
Abstract
Background:
The Global Organization Board of the Cancer Association Network projected global number of cancer cases to reach 35 million by 2050. In Africa, patients with newly diagnosed cancer are projected to double by 2030, underscoring the need for comprehensive strategies encompassing prevention, early detection, treatment, and palliative care (PC). However, PC service in Africa remains fragmented, often lacking holistic and continuous care delivery, with more emphasis on facility-based services.
Objective:
This scoping review aims to synthesize available evidences on PC approaches for cancer patients in Africa, challenges in PC delivery, and suggested measures to improve PC.
Method:
This scoping review employed the Joanna Briggs Institute review methodology. Extensive search of published and unpublished literature in English was conducted using databases including MEDLINE (PubMed), Embase (Ovid), Web of Science Core Collection, Scopus, Google Scholar, and Google. Records of 1242 were identified; after removing 309 duplicates, 933 citations were screened for abstract review using Rayyan software. Three reviewers assessed abstracts, and full texts resulting in inclusion of 27 studies.
Findings:
The findings are organized under three themes. The first theme addressed PC approaches in Africa, including home-based, community-based, facility-based, integrated, and comprehensive models. Despite the availability of multiple PC approaches, most countries in Africa primarily practice pain relief, with limited adaptation of the psychological, financial, spiritual, and end-of-life care need of the patients. The second theme identifies the challenges in comprehensive PC provision that includes restrictive opioid laws, under-funding, shortages of workforce and resources, and gaps between PC needs and available services. The third theme synthesizes suggested measures for improvements which indicate the necessity of a shift toward comprehensive, patient, and caregiver centered models with smooth referral practices. These suggestions also emphasize policy reforms to improve access to medicines and funding, and education for health workers and community volunteers.
Conclusion:
In Africa, PC remains largely inaccessible, fragmented, and of poor quality despite the existence of different approaches. To bridge this gap, implementation of a comprehensive care model that ensures continuity of care among home, community, and facility is crucial.
Review registrations:
Open Science Framework (osf.io/np9vq).
Introduction
Cancer is an important public health problem worldwide, and 18.1 million new cancer cases and 9.6 million cancer deaths were reported in 2021 by the Global Organization Board of Cancer Association Network (GLOBOCAN). 1 Africa faces a disproportionate and rapidly increasing challenge characterized by a higher ratio of mortality to incidence compared to other regions. The incidence and mortality rates are projected to rise, with cases expected to increase from 1.1 million and 711,429 deaths in 2020 to 2.1 million cases and 1.4 million deaths in the coming decades. This is attributed to factors such as aging populations, adoption of lifestyle risk factors, and limited access to prevention, early detection, and treatment services. 2 This burden underscores the need for the integration of palliative care (PC) as an essential component of universal health coverage and a fundamental human right, as advocated by the World Health Organization (WHO). 2
WHO defines palliative care as an approach intended to be safe and effective in improving the quality of life of patients and their families by preventing and alleviating physical, psychological, social, spiritual, economic, and end-of-life suffering. 3 Studies have shown that when PC is introduced early in the course of illness, alongside curative treatments, it can help prolong life. 4
Globally, the need for PC is growing due to the increasing burden of non-communicable diseases. 5 In Africa, approximately 80% of patients with cancer are diagnosed at a late stage due to limited screening infrastructure, health-seeking behaviors influenced by cultural beliefs and stigma, and weak primary healthcare referral systems. 6 According to a WHO report from 2020, more than 56.8 million people worldwide require PC annually, including 31.1 million before and 25.7 million near the end of life. Of those in need, only 14% actually receive PC, with the majority residing in high-income countries.7,8 Most individuals requiring PC (67.1%) are adults; among them, 36.5 million have PC needs related to non-communicable diseases, with cancer accounting for 34% second only to cardiovascular diseases. Notably, 76% of the global PC need arises from low-income countries.5,9
As a result of this growing demand, PC has become a key part of the global health agenda. The World Health Assembly passed resolution EB134.R7, calling on member states to integrate PC into the continuum of care. The resolution asserts that relief from pain whether physical, psycho-social, or spiritual is an ethical responsibility of healthcare professionals and the institutions that support them. This includes developing appropriate PC policies at local and national levels, allocating sufficient budgets, ensuring access to essential medications, and supporting the training and continuing education of healthcare workers in PC. 10
Despite the proven benefits of PC in addressing the social, psychological, economic, spiritual, and functional challenges faced by patients with cancer, PC delivery in many African countries remains inconsistent and inadequate. This is due to the absence of comprehensive, integrated, and continuous approaches to care; a shortage of trained professionals such as counselors, PC specialists, oncologists, psychologists, psychiatrists, and social workers; and limited resources necessary for quality service provision.11,12 Furthermore, how hospital teams collaborate with primary healthcare structures, organization, and caregivers to offer home and community-based services remains unclear. Similarly, how to involve trained healthcare workers, health extension workers, community leaders, volunteers, caregivers, traditional healers, and spiritual leaders in the health system to maintain continuity of care is still largely unknown.13–15
Therefore, this scoping review explores the current PC approaches for patients with cancer in Africa, highlighting existing practices, challenges to comprehensive PC delivery, and suggested strategies for improvement of palliative care delivery. The evidence will bridge the gap between global palliative care ideals such as the WHO’s public health model for palliative care focusing on policy, education, medication availability, and implementation and the unique socioeconomic, cultural, and healthcare infrastructural realities of African nations. In doing so, it contributes important regional perspective to the global dialogue, highlighting both the shared challenges and the context-specific solutions emerging from Africa. Furthermore, the evidence will help prioritize which models or approaches may be adapted to optimize care according to specific country contexts.
