplemental File 1) developed by the research team for this study. Data were collected between February 2023 and March 2024. Two experienced health professionals (BU and EB) with qualitative experience conducted interviews.
Data analysis
We analysed data following the six steps of Braun and Clarke’s reflexive thematic analysis approach, including familiarising with the dataset; coding; generating initial themes; developing and reviewing themes; refining, defining and naming themes; and writing up. 33 The level of analysis was at the NH level, and each NH was considered a case. To achieve familiarisation with the dataset, one research team member (BU) conducted a verbatim transcription of recorded interviews and did multiple readings of the recorded data, making notes of ideas that appeared interesting. The transcribed text was entered into NVivo software version 14 to manage data storage and facilitate the coding process. Once all interviews were transcribed and stored, two authors (BU and EB) started collating meaningful data segments from each case that reflected participant experiences into codes. We predominantly coded our data using a data-driven, inductive approach 34 to align with the constructivist approach and to represent a rich description of participants’ experiences and perspectives as expressed within the dataset. The list of codes from all six cases was then critically reviewed and analysed by the same two authors to identify similarities and overlaps between them, and those sharing meaning and relevance for answering the research questions were collapsed to generate initial themes. 33 Any disagreement in coding was resolved through consensus during discussion meetings. The NVivo mind-mapping function helped to explore relationships and levels of themes, leading to an initial thematic map with different preliminary themes. These initial themes were then collated and clustered into broader meaningful subthemes. 34 At this stage, we reviewed the thematic map to capture how the themes fit together to convey how critical companionship was experienced by participants and how it supported the enactment of a palliative care approach in the participating NHs. The collated subthemes were refined by the two authors and organised into a coherent and consistent account to achieve richer meaning. 35
To ensure methodological rigor, we used the recommended strategies for the trustworthiness of qualitative data. 36 To ensure the credibility of findings, we triangulated methods (individual in-depth interviews and FGs) and collected participant perspectives from various healthcare professions, the leadership team and the critical companions. To ensure the reliability of the findings, two analysts completed the coding of transcripts, organised peer-debriefing meetings throughout the analysis and kept a reflexive journal recording all the steps taken and decisions made. We used participant quotes to report the findings to demonstrate that they are grounded in participant perspectives. The Consolidated Criteria for Reporting Qualitative Research Guidelines 37 was used to enhance transparency and to improve the rigour of the findings reported (Supplemental File 2).
Ethical considerations
