
Abstract
Context:
Death Doulas are working globally to provide non-medical end-of-life care. They have different training experiences and views on the role and whether it should be standardised.
Objective:
To seek the views of organisations responsible for training Death Doulas in order to determine what the drivers are behind this emerging role.
Methods:
We conducted an online survey with Death Doula training organisations in five countries utilising both a targeted and snowball approach. Qualitative analysis was undertaken with themes pre-determined (apriori) due to the nature of the survey categories.
Results:
In total, representatives from 13 organisations in Australia, New Zealand, Sweden, Canada, United Kingdom, and United States responded. The organisations had provided training for 0 to 20 years, with one just starting and another training birth doulas and now expanding. Owners and trainers hold an array of qualifications such as academic, medical, non-medical, and life experience. Curricula have usually been developed locally, and not always included pedagogical consideration, a strategic business model, nor mapping processes such as gap analysis. The organisations are run similarly, and curricula have several consistent topics but with distinctly different approaches. Trainers’ views are also mixed about the way to proceed with registration of the Death Doula role.
Conclusion:
The contrasting views of training organisations explain much of the ambiguity of Death Doulas themselves regarding standardisation of registration, education and role enactment. If heading towards the ultimate goal of professionalisation of the role then a challenging path lies ahead with little in the way of agreement in what this would require.
Introduction
The role of Death Doula (DD) has emerged in recent years, described as a non-medical role and as a supporter/guide/advocate in end-of-life care. 1 Engaged for the most part by patients or families, working to empower them or provide some degree of autonomy, 2 DDs work in varying ways to provide information and support pre-death, during the dying process and after-death. 3 Anecdotally and via social media the role is growing in popularity in Australia, the United Kingdom, the United States, and Canada in particular with a few formal studies undertaken involving DDs in these countries.4–6 Examples of global initiatives that have been published include Indigenous doulas in Canada, 7 and Doulas for unrepresented patients in the United States. 8 The number of DDs working globally is unknown, with some working full-time, but with most more likely to be working part-time as a DD and part-time in another job.2,3 It is only in the last few years that research into the DD role has started to emerge, with our systematic review and a scoping review undertaken more recently, finding little in the formal academic literature regarding the role.1,9 The DD role is unregistered (although regulated in many States in Australia), with no standardised education or training in place or required, which is also true for birth doulas, a role which has been in place for decades.1,5,10
In a survey that we administered to those self-identifying as DDs to enquire about the role, respondents cited some Australian and International DD training organisations that they had studied with. 3 The respondents reported marked differences in the length and type of training and the number of courses undertaken, with 63.9% saying that they did not think that all DDs receive the same training. 3 The DDs also cited different ways in how they work, although arguably as an independent DD they take aspects of their training and use it to individualise their practice, tailored to client needs. It was also noted in the survey that word of mouth was a common way of receiving referrals, so services provided for one family (such as keeping the deceased at home after the death) may be something that they are then known for. 3 Anyone facing end of life, patient or family/carer can engage a DD if they have the means to do so, with a few DDs volunteering their services but for the most part charging a fee to clients.2,3 There are no data to date that provide client satisfaction with DD services, and in our survey, 3 the DDs said that they evaluate their service via anecdotal feedback from clients, by how comfortable the dying person is, by fulfilling the client or families’ wishes, and whether families refer their services to others (unpublished raw data). Our earlier work has provided the foundation for this study.
With the numbers of DDs growing globally DD training organisations are arguably part of the driving force in this evolving industry. Prior research indicates diversity in training experiences, so identifying the background and rationale for different training approaches is important. The aim of this descriptive study was to gather information and perspectives from representatives of DD training organisations across the world.
Methodology
Study ethical approval was obtained from the Flinders University Research Ethics Committee (Project: SBREC7933). The survey invitation was administered electronically via publicly available email addresses and consent was implied on completion of the online form. It was made implicit that organisations could be identified in the process on the Participant Information Sheet, and we asked for their organisations’ name and web address.
We developed a survey based on previous research experience, 3 which we imported into Qualtrics. The online survey contained 20 questions in relation to the organisation’s curriculum, how this was developed, the experience of trainers, and their views on standardised education and registration. Eighteen of these were open-ended questions and 2 were yes/no questions and an opportunity for a general comment was provided at the end. To establish background information, we asked respondents for the name and website address of their organisation, how long they had been providing DD training, how many DDs had they trained and about the qualifications of their trainers. We also asked their reasons for starting the organisation and the process they underwent to establish curriculum. From there we asked about the courses themselves, and how the DDs know they are ready to practice, and on to their thoughts about standardisation and the scope of the role.