Methods
Review approach
This scoping review was conducted following the Joanna Briggs Institute review reporting format. The protocol was registered on the Open Science Framework (osf.io/np9vq). Findings are presented using a narrative approach.
Review questions
What are the existing practices, frameworks, strategies, models, or approaches related to PC service delivery in Africa?
What advantages and gaps have been documented for the different PC approaches?
What challenges to the implementation of comprehensive PC have been reported?
What suggestions have been made to improve PC delivery?
Population, concept, and context
Population: Adult patients with cancer.
Concept: Approaches (frameworks, models, strategies) implemented to deliver PC and/or to improve the continuum of care across various scopes of PC.
Context: Studies conducted in Africa.
Eligibility criteria
Quantitative, qualitative, and mixed-methods studies, reports, and review articles including systematic reviews and gray literature (such as guidelines, strategies, and policy frameworks) were included. The review considered studies and reports published in English, with no date restrictions. Studies not specific to cancer were excluded; some included broader works in which data were extracted only for cancer-relevant findings. Conference abstracts and studies conducted outside of Africa were excluded.
Search strategy
The search strategy was designed to identify both published and unpublished studies and reports (Annex 1). Initially, a focused search was performed on MEDLINE (PubMed) and Embase to find relevant articles related to the topic. The keywords found in the titles and abstracts of these articles, along with their corresponding index terms, were utilized to create a thorough search strategy for both MEDLINE and Embase. All identified keywords and index terms were then modified for application across each database included in the search. Additionally, the reference lists of all selected sources of evidence were reviewed to determine further studies. The databases searched comprised MEDLINE (PubMed), Embase (Ovid), Web of Science Core Collection, CINAHL, and Scopus. The search for unpublished studies and gray literature encompassed frameworks, and guidelines obtained from Google Scholar, Google, and institutional websites.
Search string
The search strategy was constructed using a combination of Medical Subject Headings (MeSH) and free-text terms. The following keywords were used, grouped into four main concepts and combined using the Boolean operator AND:
Palliative care terms: “Palliative Care [MeSH]” OR “end of life care” OR “supportive care” OR “comprehensive care” OR “holistic care” OR “community-based care” OR “home-based care” OR “facility-based care”
Approach terms: “Framework [MeSH]” OR “model” OR “strategy” OR “approach” OR “guideline”
Cancer terms: “Neoplasm [MeSH]” OR “malignancy” OR “cancer” OR “cervical cancer” OR “breast cancer”
Geographic terms: “Africa [MeSH]” OR the names of all 54 African countries (e.g., “Algeria,” “Ethiopia,” “Tanzania,” “Nigeria,” etc.)
This search strategy was tailored to meet the specific standards of each database included, and it was re-evaluated to confirm that important articles within those databases were successfully identified.
Study selection
After conducting the search, a total of 1242 records were imported into EndNote (version 21), from which 309 duplicates were eliminated. The remaining 933 citations were then uploaded to Rayyan review software for screening. Two reviewers (K.S.D. and N.B.Y.) independently assessed the titles and abstracts of all records. Subsequently, full-text screening was performed on 49 articles by the same reviewers. Any disagreements that arose during either selection phase were addressed through discussions with a third reviewer (N.S.H.). Discrepancies were noted 14 times during the title and abstract screening and 17 times during the full-text review. After resolving these issues, an additional six studies were included in the review. Ultimately, data were extracted from 27 papers and reports. The outcomes of the search and study selection process are illustrated using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Quality appraisal
The Mixed Methods Appraisal Tool (MMAT), version 2018, was used to assess the quality of all included studies (Annex 2). A percentage quality score was calculated for each primary article and interpreted as follows: ⩽50%, low quality; 51%–75%, average quality; and 76%–100%, high quality. Only five low-quality papers were excluded from the review.
Data extraction
Data were extracted from the 27 articles included in the scoping review by two independent reviewers (K.S.D. and N.B.Y.), using a data extraction table developed by the reviewers. The tool was refined after piloting with three studies and incorporating feedback from advisors and then applied consistently across all included studies. The table was designed to capture detailed information across several categories, including existing PC approaches in Africa, associated advantages and gaps, challenges to implementing comprehensive care, and suggestions to improve PC delivery.