The French Committee of Protection of Person (CPP) granted ethical approval for this study (approval number: 2020.09.06 bis_20.07.31.64318). All interviews respected the rights of participants to choose to participate in the study through written informed consent. To ensure the confidentiality and anonymity of collected data, the reporting used codes instead of names.
Results
Participant characteristics
In total, 66 professionals took part in the study, including 49 participants in FGs, 14 participants in individual interviews and 3 critical companions. Table 2 provides the characteristics of NH participants.
Characteristics of nursing home participants.
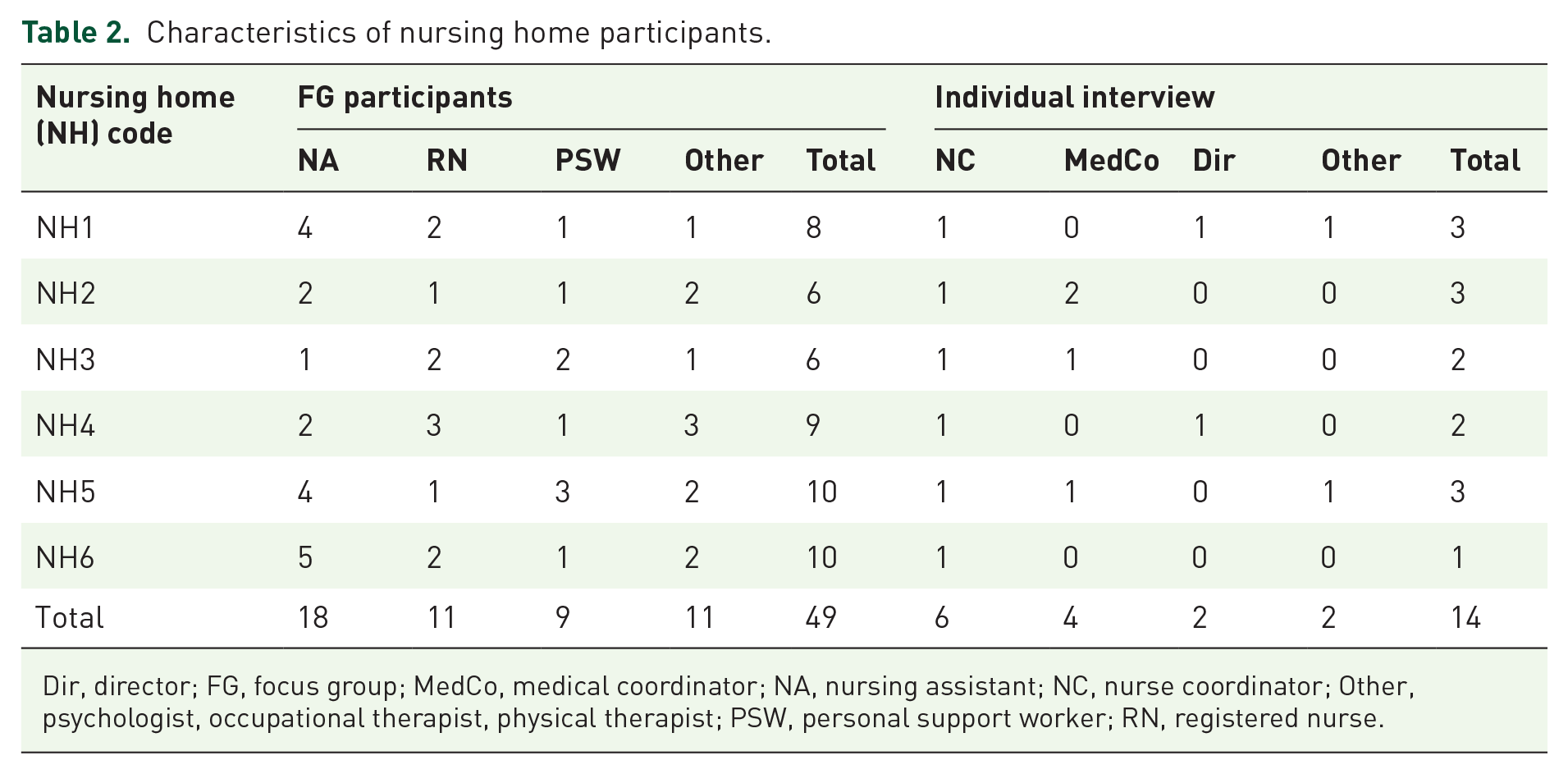
Dir, director; FG, focus group; MedCo, medical coordinator; NA, nursing assistant; NC, nurse coordinator; Other, psychologist, occupational therapist, physical therapist; PSW, personal support worker; RN, registered nurse.
Key themes and subthemes
Analysis of participant narratives revealed 4 overarching themes and 12 subthemes. The four key themes summarise how Padi-Palli critical companionship (1) enhanced palliative care competencies of NH professionals, (2) improved NH palliative care practices, (3) supported NH organisational practices for palliative care and (4) facilitated collaborative bedside learning. Generally, most of the benefits derived from Padi-Palli critical companionship were consistent across participating NHs. A more detailed presentation of themes and subthemes with illustrative participant quotes is provided in Supplemental File 3. Throughout this manuscript, a few quotes are included to illustrate participant narratives. Quotes from individual interviews are represented with an acronym designating the function or profession of the participant, whereas quotes from FGs are represented with the acronym FG, all followed by the code number of the NH.
Theme 1: Enhanced palliative care competencies
Overall, NH professionals described Padi-Palli critical companionship as a revelation that came at the right time to increase their awareness of a very sensitive topic they struggled with, that is, palliative care for older persons. The intervention enhanced their competencies at different levels leading to enhanced knowledge of palliative care principles and improved attitudes and beliefs towards death and dying.
Enhanced knowledge of palliative care principles
Narratives from professionals demonstrated that being accompanied by palliative care nurses during critical companionship broadened their understanding of the basic principles of palliative care. Some participants noted a shift in their current limited understanding of palliative care, moving from seeing it as care provided when there is nothing left to understand it as comprising ‘active symptom management’ (FG, NH1), ‘providing psychosocial support to residents and relatives’ (FG, NH5), ‘being present to provide comfort’ (FG, NH2) and ensuring ‘resident desires are documented and respected’ (FG, NH6). Many participants reported gaining a better understanding of the necessity of the psychosocial aspects of caring. One participant noted that ‘it’s now impossible for me to not find extra time to be with the person in palliative care’ (FG, NH1). Another participant shared they now understood that ‘holding hands of a dying resident is as priority care as any other type of care’ (FG, NH4).
