
Abstract
Background:
Wider social networks are increasingly recognized for supporting people with care needs. Health-promoting initiatives around the end of life aim to foster these social connections but currently provide little insight into how willing people are to help neighbours facing support needs.
Objectives:
This study describes how willing people are to help neighbours who need support practically or emotionally, whether there is a difference in willingness depending on the type of support needed and what determines this willingness.
Design:
We applied a cross-sectional survey design.
Methods:
We distributed 4400 questionnaires to a random sample of people aged >15 across four municipalities in Flanders, Belgium. These surveys included attitudinal and experiential questions related to serious illness, caregiving and dying. Respondents rated their willingness (scale of 1–5) to provide support to different neighbours in hypothetical scenarios: (1) an older person in need of assistance and (2) a caregiver of a dying partner.
Results:
A total of 2008 questionnaires were returned (45.6%). The average willingness to support neighbours was 3.41 (case 1) and 3.85 (case 2). Helping with groceries scored highest; cooking and keeping company scored lowest. Factors associated with higher willingness included an optimistic outlook about receiving support from others, family caregiving experience and prior volunteering around serious illness or dying.
Conclusion:
People are generally willing to support their neighbours who need help practically or emotionally, especially when they have prior experience with illness, death or dying and when they felt supported by different groups of people. Community-based models that build support around people with care needs could explore to what extent this willingness translates into durable community support. Initiatives promoting social connection and cohesion around serious illness, caregiving and dying may harness this potential through experiential learning.
Keywords
Background
There is growing recognition of the importance of involving friends, family members and other social connections to support people living in our communities with care needs. 1 Although most family care and support for people with care needs is provided by close family members and friends, wider social networks can be important sources of support as well.2–5 This support is not limited to providing practical help but can also be of an emotional, spiritual or social nature.2,6–8 Care within communities, provided by wider social networks of family, friends, neighbours or volunteers, is increasingly recognized as pivotal to creating sustainable healthcare systems.9,10
Several health-promoting initiatives around people with life-limiting illnesses and people in need of palliative care have emerged in recent years to respond to the challenges associated with serious illness, caregiving, dying and the decreasing proportion of people able to participate in addressing these support needs.10–16 These initiatives often rely on altruism, empathy, a sense of communal responsibility and willingness to engage in supporting others within communities who are facing situations of serious illness, caregiving and loss. Community responses that aim to build capacity around people facing such challenges, defined as public health approaches to palliative care, assign valuable roles to neighbours.17,18 Studying their willingness can explore whether there is indeed a robust foundation from which to build community-based models of support for people confronted with care needs, illness, death or dying.
The literature provides insight into some aspects of people’s willingness to support others in need of support. One study in the Netherlands, for instance, suggested that people are generally willing to help persons with care needs but prefer incidental, instrumental tasks such as grocery shopping. 19 The types of help people commonly provide also differ depending on the relationship the helper has with the help-recipient.4,5,20 Research demonstrated that people are more willing to provide help when they have a close relationship with the person who needs support, when they have a history of (in)formal caregiving or when they are older.4,21 People are less willing to provide help when they are employed, and when they have a higher financial income. 21 While the nature of the relationship between the caregiver and care recipient can be indicative of a caregiver’s willingness to support, several health-promoting initiatives demonstrated interventions that succeed in involving community members outside the support-dependent person’s direct social network as well.22–24
While several studies have thus suggested that people are usually willing to support others in need of support, these studies have focused on kin carers, are limited by their selective or small population samples and have not focused on contexts of serious illness or dying.21,25,26 This focus may influence people’s willingness since the role and representation of death and dying in Western cultures has led to social estrangement from these things, as has been amply described.27,28 Although the involvement and contributions of neighbours in caregiving are recognized in literature,2,6 research on this population remains scarce.4,5,29 Notwithstanding that recent health-promoting initiatives – which rely substantially on the involvement of non-kin carers – report outcomes that promise the fostering of social connections,12,24 the willingness of people living in communities to partake in building these mutually supportive models is still underexplored. In researching this willingness, it is also important to differentiate the types of support people are willing to provide (i.e. practical or emotional). Moreover, we lack any insight into which personal traits and experiences potentially influence or increase such willingness. Researching people’s task preferences to support others contributes to the knowledge base on integrating instrumental and incidental forms of help in the care of individuals with care needs and who are confronted with situations of illness, caregiving and loss.