From the earlier survey of DDs, participants identified 5 Australian DD training organisations and we included others in Australia and overseas following a Google search. Convenience sampling was employed (as organisations could be easily sourced and recruited), identifying specific organisations that met the inclusion criteria, with all arguably having a vested interest in the outcome. 11
We administered the survey electronically on 4 August 2021 (via the lead researcher’s email) to 15 DD organisations in 5 countries (Australia, New Zealand, Canada, United States and the United Kingdom). All contact details were found in the public domain. Anonymity was not assured as we were asking for organisations to provide identifiers (name of the organisation and URLs for training curriculum); however, we have chosen not to identify them as some organisations commented on others and are certainly identifiable within this small field. With training organisations in this arena potentially unknown, we asked these potential participants to disseminate the survey to other training organisations that they were aware of via a snowballing approach. 12
Study population
Data were extracted from Qualtrics on 30 August 2021 with responses received from 13 organisations, based in Australia (n = 4), United States (n = 4), Canada (n = 2), United Kingdom (n = 1), Sweden (n = 1), and New Zealand (n = 1). From the 15 organisations that we identified and contacted initially, n = 6 (40%) responded. The additional n = 7 organisations were sourced via snowballing approach. There is no way of knowing with certainty who completed each survey, but from responses it appeared that it was the manager/owner.
Data analysis
Due to the categorical nature of the survey questions some of the themes to emerge had been determined apriori. 13 Even so, qualitative data in the form of participant responses were thematically analysed by an independent research assistant using an inductive approach (with participant responses driving the analysis), 13 guided by the concept of grounded theory (theory grounded in the data).14,15
This involved first reading through all responses to a question in detail to derive themes. 13 From there similar words and sections of text were manually grouped under thematic headings using open coding11,16 via a line-by-line analysis of responses, generating a list of concepts. 11 Axial coding was then used to refine the themes further, extending the initial open coding by looking in a more focused way for relationships between concepts.11,16 Exemplar quotes from participant organisations were listed under each thematic heading, giving weight to the relevance of each theme. 16
Results
Background information
Background information was provided on the establishment of the DD training organisation (See Table 1).
Organisation information.
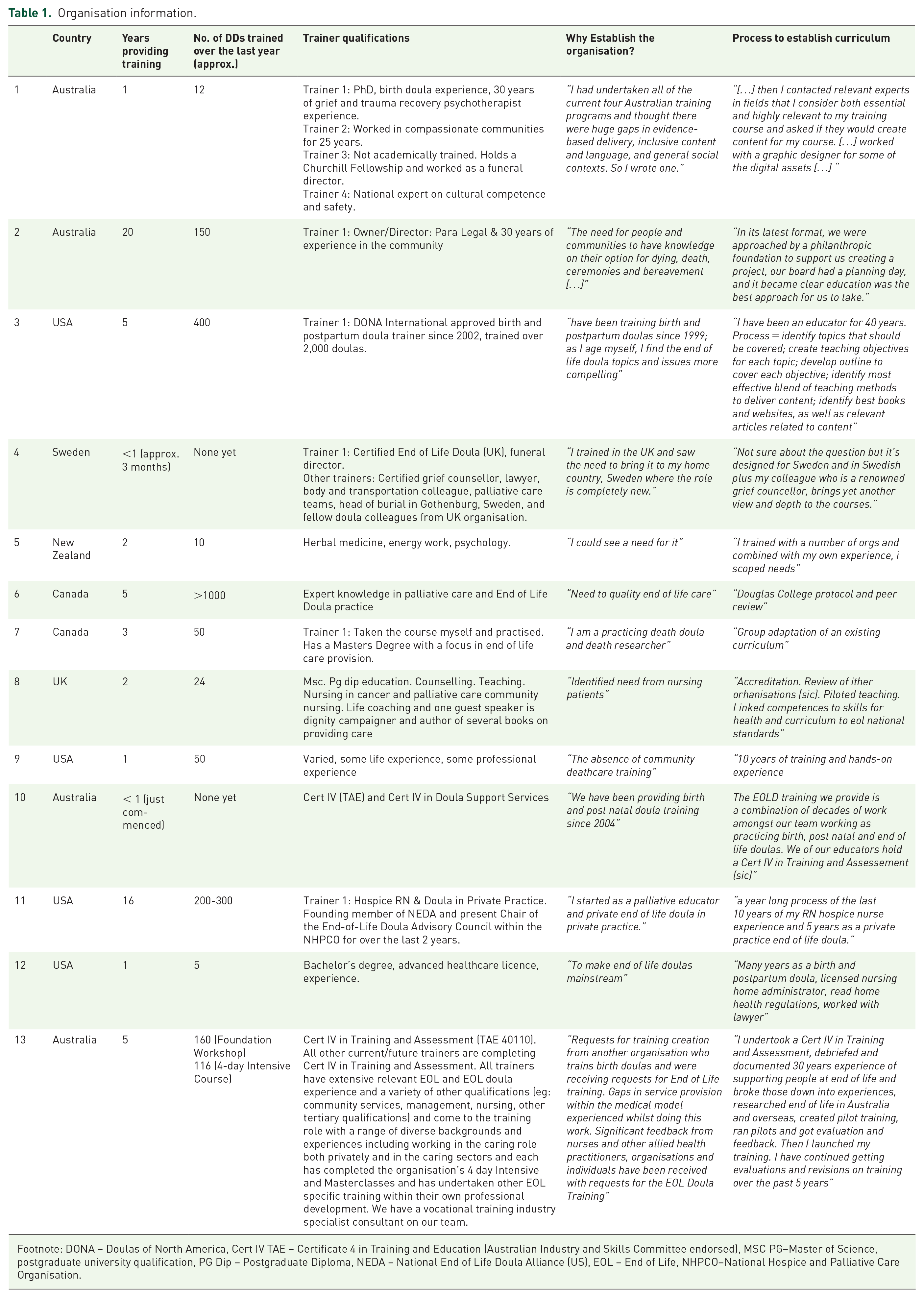
Footnote: DONA – Doulas of North America, Cert IV TAE – Certificate 4 in Training and Education (Australian Industry and Skills Committee endorsed), MSC PG–Master of Science, postgraduate university qualification, PG Dip – Postgraduate Diploma, NEDA – National End of Life Doula Alliance (US), EOL – End of Life, NHPCO–National Hospice and Palliative Care Organisation.
The DD organisations had been training DDs between 0 and 20 years, with one organisation (Org 4) having just commenced training in September 2021, and another (Org 10) having trained birth doulas and now training death doulas. Organisations’ report training between 0 and over 1,000 doulas per year although the latter figure could include birth doulas. With these organisations in existence for up to 20 years the numbers of DDs trained across the globe could be quite significant.