Professionals reported gaining what they called ‘the small things that make a big difference’ (FG, NH4) in the care of residents. For example, they learned you can ‘use banana to smoothen a dry mouth’ (FG, NH5), ‘natural yoghurt or sparkling water to hydrate a non-eating resident’ (FG, NH5), or ‘baking soda’ (FG, NH2) and ‘Coke and wine for mouth care’ (FG, NH6). They also noted enhanced interpersonal and communication skills with residents in palliative care who had lost their ability to communicate verbally, such as communicating ‘using signs or inventing a new form of communication’ (FG, NH6).
During the getting-in phase of the intervention across participating NHs, pain assessment was identified as an area in which the professionals needed further knowledge and support. Following the critical companionship, many participants reported acquiring the necessary skills and increased confidence in pain assessment, monitoring and management. A participant explained ‘now we know of different scales for pain assessment and everything that goes with pain’ (FG, NH2).
Improved attitudes and beliefs towards death and dying
Before the intervention, NH staff generally reported feeling uncomfortable having end-of-life conversations and responding to death and dying questions from residents and their relatives. They preferred avoiding such discussions and referring them to other professionals believed to be better equipped such as physicians and nurses. A participant admitted that ‘We did not know how to go about the subject’ (FG, NH1). After the intervention, interviewed NH staff reported a positive shift in attitude and beliefs towards death and dying. Many shared that critical companionship opened up space for freely discussing death matters between professionals, which dissipated discomfort around death-related conversations with residents and their families. Participants reported feeling adequately equipped to respond to unpleasant death-related questions. One participant shared that ‘We are [now] able to talk about death with residents and their relatives more easily than before’ (FG, NH1).
Theme 2: Supported improved palliative care practices
In all the NHs that participated in this study, participants expressed that their competence development translated into palliative care practice improvement. The improvements entailed having a shared vision of palliative care, adoption of a timely palliative approach to care improved symptom management and enhanced interdisciplinary collaboration.
Facilitated a shared vision of palliative care
In the first phase of the intervention, palliative care was commonly associated with care in the final few days of life. Mentioning palliative care was often met with hesitation and discomfort because it was linked to the end of life. Professionals shared how critical companionship drastically changed their vision of palliative care, so much so that it was ‘no longer seen as fatal, negative’ (NC, NH5). Their perception shifted and they adopted a ‘more long-term vision and a new philosophy of care’ (OT, NH1). The majority of participants stated being comfortable mentioning palliative care because they now understood it as an approach to care and not necessarily linked to death.
Participants also recalled past team disagreements sparked by differing visions of palliative care. However, they explained that critical companionship created a space for team reflection and a shared vision. A participant noted: Critical companionship helped us to have the same vision. It does not choke us anymore to say, ‘Do we think Mrs X will still be with us 6 months from now?’ We managed to understand what this long-term vision implies, and it allows accompanying residents and their relatives in a different way. (FG, NH5)
This shared vision reinforced teamwork while enabling the professionals to deliver tailored care. It also enabled collaboration and task sharing, as participants were confident that they shared a common philosophy of care and would deliver consistent messaging to residents and families.
Facilitated the adoption of a timely palliative care approach
Participants shared that the adoption of a timely palliative approach to care manifested through the early identification of palliative care needs and anticipated care plans. One component of the intervention was to support professionals in the early identification of residents who might need palliative care. This was generally done during multidisciplinary team meetings where professionals were supported by critical companions and a research team member as they assessed each resident in a chosen unit using the PICT. This assessment identified residents who may likely benefit from a palliative approach to care. A recurrent theme in FG discussions was a sense among the professionals that the use of a tool validated their intuition and supported their decisions. A participant said: ‘We now anticipate, we ask ourselves the right questions and earlier. Who can be considered in palliative care?’ (FG, NH5).
A common view among participants in all cases was that the use of an identification tool prompted anticipated discussions, triggered palliative care conversations earlier than before and allowed properly timed palliative care as opposed to crisis management practice. Several participants noted that having the anticipated discussions lessened the tension associated with the transition to palliative care, offering more time to prepare for it.