Data analysis and presentation
The main findings were presented using a narrative approach and organized according to the review questions of the scoping review. Accordingly, the results were categorized and reported under three main themes: current PC approaches in Africa, challenges affecting implementation, and suggestions to improve PC delivery. Each category was described in detail and supported by tabular presentation.
Findings
Characteristics of the included studies
In total, 1240 citations were identified through database searches. An additional two records were retrieved from institutional websites. After removing 309 duplicates, 933 records were screened by title, with 250 excluded. Based on abstract review, 683 records were screened, and 634 were excluded. The full texts of 49 records were assessed for eligibility; 22 were excluded and 27 were retained for full data extraction. Of the 22 excluded articles, 11 focused on PC within an ineligible concept or content beyond the scope of the objective, 6 were conducted outside Africa, and 5 were excluded due to quality appraisal (Figure 1). The included studies were published between 2002 and 2024. Most papers originated from South Africa, Rwanda, Uganda, Ethiopia, Nigeria, and Kenya. The studies and reports reviewed consisted of 10 qualitative studies, 4 quantitative studies (2 observational and 2 interventional), 2 mixed-methods studies, 2 book chapters, 1 book, 4 reviews, 2 policy briefs, and 2 strategy or guideline documents (Table 1).
List, summary of main finding, and major recommendation from the included studies.

MMAT: Mixed Methods Appraisal Tool; PC: palliative care; HBC: home-based care; NGO: non-governmental organization; ECHO: Extension for Community Healthcare Outcomes.
In this scoping review, we analyzed 27 articles from various African countries and organized the findings into three key categories: an overview of current PC approaches in Africa, challenges affecting comprehensive PC delivery, and suggested measures for improvement.
PC approaches for patients with cancer in Africa
The most commonly reported PC approaches include home-based care (HBC), community-based care (CBC), facility-based care (FBC), integrated PC, and comprehensive or holistic PC (Figure 2). In Africa, PC is characterized by diverse approaches influenced by each country’s unique cultural, economic, and healthcare contexts, which play a critical role in shaping how PC services are delivered and accessed. For instance, cultural beliefs surrounding illness, death, and dying affect patients’ and families’ willingness to engage with PC services.16,17

Palliative care model in Africa.
HBC model
Evidences show that HBC is a commonly reported model for palliative care delivery in Africa.9,17–19
The Kenya Hospice and Palliative Care Association promotes HBC and works to integrate palliative care into the national health system, providing training for healthcare providers. 9 The Palliative Care Institute of Zimbabwe offers HBC services for patients with chronic illnesses, with a focus on caregiver support and training. 18 A network of HBC services has been developed in Uganda to deliver care directly to patients in their homes. 20
In South Africa, the Hospice Palliative Care Association supports hospice services by providing training and resources for HBC. The focus is on pain management, psycho-social support, spiritual care, and care coordination for patients and families. 21
Key aspects of HBC in Ethiopia include offering care at home, allowing patients to remain in a familiar environment; however, palliative care remains primarily donor-dependent and focused in urban areas.13,22
The literature commonly reports family involvement in decision-making and care processes as a feature of HBC. Cost-effectiveness is also described as a characteristic of this model. Mainly reported challenges include limited access to medications, the need for continuous support for caregivers, and difficulties in balancing family needs with medical recommendations.9,19,21 As outlined in Table 2, different service delivery approaches have been implemented to address challenges associated with HBC.
Types and features of HBC approaches in Africa.