The research questions of this study are as follows:
(1) How willing are people to provide practical and emotional support to their neighbours in need of support?
(2) Is there a difference in their willingness depending on the type of support tasks?
(3) Are personal characteristics, personal experiences with care, illness and death, religiousness and perceived social support associated with people’s willingness to provide practical and emotional support to their neighbours?
Methods
Design, participants and setting
We applied a cross-sectional survey design and sent a questionnaire to a simple random sample of members of the general public aged 16 years or older in four municipalities in Flanders, Belgium. Two of the municipalities had an urban city centre (Bruges with 118,000 inhabitants and Sint-Niklaas with 80,000 inhabitants) and two were semi-urbanized (Herzele with 18,500 inhabitants and Gavere with 12,000 inhabitants). Bruges and Herzele were selected to be part of a complex public health programme around serious illness, death, dying and bereavement while Sint-Niklaas and Gavere served as control municipalities. The survey was conducted at a baseline moment of the programmes. The protocol of this intervention is published elsewhere and provides more insight into the associated research project. 30 Two other papers of this research studying citizens’ discomfort with someone’s suffering and dying and their palliative care knowledge have previously been published.31,32 The Checklist for Reporting Of Survey Studies (CROSS) was followed to structure this paper (Supplemental Appendix 1). 33
Sampling
A civil servant from each municipality drew a random sample from the local population register. We decided to oversample family carers because the overarching research project focused on serious illness, death, dying and bereavement, which we anticipated would impact this population the most. In Bruges, to increase statistical power for this subgroup, we disproportionately oversampled registered family carers with factor six (i.e. registered in the municipal population to receive financial municipal compensation for family caregiving). This compensation or register did not exist in the other municipalities. The resulting sample from Bruges had an imbalanced age distribution which, together with the oversampling of family carers, was corrected by applying weighting factors ranging between 0.58 and 2.42. 34 Confidence intervals were set at 95% with accuracy at ±5% and heterogeneity at 50%. A conservative estimation for a 35% response rate resulted in a total sample of 4400 individuals from the general public in the four municipalities (1100 each). 35
Data collection procedure
All self-administered questionnaires and accompanying information letters were sent out in the first semester of 2021 via postal mail by the municipalityies’ civil servants and a data collector who was recruited by the research team. We worked with a maximum of three reminder mailings at set time intervals and followed Dillman’s total design method to enhance response rates. 36 If no response was obtained after three reminder mailings or if the potential respondent indicated no desire to participate by contacting the researcher, no further steps were taken. To prevent respondents from receiving an unnecessary reminder, the respondent numbers were collected by the data collector each time a questionnaire was received. Respondents could send the questionnaire via mail using an accompanying pre-paid envelope or had the option to fill out the survey online in Limesurvey using their unique respondent number. Completed questionnaires along with the pseudonymized respondent numbers were received by the researcher, who then communicated these numbers to the data collector. This process ensured that the main researcher remained blinded throughout the entire procedure. None of the people involved in this process could link the respondents’ responses to their names.
Questionnaire and measures
The entire questionnaire related to the topics of illness, death, dying, care and grief and its measures are outlined in the published study protocol. 30 Here, we describe the measures relevant to this study. For some measures in this survey, we used background questions from the Death Literacy Index which had not yet been published when this questionnaire was designed. 37 Several questions asked participants to reflect on their situation prior to the COVID-19 pandemic when answering as answers might otherwise not have been representative (e.g. questions that relate to people being in physical proximity of each other like volunteering, which was not possible due to social distance measures). Informed by prior research, we chose to focus on specific independent variables that relate to people’s personal experiences with care, illness and death as these experiences can increase their knowledge about these topics, therefore potentially impacting their willingness to help neighbours. 38 We were additionally interested in people’s willingness to support others who are not closely related to the caregiver, as a study indicated that the personal relationship between caregiver and recipient impacts willingness. 4 Lastly, expert input and prior research led us to hypothesize that people who feel socially supported by the people in their neighbourhood may experience an increased willingness to contribute to this supportive culture.