Professionals from across categories noted that the early identification of palliative care needs leads to the development of timely care plans when they are still able to verbalise them. The early identification of needs offered professionals the opportunity to anticipate care plans that integrate residents’ wishes and avoid the last-minute planning that usually leaves both themselves and the residents and their relatives unsatisfied with the care. A participant clearly articulated the importance of ‘not being taken by surprise’ (Dir, NH1).
While the identification tool and InterRAI-PC instrument were appreciated across cases, the sustainability of their adoption in practice was deemed challenging due to time constraints in some NHs. In fact, only a handful of settings continued using the tools as part of their routine practices.
Improved symptom management
With a new understanding of a palliative approach to care integrated earlier in the care plan, professionals reported adopting a different approach to caring for the person: emphasising resident comfort from a global perspective. Along with enhancing their competencies, participants noted improvement in practice related to symptom management. A medical coordinator observed significantly increased confidence in pain symptom assessment and reporting, and systematic pain monitoring is now embedded in the routine practices of the NH. They highlighted: ‘Pain assessment is much better now, they are much more confident. They assess more systematically’ (MedCo, NH5).
Notably, pain management stood out as an area of improvement across all settings. Valid assessment scales for appropriate pain assessment for both communicative and non-communicative residents were integrated into practices.
Enhanced multidisciplinary collaboration
By offering opportunities to learn as a team, critical companionship also fostered collaboration, which then transformed into enhanced multidisciplinary collaboration through the valuing of each team member’s role, sharing the same vision and creating opportunities for discussion. Dedicated time set aside to assess resident needs using a screening tool unified professionals from different occupational groups who did not usually work together. A participant shared how those moments were ‘the rare moments where we sat together as a team to hear views from different professionals’ (FG, NH4).
Opportunities for team discussion and peer-to-peer learning increased team collaboration and helped professionals better understand the interdependence of roles in the NH. For example, one NH professional reported that they initially lacked an understanding of the psychomotor therapist role and had failed to integrate them into the day-to-day care provision. During the critical companionship intervention, sessions for ‘toilette evaluative’ were held where nursing assistants paired with psychomotor therapists during bed bathing, which allowed the professionals to learn from each other and to gain a better understanding of resident needs. Even professionals not involved in direct care reported the same awareness of the complementarity of roles and gained a better understanding of how they could further support their colleagues. One director shared how it was interesting to ‘take part in the multidisciplinary learning session with all staff’ (Dir, NH4), an opportunity that allowed a better understanding of their roles.
Theme 3: Supported organisational practices for palliative care
Participants, particularly those in supervisory roles, felt that beyond empowering professionals with palliative care competencies, critical companionship supported organisational change and innovation. Organisational changes of note included the improvement of organisational procedures and processes, increased organisational receptiveness to palliative care and enhanced collaboration between NHs and external palliative support teams.
Improved organisational procedures and processes
Critical companionship facilitated the development of mechanisms and processes to support palliative care provision. In various NHs, processes such as the nomination of palliative care champions or the creation of a palliative care committee were either initiated or formalised during the intervention. One participant explained, ‘The intervention prompted us to start a new palliative care committee that didn’t exist in our setting before’ (MedCo, NH5).
While some NHs had previously identified palliative care champions, they were often not formally recognised at the institutional level and as a result, their initiatives were undervalued, or even ignored. Other NHs had no palliative care champions identified. Critical companionship both legitimised existing champions and supported the nomination of new ones. One participant stated that because of the intervention, their Director had ‘set up a working group of palliative champions. It was the first of this kind where we were formally appointed and sent on a mission’ (FG, NH2).
New processes put in place during the intervention also included updating palliative care materials and investing in new materials to enhance resident care quality. For example, in some NHs, critical companions observed a lack of varied palliative care supplies and worked with the professionals and pharmacies to source new materials such as air mattresses, comfort chariots, oral care sticks and baking soda.
Increased organisational receptiveness to palliative care
Most interviewed leaders mentioned that the activities of the Padi-Palli intervention increased their awareness of the necessity of having streamlined policies in place to support the further integration of a palliative approach in resident care. Several leaders mentioned adopting ‘a new approach to care’ (Dir, NH1), facilitating ‘a new culture in the provision of palliative care’ (Psy, NH5) or welcoming a ‘breeze of newness’ (FG, NH6). While for others, the experience reiterated the necessity to ‘formally integrate palliative care in the projet d’accompagnement personnalisé’ (MedCo, NH5), an individualised care plan created shortly after a resident enters the NH. A nurse coordinator highlighted how this has become standard and embedded in their culture: ‘We revisited the “PAP” Projet d’accompagnement personalisés (individualised care plans) to include the palliative care dimension’ (NC, NH5).