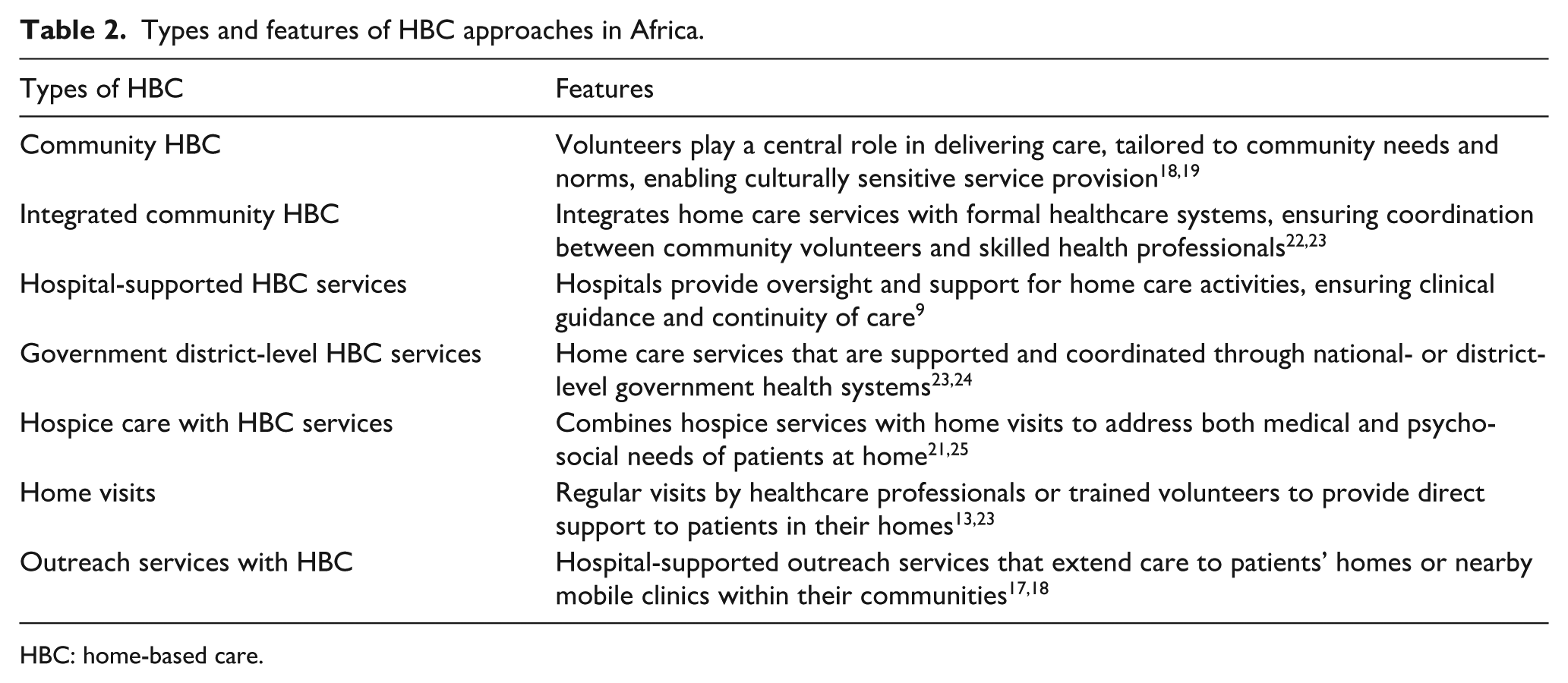
HBC: home-based care.
Community-based care
As the literature shows, trained community health workers play a pivotal role in the delivery of community-based PC, particularly in rural areas where access to specialized healthcare services is limited. This approach also allows for the effective use of local resources. These workers are familiar with the cultural and social dynamics of their communities, enabling them to integrate cultural practices and beliefs into the care they provide. 26 By bringing care closer to home, community-based models reduce the travel burden for patients and families, and facilitate timely interventions that can alleviate suffering. 27 However, the effectiveness of CBC is influenced by several factors: the level of formal training received by community health workers, limited access to opioids, cultural resistance to modern care, weak referral systems between community- and facility-based services, the absence of supportive policies, and the risk of burnout among volunteers or caregivers. Additionally, religious and societal beliefs often shape treatment decisions. 16
In Uganda, CBC extends PC services beyond hospitals through volunteer networks and the involvement of family physicians.19,23 Similarly, in Egypt, the PC model implemented by the Gharbia Cancer Society through the Tanta Project provides support to cancer patients and their families. This example demonstrates the significant role that non-governmental organizations (NGOs) can play in developing community-based PC services integrated within hospital oncology departments. 26
In Rwanda, the CBC model highlights how the presence of community health workers fosters trust and acceptance among patients and families. Care is delivered by individuals who share similar backgrounds and understand local traditions. It was noted that the engagement of community volunteers in the care process led to increased patient satisfaction. 28
In Ghana, community-based PC has been strengthened through the Extension for Community Healthcare Outcomes (ECHO) model. This approach improves access to PC for patients with life-limiting illnesses by enhancing the capacity of healthcare providers to deliver care in community settings. It does so through tele-mentoring, which connects providers for ongoing learning and support. 27
Facility-based care
Facility-based PC models offer a structured environment where healthcare professionals with specialized training deliver PC services. These models facilitate interdisciplinary collaboration among healthcare providers. However, they require significant resources and expertise to manage complex medical conditions and provide advanced symptom relief. Identified gaps in FBC include limited accessibility, concentration in urban areas, inadequate staffing, limited training, high cost, insurance limitations, poor infrastructure, a predominant focus on pain management, and a lack of integration with locally available resources.25,29