Main outcome measure
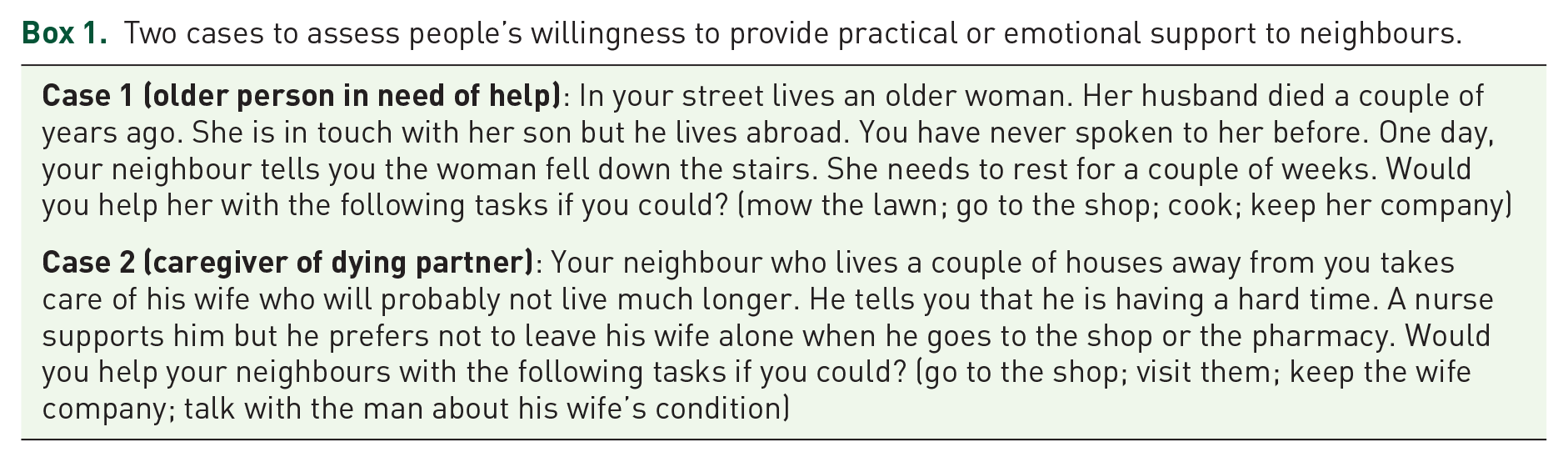
We assessed people’s willingness to provide practical or emotional support to neighbours through two self-developed cases (Box 1). We opted for hypothetical cases to enhance the situation’s recognizability among respondents. Case 1 depicts a person with minimal social support who needs practical and emotional support. Case 2 depicts a neighbour who is a carer for his care-dependent and terminal spouse. These cases allow us to study the possibility of enhancing community involvement coming from the outer social network of people in need of support. 1 Each case proposes four hypothetical types of support. Respondents are asked to indicate how willing they would be to provide each kind of support on a scale ranging from (1) definitely not to (5) definitely.
Two cases to assess people’s willingness to provide practical or emotional support to neighbours.
Demographic characteristics, religiousness and other measures
We asked respondents about their sex, age, working situation, highest degree of education and religious orientation. Since providing care can have important financial consequences for carers, their working situation and the highest degree of education may be relevant measures (since financial income may impact people’s willingness to exchange paid labour for family care). 39
We also asked whether they volunteer, have a chronic illness, are currently mourning the loss of someone or live in a long-term care residence (nursing home, service flat, institution). Lastly, we asked whether people had already undertaken certain actions around their end of life such as having discussed end-of-life preferences with friends or family, or having prepared a will.
We used a validated Dutch translation of the Palliative Care Knowledge Scale (PaCKS) to objectively assess people’s palliative care knowledge. 40 We assessed people’s subjective palliative care knowledge through three self-developed questions. The composition of the PaCKS is found in Supplemental Appendix 2.
We measured how comfortable people feel about the suffering and dying of others. 31 This feeling might impede people’s willingness to help their neighbours when they are confronted with suffering or the end of life. This scale was a non-validated Dutch adaptation of the subscale Dying of Others from the Collett-Lester Fear of Death scale. 41
Personal experiences with care, illness and death
We reasoned that certain personal experiences around the topics of serious illness, death, dying and caregiving could affect people’s willingness to support their neighbours.38,42 Prior experiences with care increase the likelihood that people will care again and change their attitudes on death.5,21 A substantial proportion of people with a professional healthcare background take up an additional family caring task. 43 We additionally asked whether respondents had experience as a family carer, a volunteer around serious illness, death, dying or grief in the year preceding the COVID-19 pandemic’s onset or as a healthcare worker and we asked whether they had ever been with someone else at the time of their death. The variable Cultural exposure to death and dying was composed of two existing questionnaires.37,44 The composition of these variables is found in Supplemental Appendix 2.