The use of an early identification tool allowed NHs to better understand the current needs of their population and prompted a shift to invest more resources into palliative care. Most medical coordinators were surprised to discover that the use of assessment tools indicated a higher number of residents potentially requiring a palliative approach to care than they expected. Some reinforced their supportive policies such as anticipated prescriptions to ensure that residents requiring pain relief received it without needing emergency transfer. Some settings started organising palliative care round meetings and formalised documentation of palliative care decisions.
Enhanced collaboration between NHs and external palliative support teams
Most NHs participating in the study had collaboration agreements with external palliative care support teams to offer expertise in caring for complex residents. This collaboration remained suboptimal in some settings, but with the support of critical companionship, some NH teams and palliative care teams met to share concerns and restructure their collaboration. Participants reported increased openness in requesting palliative care team intervention, more reactive response from the palliative team and a better two-way relationship as one medical coordinator shared: ‘The collaboration with our partners is more fluid, and this is thanks to the bridge built with the project’ (MedCo, NH2).
The project also connected NHs to supportive resources they had not previously utilised. For example, in one NH, participants shared how the critical companion connected them to a palliative care unit for a respite stay for a declining resident. The resident had complex care needs and attempting to meet them had caused the team severe compassion fatigue. The connection to the specialised palliative care unit allowed quality relief to the resident, their relatives and the care team.
Theme 4: Facilitated collaborative bedside learning
In their accounts of experiences with critical companionship, a recurrent theme across all cases was the collaborative grounding of the design of critical companionship and the relational qualities that characterised the companions during the delivery of the intervention. Overwhelmingly, participants across settings appreciated reciprocal learning, bedside learning and the non-judgemental support they received from their critical companions.
Enabled reciprocal learning
One of the key pillars of critical companionship is knowledge sharing and reciprocity in learning. Several participants particularly appreciated learning together as a team of professionals during care provision, supported by the companions. They felt that peer-to-peer learning enhanced their collaboration and forged a culture of inquiry and knowledge sharing. One participant specifically underlined the importance of team learning: ‘we were doing it as a team; it helped us to learn together’ (FG, NH5).
Reinforcing the importance of reciprocal learning, critical companions also shared how the learning not only benefitted NH professionals but also critical companions themselves felt they learned a lot from the experience. One noted that ‘the experience was transformative. . ., there will always be a before and after critical companionship. It has expanded my gerontology knowledge’ (CC, 1), while for another, the experience has become ‘a guiding reference in my current practice after the companionship’ (CC, 3).
Supported bedside learning
Most of the learning throughout critical companionship took place during care provision in a resident’s room as opposed to in a classroom environment. Referring to this bedside learning, critical companions explained the importance of ‘getting your hands dirty’ (CC, 2) or ‘adding oil in the wheel’ (CC, 1) to facilitate learning embedded within everyday practice. The professionals echoed these views, indicating that learning from the companions during care provision allowed hands-on learning, better understanding and immediate application of new knowledge directly translated into practice. One participant noted, ‘We were in doing it together, not listening to a lecture, rather in seeing, living it, and interacting as we care’ (FG, NH1). Participants were unanimous on the added value of having an outsider with notable palliative care expertise who got involved in bedside care provision for a sustained period in their team. One of the medical coordinators perceived such a supportive presence as ‘a valuable gift’ (MedCo, NH2). More specifically, they said, ‘Having a staff (member) from JG (a hospice unit) on our team was a valuable gift, isn’t it?’ (MedCo, NH2). Critical companions echoed this sentiment, noting it was at the bedside that ‘priority-learning needs were (better identified)’ (CC, 1) and where they were able to propose a companionship that met those needs. Other participants alluded to the fact that by observing critical companions doing care with them they acted as role models to emulate. One participant discussed the specific traits of their critical companion and how they would strive to follow their example: They were very gentle in handling residents, in mobilisation. They brought that humanity to us. The fact of gently wrapping someone during bed bathing, sitting to be closer to residents. We could do nothing but learn by seeing them doing and we imitate them. (FG, NH1)
In another FG, a participant illustrated the impact of role modelling on their practice. They discussed a time when they were preparing to provide oral care to a resistive resident with biting behaviours but remembered ‘having seen S. [critical companion] doing it with a mouth prop’ (FG NH1), so they reproduced what they had learned and safely provided the necessary care. Critical companions shared that they aimed to role model alternative behaviours at the bedside for the professionals during care provision.