Trainers reported an array of different qualifications and work experiences. This includes academic qualifications (Masters/PhD) and /or health qualification (such as nurse), or a non-health qualification (such as lawyer). Others will have many different experiences, such as those undertaken by trainers (not owners necessarily) including energy work, dignity campaigner and life experience. Many DD training programmes have been established quite recently which again reflects that this is an emerging community response development.
The drivers of DD course development appear to have evolved from individual passion and attracting like-minded people rather than the professionalisation of a role. There was little indication of business model and gap analysis (or it was not reported). Programme development appeared based on personal knowledge in some cases, with very little report of the use of pedagogical frameworks or assessment or outcomes. Without a formal mapping process and contextual curriculum details, it is likely that each training programme is equivalent to Level 2 or Level 3 in the Australian Qualifications Framework (AQF), with level 7 a bachelor’s (undergraduate) degree which HCP will usually study to gain their qualification (e.g. nursing).
Training
Eligibility
Some have no course entry eligibility criteria especially for the foundation or introductory course, one has an age limit (over 18), and others have criminal checks or pre-training surveys to discern the reason for joining. One mentioned postponing training if a recent close death had been experienced.
Course information
The foundation or introductory course could be 5 to 6 hours with most describing their main training course as lasting between 4 and 12 weeks, with one up to a year. It is unknown how many hours this entails as some will be full-time and others part-time. Nine out of 13 organisations provided further training. Overall, organisations stated that foundation courses were a prerequisite to engage in additional training, however it varied as to whether people tended to participate only in the foundation courses or continued on to do further training. All organisations stated that they provided students with a certificate after completing the training which may be the foundation course alone or additional courses. For the most part those completing DD training could start practicing at any time, one respondent stating: ‘They work that out’ (org 2) and another ‘they need to feel ready in themselves’ (org 4), others actively mentor trainees, and two require volunteering in a hospice (orgs 8,9). One required insurance.
Curricula
Each organisation’s curriculum was described, some in detail and others via a few overarching headings, with (n = 7) providing links to their website. As one organization described curriculum as “commercial in confidence/copyrighted” details are subsequently not provided on specific course content but rather via overarching lists. These curriculum content lists show some commonalities such as communication, bereavement /after death care but also individual content such as specific to First Nations people, or about holistic therapies. Information in Table 2 has been sourced from either the organisations’ website (if it was provided in the survey) or from the information provided in the survey (see Table 2).