Perceived social support
This self-developed measure assessed whether respondents believed they would receive help from others if they fell ill and needed to go to the hospital. The exact composition of this scale is found in Supplemental Appendix 2.
Translation and testing of the questionnaire
The validated measures Cultural exposure to death and dying and PaCKS were translated using the European Organisation for Research and Treatment of Cancer (EORTC) guidelines. 45 Our research team with expertise in end-of-life care and survey development reviewed the entire questionnaire and an external language service checked its language and understandability for sixth-grade level literacy. The questionnaire was cognitively tested once among 15 individuals from the general public to verify its language and its conceptual and face validity.
Data preparation and data analyses
The main outcome measure Willingness to provide practical and emotional support to neighbours has total scores ranging between 8 and 40. These were divided again by eight to facilitate interpretation, resulting in scores ranging from 1 to 5, where higher scores indicate a higher willingness. After consultation with a statistician, we opted to use the factor scores of the main outcome measure for the multivariable analyses examining predictors of willingness since it gave a more satisfactory distribution. 46 Prior to this, we assessed the main outcome measure’s factorial validity. Because of our large sample, a satisfactory subject-to-item ratio of 231.4 was guaranteed. 47 The factor analysis showed all items fall under a single component. An internal consistency test revealed the factor structure to be reliable. Several independent variables represent different types of experiences with care, illness and death (Cultural exposure to death and dying; Having been with someone else at the time of their death; Experience as a family carer; Experience as a volunteer around serious illness, death, dying or grief; and Experience as a healthcare worker). A factor analysis of these variables identified two components but also an unreliable factor structure which is why they are regarded separately. The analyses are found in Tables 1 to 6 in Supplemental Appendix 2.
Missing scores of the responses to the eight items of the main outcome measure were imputed with mean scores. Respondents who answered fewer than six out of eight questions from the main outcome measure were excluded from further analysis (157 cases). Figure 1 presents a summary of the process for obtaining the number of questionnaires used in data analyses. Weighting factors were applied to the data prior to data analyses.

Flowchart of how the final number of used questionnaires was obtained.
To explore whether people’s willingness differs between tasks, we calculated the average willingness scores for each type of support and performed a one-sample T-test. A bivariate correlation analysis explored the correlation between the main outcome measure and respondents’ personal experiences with care, illness and death, demographics, religiosity and other measures. Pearson correlation coefficients were calculated. We also assessed whether people’s discomfort with someone’s suffering and dying is associated with their willingness to support their neighbours. To determine the most appropriate de-confounding strategy (and avoid the so-called ‘table 2 fallacy’), 48 we identified the possible confounders for each of the variables of interest. Next, each of these variables that were statistically significantly (p < 0.05) associated with the dependent variable in the bivariable analysis were entered into multivariable linear regression models, controlling for the right set of confounders.
Results
Of 4400 questionnaires sent out, 2008 were returned (45.6% response rate). Individual response rates per municipality were as follows: 49.7% for Bruges, 44.1% for Sint-Niklaas, 38.3% for Herzele and 42.5% for Gavere.
Characteristics of the study population
The age of the respondents ranged from 16 to 97 and the majority were female (51.2%) (Table 1); 39.8% had obtained a higher education degree. There was a minor non-response observed among certain age groups. Our sample did not show a significant difference between the male–female distribution and the population average. Of all respondents, 52.3% were working, 30.5% were retired and 20.5% had been a family carer in the past. The majority identified with a religious denomination (63.5%).
Characteristics of the study population.