At Kenyatta National Hospital in Nairobi, a PC programme has been developed that emphasizes interdisciplinary collaboration, involving teams of doctors, nurses, clinical officers, and social workers working together to manage complex cases. In addition, community outreach programmes have been introduced to raise awareness about the PC services available at the hospital. 9 In Ethiopia, FBC is primarily concentrated in urban areas and includes limited inpatient care. There is little integration with primary healthcare units or HBC services. An exception is Hospice Ethiopia, which refers its clients to public referral hospitals for advanced care.13,25
In Uganda, hospitals provide PC services directly to patients’ homes to reduce unnecessary hospital admissions and improve patients’ quality of life in their preferred environment. Although this model helps to ease the burden on overcrowded hospitals, it remains hospital-led. As such, it may create conflicts of interest in patient management and has been criticized for not fully accommodating the needs of culturally sensitive, CBC. 23
At the Lagos University Teaching Hospital in Nigeria, the Palliative Care Unit supports patients with life-limiting illnesses and their families. Hospital-based care in Nigeria is largely driven by NGOs and focuses on inpatient and outpatient consultations, pain management, home visits, and bereavement support. However, there are no national policies on cancer pain relief or PC, and government involvement remains limited, with low budget allocations to health.29,30
In Sudan, a multidisciplinary hospital-community-based model has been developed. Its scope includes pain and symptom management as well as psychological support. 31
In Tanzania, Selian Hospital provides specialized PC for patients with cancer as part of broader medical care. This includes managing complex cases in collaboration with community resources. The center serves as a referral point for advanced cases and acts as a hub for advocacy, training, policy development, and the provision of specialist PC services. 32
Integrated care models
The integrated PC model offers the advantage of making PC accessible across hospitals, community health centers, and HBC settings (Table 3). These models support continuity of care between inpatient, outpatient, and home-based services. Moreover, integration respects the cultural context of patients, making care more relevant and acceptable to those receiving it.16,33 However, several challenges are associated with implementing integrated care models. These include high costs and limited resources, inaccessibility of opioids at the community level, a shortage of trained professionals, and infrastructural challenges such as insufficient mobile clinics and limited medication availability. Additional challenges include inadequate policy frameworks, unclear referral pathways, and issues with community engagement such as difficulty mobilizing local resources and a shortage of trained volunteers.34,35
Features of PC service integration.
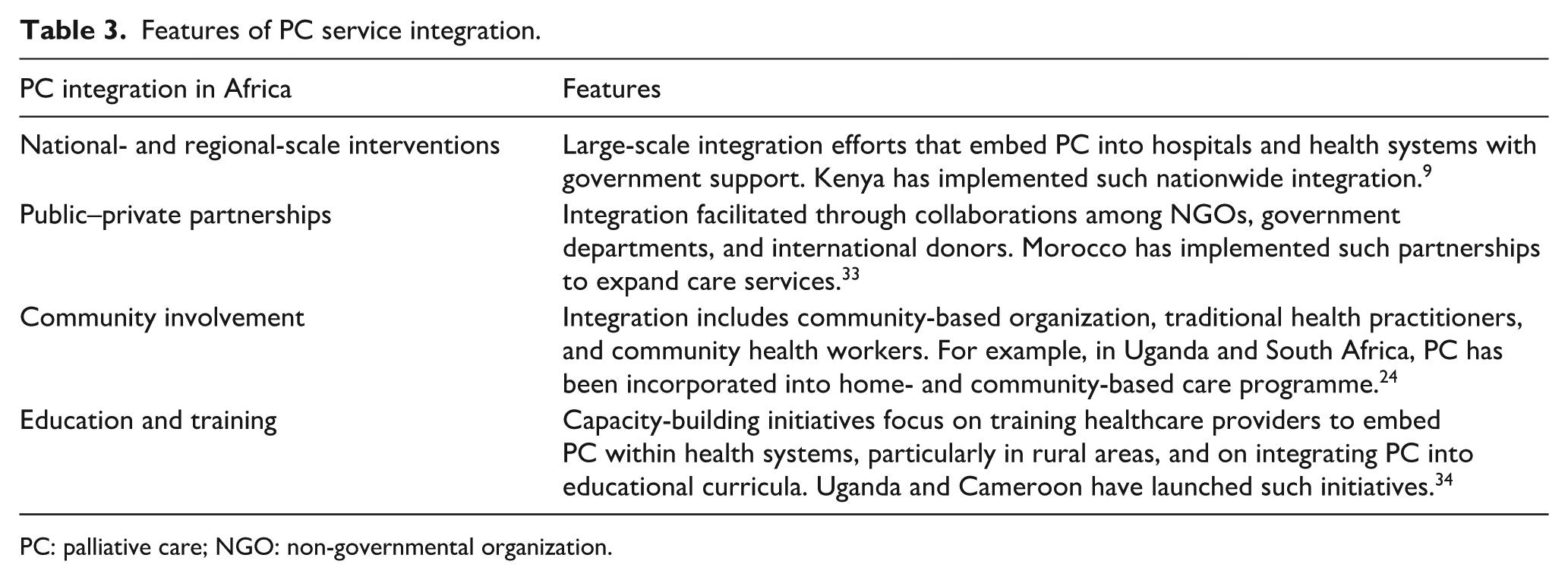
PC: palliative care; NGO: non-governmental organization.