Death Doula training organisation’s curriculum.

Content
When asked about the similarity of their content to that provided by others, some participants said that they don’t know for sure what the other organisations teach, and one agreed that there is some overlap. What stood out were the points of difference between training content of organisations articulated by some: My point of difference is a very broad and deep cultural, historical and social set of contexts, evidence-based information, a social science background in combination with psychotherapy training and practice [. . .] As far as I know I am the only end of life trainer to discuss sex and sexuality at end of life and to be as comprehensive and inclusive as I am. (org 1) Mine is an expanded concept of the role of the EOLD. Encouraged to be involved further upstream of active dying process, even with Advance Care Planning when folks are well. I also include training in how to be self-employed and create a doula business. (org 3) [. . .] but mine also reaches back into renaissance and ancient greek ways of caring for the whole person. Nature and connection to nature is also central to my approach’ (org 5) ‘We do have more practical business application. (org 7) Additional validated cerificates (sic). Grounded in national standards and competences but bkended (sic) with a non biomedical model. (org 8) I do not teach deathcare with an emphasis on “professional” or how to make money at caring for the dying and dead. That is the major difference!. (org 9) I dont (sic) know of any training that is comparable to mine. I’m not being an ass, just truthful. I have a unique perspective on palliative care, hospice care, private practice. (org 11)
No, we are training specifically for our company policy, procedures, trade secrets, team-based care and do things differently than a solo doula. (org 12)
We are wholly EOL focussed and dedicated. We now have a Government accredited Certificate IV in End of Life Doula Services [. . .] Our after death training was developed in collaboration and under the ongoing guidance of Natural Grace holistic funeral directors. (org 13)
Points of difference in curricula were fiercely defended and ranged from the personal unique perspective to the professional, citing government accreditation and an evidence base.
Standardisation
We asked participants’ thoughts on a standardised (National or International) education curriculum for Death Doula training, with themes in their responses shown (Table 3), reflecting various subthemes: that current training varies widely, no room for specialization, in favor of standardised curricula, against standardised curricula, unsure, alternatives to standardisation, importance for insurance and reassurance for the community.
Views on standardised education.
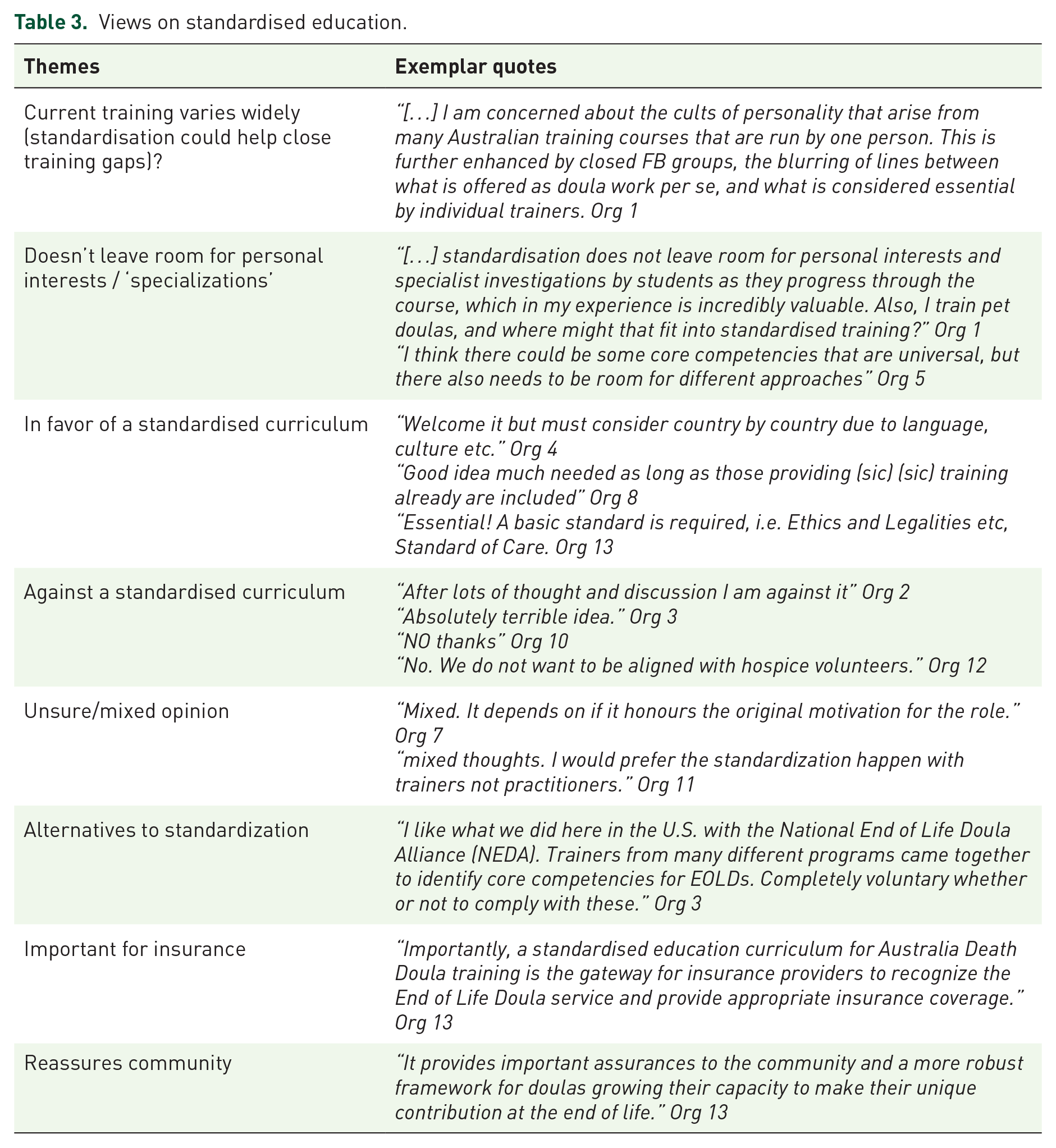
Of n = 13 DD training organisations n = 4 answered ‘No’ in regards to standardised training, n = 3 had mixed feelings, n = 2 did not answer and n = 3 said ‘yes’, but had caveats to this occurring. One organisation did not provide an answer that addressed the question.
Registration
We asked participants’ thoughts on registration for Doulas via a peak body (a board for example) (See Table 4).
Views on registration for DD.

In terms of registration n = 5 answered No, n = 2 did not answer, n = 1 was not sure that the sector is ready, and n = 5 said yes with one of these adding a caveat.