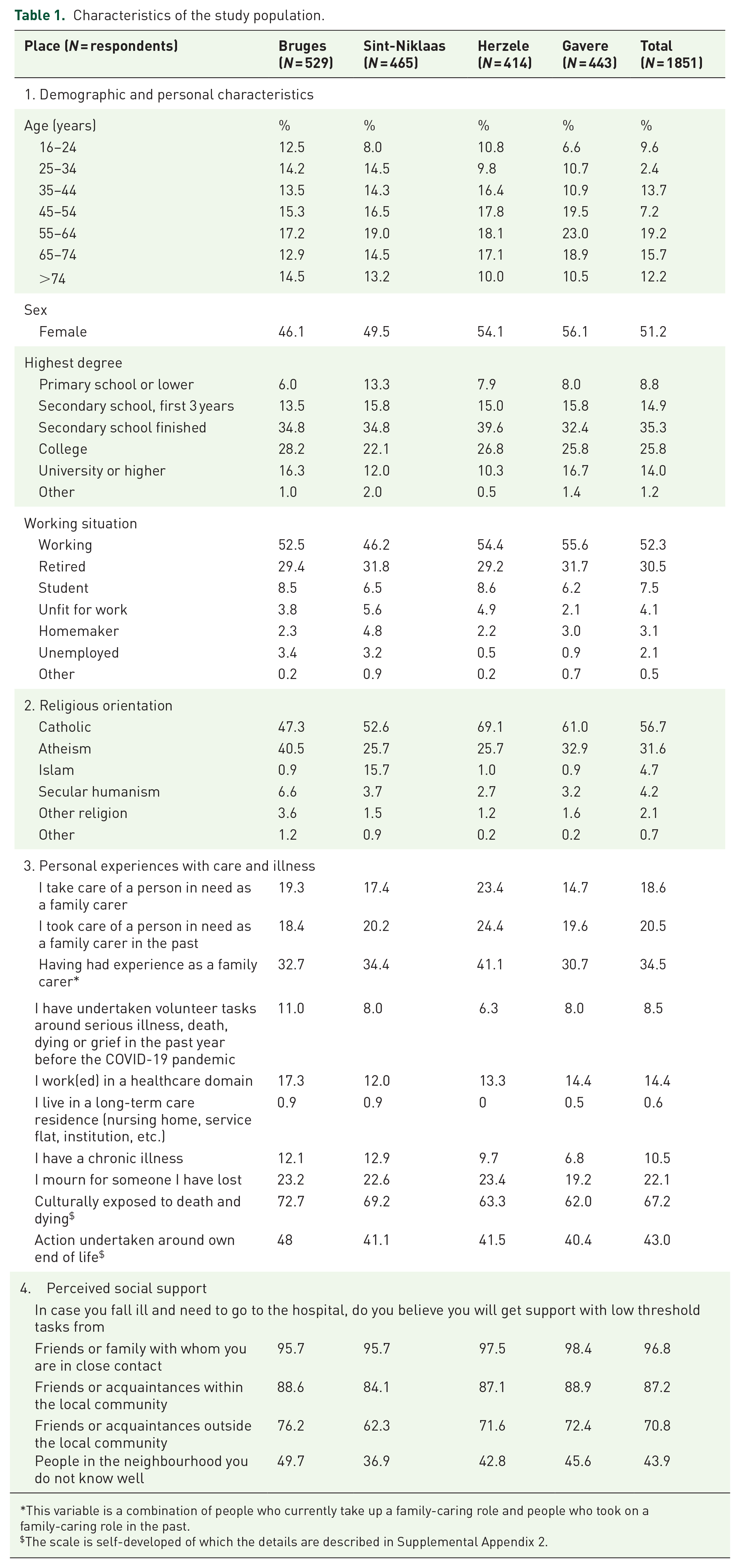
This variable is a combination of people who currently take up a family-caring role and people who took on a family-caring role in the past.
The scale is self-developed of which the details are described in Supplemental Appendix 2.
In the hypothetical case that they became ill and needed help, most respondents (96.8%) believed they would be supported by close friends or family, 87.2% believed they would be supported by acquaintances from their local community, 70.8% by acquaintances from outside their local community and 43.9% believed they would be supported by people they do not know well from their neighbourhood.
How willing are people to provide practical and emotional support to neighbours?
Table 2 presents people’s willingness to help with different types of support in two different cases. The average score on willingness was 3.41 (SD = 1.00) for case 1 (older person in need of help) and 3.85 (SD = 0.95) for case 2 (caregiver of dying partner). For all types of support, except cooking, over half of the respondents indicated that they would probably or definitely be willing to provide this support for their neighbours. In both cases, respondents’ results indicated that willingness was highest for doing groceries (scores of 3.98; SD = 1.11 and 4.12; SD = 1.04). In case 1, cooking for the person in need received the lowest score (3.11; SD = 1.35) while in case 2, the lowest willingness score was obtained in the situation where respondents would have to keep the dying person company (3.59; SD = 1.16).
Willingness of people to provide practical and emotional support to neighbours.

Respondents that filled out a minimum of six out of eight items. 7.8% missing values. Values ranging from 1 (definitely not) to 5 (definitely) with higher scores indicating a higher willingness to provide help.