The South African government has recognized PC as an essential component of primary health care. Training programmes have been implemented for healthcare professionals at all levels. Many hospitals have established partnerships with local hospices to provide integrated services that include inpatient care and community outreach.24,35 The Kenyan government has developed guidelines promoting the integration of PC across all levels of the healthcare system. Community health workers have been trained to deliver basic PC services, ensuring that patients receive support at home.16,24,27
Tanzania has implemented an integrated PC model for cancer patients where NGOs have established HBC programme training local volunteers for community support. In Mozambique, integrated care emphasizes collaboration between health facilities and community organization to embed palliative care through training and advocacy. In Zambia, a government-developed national framework supports including palliative care in primary healthcare, engaging local communities to identify patients and facilitate timely referrals. 18
The Cameroon Baptist Convention Health Services launched an integrated care programme with support from Hospice Africa Uganda. This model includes hospital-based care, HBC for patients with advanced cancer, and community outreach. The integration has extended to district hospitals, with the development of mobile teams and dedicated PC units. 34 In Morocco, the National Institute of Oncology has developed integrated care pathways that include PC as part of the overall treatment plan for patients with cancer. These pathways ensure PC services are available from the time of diagnosis and run concurrently with curative treatments. Trained healthcare workers conduct home visits to provide pain management and emotional support, while family members are actively involved in the care process. 33
Comprehensive care model
As studies showed, the comprehensive care model integrates various PC components to address the physical, emotional, social, economic, end-of-life, and spiritual needs of patients and their families, including bereavement support. Community volunteers and primary caregivers are key in providing daily care. As illustrated in Table 4, this model is designed to deliver holistic care by ensuring continuous referral and transition from FBC to HBC.16,36,37 The main challenges to delivering comprehensive care include limited resources, diverse cultural beliefs and practices within communities, the burden placed on family caregivers, restricted access to essential medications, inadequate infrastructure at health facilities to support effective referral pathways, and widespread misconceptions or low levels of awareness about PC.16,25,36
Advantages of comprehensive care approach.

PC: palliative care.
Malawi’s PC model is a comprehensive strategy addressing education, treatment, patient, and family needs through public–NGO partnerships. The model involves training for healthcare professionals and community health workers to deliver services across the care continuum. Its scope covers physical, psycho-social, spiritual, economic, and end-of-life care, with home care teams and NGOs providing holistic, community-based support. The model also facilitates access to essential medicines, including locally produced morphine.9,17
The SAFARI model is a culturally sensitive, comprehensive PC model developed to meet the specific needs of patients and families in Rwanda. SAFARI meaning “journey” in Swahili is based on a Rwandan sociocultural approach that interprets the language of suffering expressed by families and caregivers during family meetings. 38 Each component of the model highlights a holistic approach to PC, recognizing the importance of cultural context, family involvement, and community resources. The model engages family members in decision-making and care-giving, providing them with education and support throughout the illness trajectory. It utilizes community health workers and mobile clinics to reach patients in remote areas and engages local support systems including traditional healers and community-based organizations to complement medical care. It also integrates PC into existing healthcare frameworks, supporting communication between healthcare teams and community resources.37,38
Uganda has developed a comprehensive national policy that emphasizes the integration of holistic PC into the broader healthcare system. This approach addresses psycho-social, spiritual, end-of-life, and economic needs alongside physical symptoms. It is culturally sensitive, promoting the involvement of family members, community volunteers, and traditional healers by incorporating cultural beliefs and practices into care. Structured training programme have been established for healthcare workers including medical students, nurses, and community health workers through continuous professional development in PC.19,23,39
Challenges to comprehensive PC delivery
Lack of awareness and skills among patients and caregivers, misconceptions within communities, and cultural and religious beliefs that influence patients’ preferences and decision-making are encounters arisen from community. For example, strong family ties often lead to expectations for family involvement in care, which can impede the delivery of professional services. Families may prefer home care over FBC, limiting access to structured PC. Additionally, the need for trained care providers who understand diverse religious and cultural practices is critical but often unmet.21,40,41
Health system-related challenges also play a significant role. These include the lack of integration of PC services into existing healthcare systems, unclear referral pathways, and the absence of quality metrics to evaluate the effectiveness of PC and patient outcomes.