Offered non-judgemental support
Across NH settings, professionals praised the critical companions for their relational qualities and their ability to build trust. A number of qualities emerged in the FG that facilitated this relationship-building, such as ‘calmness’, ‘non-judgemental’, ‘kindness’, ‘supportive’, ‘considerate’, ‘availability’, ‘ability to listen’, ‘undivided attention’, ‘friendly’, ‘motivational’, ‘committed to the team’ and ‘pleasant’. Participants appreciated the non-judgemental attitude of the critical companions who facilitated practice improvement without imposing new ways of doing it. One participant explained they were ‘very considerate; they never come in saying we are going to do it this way’ (FG, NH3), while another participant added, ‘They knew how to get involved and work with us rather than telling us how to do. Gentle and supportive’ (FG, NH3).
Some professionals viewed critical companions as non-judgemental peers to whom they could confide their professional concerns without fear of being judged. In several instances, participants mentioned feeling supported and reassured by the presence of critical companions who appreciated what they did, respected them, and helped them recognise and use their undervalued skills. One critical companion was touched by the trust they gained and the confidence they received: ‘Some have even confided in me their feelings, their lack of sense of worth, and their lack of confidence’ (CC, 2). The supportive relationship they forged with the critical companions instilled in some professionals the desire to pursue a career in palliative care as it added meaning to their work.
Discussion
This manuscript presents the design, application and stakeholder experiences of the Padi-Palli critical companionship practice development intervention, which aimed to promote the integration of an early palliative care approach in the care of residents in NHs in France. Prior studies have noted the importance of workplace learning designs that are appropriate to the constrained learning context of the NH.15,17 The most striking finding that emerged from this study was the appreciation of the collaborative and co-creation principles that informed the design and the delivery of the Padi-Palli critical companionship intervention.
NH professionals and leaders appreciated having dedicated supportive nurses who provided clinical expertise through collaborative learning during everyday practices in the workplace. This process of co-creation and partnership is the hallmark of the Padi-Palli critical companionship approach and is significantly different from other learning approaches participants were familiar with. One possible reason for this appreciation might be that NHs and palliative care practices are by nature collaborative even when professionals must navigate resource constraints. The resident bedside learning embedded in Padi-Palli critical companionship tapped into this inherent collaborative nature and supported the creation of communities of practice 38 within NHs. Another possible explanation could be that the dedicated project resources and support from critical companions helped reduce the perceived burden of participating in the intervention alongside other NH responsibilities. Professionals also felt valued, respected and recognised as part of the palliative care community.
A community of practice is perceived as a context where practitioners of different skills and clinical experiences with a common goal come together and learn from one another through sharing and creating knowledge during regular social interactions in the context of their practices. 39 The NH environment, serving both as a living space and a care facility, provides a relevant social context for communities of practice to emerge, as learning is situated within the context of the interplay between life-enriching and caring activities. 40 Findings from our study highlighted how reciprocal and peer-to-peer learning fosters collaborative reflections, nurtures teamwork spirit and furthers multidisciplinary collaboration. Padi-Palli critical companions acted as facilitators of learning to provide support and role model the appropriate behaviours during care provision, all the while learning from interacting with NH professionals. The relational qualities of the critical companions allowed trust and professional cohesion to emerge, essential characteristics of communities of learning.
Approaching learning from this perspective allowed a shift from a ‘working and learning’ approach towards a ‘working is learning’ 15 approach, which integrates learning as part of everyday practice, and positions everyday practice as a learning and teaching moment. The findings suggest that designing Padi-Palli critical companionship in a way that does not dissociate learning from care provision comes with added benefits. All professionals were eager to be supported to learn while providing care, which enhanced the immediate translation of acquired skills into practice. The second benefit, which is supported by previous studies, is that learning while providing care relieved professionals and managers of the burden of delegating care responsibilities to other professionals to attend classroom teaching, a delegation that can increase the feeling of being overburdened and likely impact quality of life at work. 41 Instead, participants described how learning with critical companions provided them with both practical and psychosocial support amidst their busy schedules.