Depending on the item, missing values lay between 0.4% and 2.9%. Missing data are completely random.
Differences in willingness to provide practical and emotional support to neighbours, depending on the type of support
For both cases, doing groceries was the preferred task (p < 0.001). For case 1, people were more willing to mow the lawn than cook (p < 0.001) and more willing to keep company than cook (p < 0.001). No significant difference was found between mowing the lawn and keeping company. For case 2, people were more willing to go to the shop than to visit them and keep the wife company or talk with the neighbour about his wife’s condition (p < 0.001). People were more willing to talk with the neighbour about his wife’s condition than to visit them or keep the wife company (p < 0.001) and more willing to visit them than to keep the wife company (p < 0.001). These analyses are found in Table 7 in Supplemental Appendix 2.
Factors associated with people’s willingness to provide practical and emotional support to neighbours
Being female, religious, having had personal experiences with care and illness (i.e. being culturally exposed to death and dying; having or having had experience as a family carer or as a volunteer around serious illness, death or dying; having been with someone else at the time of their death), mourning a loss, having experience as a volunteer, having better (self-estimated) knowledge of palliative care and believing they would receive support from others themselves if they fell ill were all associated with scoring higher on willingness. Being older was minimally associated with scoring lower on willingness to support neighbours.
After controlling each variable for their defined set of potential confounders, the multivariable linear regression shows that all significant relationships found in the bivariate correlation analysis remained (Table 3).
Multivariable linear regression analysis of variables associated with people’s willingness to provide practical and emotional support to neighbours.

The following variables which did not have a significant relationship with the main outcome measure in the bivariate correlation analysis were not entered into the multivariable linear regression analysis: Working situation, Highest degree of education, Discomfort with someone’s suffering and dying and Perceived social support from family or others with whom you are in close contact. Controlled for confounding variables: 1Age, sex (female), chronic illness (yes), living in long-term care residence (yes); 2Age, sex (female); 3Age, sex (female), chronic illness (yes), living in long-term care residence (yes), Volunteering around serious illness, death, dying or grief (yes); 4Age, sex (female), chronic illness (yes), Living in long-term care residence (yes), volunteer (yes); 5Age, sex (female), Volunteering around serious illness, death, dying or grief (Yes), Been with someone else at the time of their death (Yes); 6Age, Sex (Female), Volunteering around serious illness, death, dying or grief (Yes), Mourning a loss (Yes); 7Age, Sex (Female), Volunteering around serious illness, death, dying or grief (Yes), Healthcare worker (Yes), Been with someone else at the time of their death (Yes); 8Age, Sex (Female), Living in long-term care residence (Yes).
Discussion
This population-based survey study showed that people are on average willing to support their neighbours in need of help, with different measures being associated with higher willingness. The scores on willingness ranged between 3.11 and 4.12 on a scale from 1 to 5. A higher willingness was associated with being a woman, being religious, having been culturally exposed to death and dying, having had experience as a family carer, working or having worked as a healthcare worker, volunteering in general or volunteering specifically around serious illness, death, dying or grief, having undertaken action around their end of life, having been with someone else at the time of their death, having higher (self-estimated) palliative care knowledge and believing they would receive support from different groups of people if they needed help. People’s working situation, highest educational degree, level of discomfort with someone’s suffering and dying, and whether they felt supported by family or others with whom they are in close contact were not associated with willingness to support.
Some strengths and limitations of this study ought to be considered. The utilization of random samples derived from full population registers in four municipalities allows for statistical generalizability of our findings to these municipalities. However, caution should be exercised when extrapolating these results further to other municipalities or countries, due to diversity in their social and cultural characteristics. Although we achieved relatively high response rates, we cannot exclude the possibility of selection bias as we observed minor discrepancies within different age groups when comparing the age distribution of the responders with that of the population. People who are more socially invested may have been more willing to respond to our questionnaire which also indicates that selection bias may be present. Notwithstanding that both cases and the questions for the main outcome measure are developed by a group of researchers with expertise in community development, public health approaches to palliative care and ageing, we cannot fully ensure the measure Willingness to provide practical and emotional support to neighbours is validated for content. We also cannot exclude measurement bias, caused by social desirability bias for example; however, we can reasonably assume that this bias is less strong for neighbours than it would be for family members or close friends in similar research.4,49 Although the main outcome measure Willingness to provide practical and emotional support to neighbours was self-developed, we assessed its factorial validity and conducted supplementary cognitive testing to enhance content validity and mitigate possible measurement bias. In contrast to many studies on family care, we did specify the types of help that constitute this care.4,50 The cross-sectional study design applied in this research allows exploration of which measures influence people’s willingness but longitudinal designs would be better suited to providing more insight into temporal influences and residual confounding.