The lack of multidisciplinary teams comprising physicians, nurses, social workers, community leaders, and other specialists limits the ability to comprehensively address the physical, psycho-social, spiritual, economic, and end-of-life needs of patients. These challenges obstruct continuity of care, particularly in the transition from FBC to CBC or HBC.13,27,34
Additional challenges reported include the unavailability of essential medications and restrictive laws governing opioid access, the absence of national policies supporting integrated and comprehensive care, and the lack of systems to gather feedback from patients and families to inform service improvement. A further limitation is the scarcity of research initiatives to generate evidence-based practices in PC. The inability to deliver culturally sensitive care tailored to the diverse needs of patients, combined with insufficient government funding, limited resources, and shortages of skilled providers, all contribute to fragmented PC delivery across the region.28,33,35
Suggested measures to improve PC delivery
According to the literature, improving PC delivery for patients with cancer in Africa requires culturally sensitive, community-focused, comprehensive, and integrated approaches that reflect the region’s unique cultural, religious, and social contexts.2,16,24,36
Key recommendations include training healthcare providers in cultural competence to understand and respect the diverse beliefs and practices of patients and their families. Expanding training programmes focused on communication skills, symptom management, and psycho-social support is also essential. Increasing public awareness and engaging local communities in PC education can help reduce stigma associated with cancer and PC services. Further suggestions include providing training and resources for caregivers and integrating traditional healing practices with conventional PC in order to deliver care that aligns with patients’ needs and preferences.13,18,33,39
In addition, advocacy for policies that prioritize PC within national health systems is vital. This includes promoting context-based frameworks or approaches, integrating PC into existing health services, and allocating adequate resources for implementation. Enhancing access to essential medications, including opioids for pain management, through policy reform and improved supply chains has also been emphasized. Furthermore, fostering collaboration among governments, NGOs, and international organization is key to supporting the expansion of PC services and ensuring continuity of care across various settings.23,26,36,37
Discussion
This scoping review highlights existing approaches to PC service delivery across Africa, including hospital-based care, CBC, HBC, integrated PC, and comprehensive PC. The effectiveness of these models varies significantly depending on local resources, cultural beliefs, and healthcare infrastructure. 16 The report reveals that the success or failure of a model often based on its alignment with these contextual factors; for instance, hospital-based models often struggle in resource-poor settings, whereas community-based models can fail without strong local trust and volunteer networks. Overall, the evidence indicates a strong need for comprehensive, integrated, culturally sensitive, and community-focused PC approaches across African regions such as those documented in Uganda, Rwanda, and Malawi26,29,31; others have initiated HBC and CBC to bridge the gap between patients’ needs and formal healthcare systems.23,28,35,37
As the findings revealed, home-based PC is a common approach to cancer care in Africa, offering culturally sensitive, cost-effective solutions that prioritize patient comfort and family involvement.9,18 This highlights the need for targeted strategies to enhance the effectiveness of HBC, such as continuous professional development, resource allocation, and support systems. The success of HBC is linked to strong family structures and the availability of trained community health workers, while its failure is often linked to caregiver burnout and a lack of integrated professional support. These elements are essential to improving the sustainability and impact of HBC across the continent. This also implies that policymakers play a crucial role in shaping the future of HBC in Africa. A number of papers included in this review showed that the CBC model helps optimize healthcare delivery by bringing services closer to home, enhancing patient-centered care, and reducing the travel burden on patients and their families. However, for this approach to be effective, challenges related to limited resources, inadequate training, weak coordination, and insufficient cultural competence must be addressed.27,29,35 The factor determining the outcome of this model is the degree of community ownership and the presence of referral system to facility-based services. This suggests that by tackling these gaps, it is possible to build a more equitable and effective PC system that responds to the diverse needs of patients and caregivers. It also underscores the complexities involved in delivering effective PC, particularly in community and home-based settings.
The facility-based PC model is primarily used to deliver specialized care to patients with serious illnesses. While this model enables interdisciplinary collaboration and provides advanced symptom management, its main limitations are cost-ineffectiveness and restricted accessibility.29–31 This model is effective in urban centers with stable funding and specialist manpower but challenged in rural contexts where infrastructure and travel costs are insufficient. These findings indicate that policymakers and stakeholders should focus on improving accessibility, integrating community resources, and ensuring that PC addresses patients’ holistic needs beyond pain management alone.
As reported, integrated PC models offer significant advantages by improving accessibility, ensuring continuity of care, and respecting the cultural contexts of patients. Nevertheless, challenges such as limited resources, regulatory hurdles, weak policy frameworks, and unclear referral pathways must be addressed to optimize their effectiveness.18,24,25,42 The success of integration is dependent on strong governmental policy and collaboration between different levels of the health system, whereas failure is often a consequence of siloed funding and fragmented health information systems. To enhance the implementation and impact of integrated PC models, stakeholders including policymakers and programme developers should prioritize capacity building, resource mobilization, policy development, and community engagement.