Studies that used models similar to critical companionship reported comparable experiences regarding the supportive role of the palliative care nurse specialist for the capacity building of NH professionals. A Canadian study 2 used a ‘link nurse’ to support the introduction of a palliative care approach into Canadian NHs. Similarly, a Scottish study 42 used palliative specialist nurses to provide support and training in NHs in Scotland, while another study 43 employed palliative care nurse specialists to provide onsite mentorship to long-term care staff to improve palliative care delivery in long-term care facilities in New Zealand. Together, these results provide important insights into the potential benefits of designing work-based learning approaches where clinical expertise from palliative care specialists is provided onsite to support the transfer and sustainability of learning.
The study’s findings confirm that Padi-Palli critical companionship can positively facilitate a culture shift towards integration of a palliative approach in the care of residents at individual, team and organisational levels. At the individual level, the approach deepened the knowledge and competencies of the professionals as evidenced through their changed attitudes that normalised death and dying, increased knowledge on principles of palliative care, empowered communication about palliative care with residents and families, and improved confidence in symptom management. Through the ‘encouraging’ pillar of Padi-Palli, the program engaged NH professionals in a reflexive process to challenge their old ways of doing and fill knowledge deficits to create an expanded understanding of the psychosocial aspects of palliative care. The facilitative domains of critical companionship that model consciousness-raising, reflection on one’s practice, and the problematisation of taken-for-granted practices 21 supported professionals in gaining an increased sense of autonomy, creativity in practice and confidence in providing care to residents requiring palliative care. In some NH settings, increased confidence led to perceived efficacy for providing palliative care, which subsequently became a retention motive for professionals who had previously expressed their intention to leave the NH environment. Research has shown that critical companionship sustains the enlightenment, empowerment and emancipation of professionals, 22 and our study supports these findings in relation to caring for residents requiring palliative care in NHs. Equipping professionals with palliative care knowledge can lead to professional fulfilment and work satisfaction, 44 and can contribute to increased happiness on a personal level. 45
At the team level, Padi-Palli supported the improvement of NH care provision through the enhancement of palliative care practices. This was demonstrated largely through a renewed and shared vision for palliative care, integration of palliative discussions earlier in resident care, earlier identification of palliative care needs using validated tools, development of anticipatory care plans, improved symptom management and enhanced team collaboration. Findings across NHs demonstrated important clinical and decisional changes reflected in unit practices in relation to how palliative care was provided. One possible reason for this immediate translation of acquired skills into unit practices is that the Padi-Palli intervention was not a classroom-based one-off training; rather, it utilised hands-on collaborative learning that occurred on an ongoing basis within the flow of everyday practice. Indeed, a previous systematic literature review noted that the brevity of conventional educational interventions in NHs did not allow for complex issues surrounding end-of-life care to be explained in detail, making it unlikely the training had altered clinical behaviour or changed practice. 46 Our findings support this previous research and underscore the dire need to redesign training interventions to occur on a continuous basis within the flow of work to facilitate the immediate uptake of learning into unit practices.
At the organisational level, Padi-Palli critical companionship supported the creation of optimal organisational processes to support an integrated palliative care approach within the care of residents. Through participating in this practice development program, NH settings became more receptive towards palliative care; at multiple times, directors and medical coordinators involved in the study alluded to how the program instilled a new organisational dynamic towards palliative care. This was translated through renewed leadership commitment to palliative care, including integrating palliative care into the organisation’s strategic plans, creating guidelines to facilitate the adoption of a palliative approach, obtaining resources and equipment to support improvement in palliative care provision and strengthening collaboration with external palliative support teams. This finding is promising for the sustainability of the learnings and improvements gained during this intervention as previous studies have noted that translating individual learning into organisational learning in NHs is challenging. 17
Adopting critical companionship for learning rather than using traditional training strategies supported individual, team and organisational development by improving individual and collective competencies; reinforcing learning; and encouraging individual professionals, teams and organisations to engage in a process of practice improvement through innovation and change.17,47 Organisational readiness has been identified as a crucial factor for the effective implementation of palliative care innovations in long-term care facilities, 48 but it requires optimal organisation culture and working environments where learning and application of skills are supported. 49 Padi-Palli critical companionship’s philosophical underpinnings that focus on empowerment can create conditions that foster individual, team and organisational readiness for change and improvement.