The scores on willingness to help neighbours seemed relatively high in the four studied municipalities. Both our cases depict people who live in the neighbourhood of the respondent and need relatively straightforward types of help. Literature indicates that people’s willingness is higher when tasks are short-lasting, less demanding and taking place nearby.25,26,49 Hoefman et al. 19 also suggest that practical support may be considered a public responsibility as opposed to nursing help which is more often seen as a shared responsibility between formal care providers and the care recipient’s inner social network. Research on family care does not always stipulate how this ‘care’ is operationalized, leaving it open to the respondent’s interpretation. 50 This constitutes the already-known phenomenon of carers who do not regard their tasks as divergent from social norms, thereby undervaluing their work and possibly missing out on potential support (i.e. not applying for financial compensation for family carers or preferring to shoulder the burden alone).2,49–51 Additionally, connecting individuals willing to provide support with those in need of care can be challenging when there is uncertainty about the specific support required and how this support needs to be delivered. 51 For communities to make use of the willingness of people to support, we would need to appreciate practical, emotional, spiritual and social support as an integral part of care within and by communities and recognize the added value this creates in the holistic view of both care recipients’ and carers’ health. Indeed, studies have shown that carers experience less caregiving burden when supported by their social network,52,53 which is already a valued strategy in several existing public health interventions.24,53,54
People who had an optimistic outlook about the support they would receive themselves when in need of help were more willing to support their neighbours. This may indicate a perceived reciprocal relationship between community members: if people believe they are supported by their community, their willingness to support their fellow community members increases in return. Our finding that people who believed they would receive support from people outside of their community when in need of help were more willing to help others seems to strengthen this reasoning. The fact that people appear to be willing to support others with support needs adds strength to the community-based strategy applied in health-promoting initiatives around people confronted with illness, death or dying.10–12 The finding that people with experiential exposure related to illness, death or dying exhibited greater willingness to support their neighbours, endorses the broader objective of normalizing the end-of-life stage, as formulated by many health-promoting initiatives within this domain. 12
Population care needs continue to evolve in congruence with the escalating manifestation of chronic illnesses that endure over prolonged periods of time, thereby intensifying the strain on our healthcare systems. 9 Recognizing and establishing community-based care and support as an integral and valued part of our healthcare systems, and an essential approach towards sustainability, may become an imperative strategy. As our research showed that people who were culturally exposed to death and dying or who had volunteered around serious illness, death, dying or grief reported higher willingness, interventions pertaining to these topics may help increase community-based care. Such interventions can help decrease preconceptions and change attitudes about the end of life, thereby reducing barriers that exist for people to support their neighbours.5,55
Conclusion
People are generally willing to provide practical and emotional support to neighbours who need care or support, with their willingness varying between types of support. Women, people with volunteering experience around serious illness, death, dying or grief, with experience as a family carer, and people who expected to be socially supported when in need of help themselves were more willing to help their neighbours. Hence, there may be a large supportive network in neighbourhoods that can be fostered for people who need support. This shows sound potential for the empowerment of people to engage in community-based support models in health-promoting initiatives. Interventions aiming to increase people’s exposure to illness, death and dying, inducing experiential learning, may help build community-based support networks.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241249196 – Supplemental material for Willingness to support neighbours practically or emotionally: a cross-sectional survey among the general public
Supplemental material, sj-docx-1-pcr-10.1177_26323524241249196 for Willingness to support neighbours practically or emotionally: a cross-sectional survey among the general public by Bert Quintiens, Tinne Smets, Kenneth Chambaere, Lieve Van den Block, Luc Deliens and Joachim Cohen in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524241249196 – Supplemental material for Willingness to support neighbours practically or emotionally: a cross-sectional survey among the general public
Supplemental material, sj-docx-2-pcr-10.1177_26323524241249196 for Willingness to support neighbours practically or emotionally: a cross-sectional survey among the general public by Bert Quintiens, Tinne Smets, Kenneth Chambaere, Lieve Van den Block, Luc Deliens and Joachim Cohen in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.