Findings from this review further revealed that the comprehensive care model provides well-rounded support throughout the course of illness by aligning physical, emotional, social, economic, end-of-life, and spiritual needs across settings. Community volunteers and primary caregivers play vital roles in delivering daily care, ensuring that patients receive necessary support in familiar environments.9,23,28,36 This model was shown to enhance quality of life for patients with serious illnesses and their families by providing holistic support that extends beyond the physical. However, its implementation is particularly dependent on context, succeeding only in environments with strong multi-stakeholder coordination and failing where any single component such as spiritual or economic support is neglected due to resource constraints or lack of trained personnel. The approach still faces significant challenges including limited resources, cultural diversity, caregiver burden, regulatory restrictions, poor infrastructure, and low public awareness which must be addressed for its full potential to be realized.13,16,43
The findings also revealed poor PC advocacy, regulatory hurdles, insufficient funding and resources, and a general lack of prioritization of PC within national health systems as major challenges hindering the optimization of holistic care delivery.18,25,36 These issues point to the need for policy reforms aimed at improving supply chains, enhancing resource availability, and developing context-based frameworks to integrate comprehensive PC into existing healthcare structures. Furthermore, the review indicated that factors such as low awareness among healthcare programme designers, providers, communities, and patients as well as cultural stigma surrounding cancer and end-of-life care negatively affect the quality of care.17,25,43 This highlights the need for targeted interventions that promote education and raise awareness about the value and benefits of PC.
Strength and limitation of the study
This study has summarized PC approaches for cancer patients in Africa. The search strategy for this review was limited with keywords and subject headings related to palliative care, supportive care, and end-of-life care, resulting in findings primarily concerning palliative care practices. However, it did not encompass terms that are implicitly connected to palliative care, such as pain management, psycho-oncology, psycho-social support, spiritual care, and bereavement. Future reviews could enhance the breadth and quality of research in Africa by incorporating these related implicit terms.
Conclusion
While WHO defines palliative care as comprehensive care addressing pain, psycho-social, spiritual, economic, end-of-life, and bereavement needs, its scope in most African nations remains largely confined to pain management, delivered through fragmented systems. Our analysis reveals this fragmentation stems not only from known challenges like opioid shortages, under-funding, and weak health system integration but fundamentally from a mismatch between implemented care models and Africa’s sociocultural context. HBC, though culturally resonant, struggles with caregiver burnout and inadequate medical oversight; CBC leverages local trust but is hampered by untrained workers and cultural resistance; FBC offers specialization but is urban-centric and costly. While comprehensive models (e.g., Malawi/Uganda frameworks, Rwanda’s SAFARI) integrating medical and community systems show promise, they often depend on donors and lack scalability.
Continuity and comprehensiveness of PC are challenged by opioid inaccessibility, absence of multidisciplinary teams, poor service integration, unclear referrals, insufficient government funding, lack of research for evidence-based practice, and a lack of culturally sensitive care. Crucially, cultural agency and community capital remain profoundly underutilized pillars. Vital elements like family structures, spiritual traditions, and community volunteers essential for care acceptance are rarely integrated into formal pathways; for instance, religious beliefs dictate treatment choices and family-led decision-making often conflicts with clinical advice, dynamics overlooked in facility-centric models. Aligning care with local concepts of suffering and dignity, while strengthening bidirectional community health system linkages, is key to improving access and acceptability.
Since PC aims to understand lived experiences and extends beyond technical aspects, designing care acknowledging complexity requires co-designing context-specific frameworks with communities to reflect local values, prioritizing caregiver support through respite and financial aid, and advocating policy reforms recognizing PC as a sociocultural intervention not merely medical by mandating cultural competence training and community participation in care. Without addressing these sociocultural dimensions, efforts focused solely on expanding access or opioid availability will fail to deliver holistic PC. Future research must prioritize evaluating community-led models, promoting comprehensive integration as a core national strategy pillar, and developing cost-effective strategies to systematically embed cultural sensitivity across all PC tiers.
To guide such efforts, critical research gaps must be addressed including the systematic evaluation of community-based models of care to build an evidence base for their effectiveness and scalability, the development of cost-effective strategies to integrating cultural protocols and traditional support networks into formal care plans, and the longitudinal study of bidirectional referral pathways between health facilities and community volunteers to facilitate patient navigation and continuity of care.
Footnotes
Annex 1: The search strategy
Acknowledgements
The authors acknowledge Henok Kumsa from Woldia University, Ethiopia for his support in searching articles.
Ethical considerations
As part of the PhD research work, the study was reviewed and approved by the Institutional Review Board (IRB) of the College of Health Sciences (CHS), Addis Ababa University (AAU) with approval number: 064/24/SPH.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: As part of the PhD, this work has been supported by the Network for Oncological Research in Africa (NORA) project, Funding Initiative of the German Federal Ministry of Education and Research (BMBF), Research Networks for Health Innovations in Sub-Saharan Africa (RHISSA), GIZ (Germany) [Funding reference: 01KA2220B], and Research and Excellence in African Capacity to Control and Treat CANcer (REACCT-CAN) project, Science for Africa Foundation to the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) programme [Del-22-008] with support from Wellcome Trust and the UK Foreign, Commonwealth & Development Office and is part of the EDCPT2 programme supported by the European Union.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are within the manuscript, and the complete lists of the studies extracted and analyzed for this study will be available upon the reasonable request of first or corresponding author.