The findings from this study hold implications for practice and research. The findings underscore the urgent need for co-creating a culture of learning in NHs to facilitate collaborative communities of learning where every work interaction is a learning opportunity. Critical companionship can also help forge communities of learning to deliver effective palliative care and improve resident quality of life. Thus, this learning approach should be institutionalised, and a formal monitoring system should be put in place to support its adoption, dissemination and sustainability. By so doing, NH organisations could potentially retain a competent, confident, reflective and satisfied NH workforce, thereby improving the quality of palliative care provided to NH residents and their relatives. The fundamental pillars of the Padi-Palli critical companionship model, that is, sharing, valuing and encouraging, mobilise not only the technical expertise of the critical companions but also their relational qualities. Indeed, the professionals involved in the study identified the relational qualities of the critical companions as the central driving force underlying the learning process and the benefits gained from the intervention. This suggests that NHs that want to explore integrating critical companionship into their settings must consider the professional competencies and the relational and human qualities of the critical companions. The co-learning journey through critical companionship involves blending the professional competencies of the companions in their domain of expertise with their relational qualities, including who they are as persons, their ability to forge trust, generate respect, offer non-judgemental support and demonstrate generosity in giving and receiving knowledge from the co-learners. Preparation for the role is key but differs in length depending on whether the companion is an experienced professional and skilled facilitator (as was the case in this intervention) as opposed to a novice facilitator. 21
A key strength of this study resides in the multiple perspectives from multidisciplinary NH staff; the NH leadership team as well as the critical companions who delivered the intervention. This offered a broader understanding of its effectiveness. Additionally, the paper not only reports the design of the Padi-Palli critical companionship model but also provides details on its application in the French NH context and shares empirical findings on its effectiveness. This constitutes a strength for other scholars who may want to replicate the model in different settings. We have embedded an interprofessional component into the critical companionship framework, as we believe it is critical but lacked emphasis in the original framework. Given the required interprofessional and multidisciplinary collaborative approach in the provision of comprehensive care to residents requiring palliative care, 10 this conceptual expansion has made a substantial contribution to advancing the application of critical companionship in NH settings where caregivers across professional backgrounds must learn and work together to develop person-centred care practices. Facilitating learning and practice development within these complex and adaptive settings calls for using collaborative learning approaches and blending individual, team and organisational learning to create communities of learning and caring. 50
In terms of limitations, this study relied on qualitative data, which involves subjective perspectives. Additionally, the time constraints of the intervention did not allow for measuring the effectiveness of the critical companionship and the sustainability of improvements brought about by it over time. Moreover, the data collected did not allow for an understanding of the effects of the approach on quality of care as perceived by residents and their families. Additional research is warranted to analyse the robustness of the impact of this practice development approach taking into consideration both resident and system outcomes.
Conclusion
Given the projected increase of older persons with complex needs who will require palliative care in the future, 51 there is a pressing need to ensure that NH professionals are properly equipped to deliver effective palliative care. Only then will NH professionals be able to meet the physical, psychosocial and spiritual needs of residents and their families to provide timely and integrated palliative care. Findings from this study demonstrate the effectiveness of the Padi-Palli critical companionship model in NHs to facilitate continuous learning to empower professionals, units and organisations with the necessary competencies to improve residents’ quality of life and successfully accompany them through both living and dying. This intervention offers an innovative practice development approach that supports the culture shift needed in NHs to integrate a palliative approach earlier within the care routine of residents. Experiences from this study suggest that creating and sustaining a palliative care approach in NHs is possible if individual professionals, teams and organisational leadership combine efforts to build a collaborative practice development process that will ultimately result in the infrastructure and culture required to sustain a work-based learning culture.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241293819 – Supplemental material for Fostering timely integrated palliative care in nursing homes through critical companionship: experiences from a Padi-Palli interventional study in France
Supplemental material, sj-docx-1-pcr-10.1177_26323524241293819 for Fostering timely integrated palliative care in nursing homes through critical companionship: experiences from a Padi-Palli interventional study in France by Emmanuel Bagaragaza, Benoite Umubyeyi and Danièle Leboul in Palliative Care and Social Practice
Footnotes
Acknowledgements
We are grateful to the nursing homes and professionals who participated in the study. We acknowledge the contribution of the palliative care nurses who played the role of the critical companions.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.