Voluntary assisted dying (VAD)
Participants were asked whether they see a role for Death Doulas in Voluntary Assisted Dying. The majority of participants (n = 11, 86.41%) said yes to this question citing it as a part of care of the dying. One participant had already experienced this type of care working in Victoria, Australia: The manifestation of that personal agency at end of life can be greatly enhanced by the presence of an end of life doula who is independent of the family, familiar with the process (increasingly so as VAD is taken up) and providing instrumental practical and emotional support direct to the person in all settings. There is little difference from non VAD [. . .] I have worked with 2 families in this space that are from VIC and looking forward to supporting families in other states as their laws change. (org 13)
However, there were some caveats: One of education and support for the dying person and their loved ones, yes. Direct involvement in the process, no, as that would be a violation of scope of practice. Also, it will confuse consumers overall if the profession becomes conflated with assisted dying. (org 3) Yes where this is legislated. (org 8)
One organisation was not ready to answer yet and one (below) said no: I would not suggest it. I have had many conversations with leaders and it would be best to me if the people who companion through MAID be volunteers of the org that is supporting the family. and if that person is also a doula, they not mix it up in their services but rather state they volunteer with so and so. that they never charge for that support. (org 11)
NB: MAiD is Medical Assistance in Dying – terminology used in United States and Canada
Discussion
Results from this survey demonstrate diversity in the views of DD training organisation operators regarding training, education, regulation, and standardisation of the DD role. Despite being offered for some years, DD training is not accredited, standardised nor formalized in Australia nor overseas. There are an increasing number of DD training organisations, 2 each with their own unique view on what is to be included in the curriculum. We can see these training organisations in the media (such as those we found on a Google search), in tandem with a plethora of radio interviews, television appearances, podcasts and local directories with DD listings, all of which are helping to normalize this role in the public domain, albeit with a limited assessment of consumer need and understanding of the impact of different approaches and services.1,9
Training
The diverse views, training experience, and knowledge of what training other DDs receive that were seen in our first DD survey in 2019, 3 may reflect the diversity in views of the organisations that train them as seen in the current study. Krawczyk and Rush, 5 highlight this heterogeneity, saying their DD participants celebrated the diversity of the role, but arguably without consideration of the impact of multiple DDs practicing without accord or consensus, contributing to the complexity of potentially coming together via standardisation in practice. Mallon 17 says that approaches to practice and standardisation are in progress, which is starting to be seen in Australia, although with what Young (2021), 18 calls ‘professional ambivalence’. Young 18 uses birth doulas as an example, as they continue to ‘navigate uncertain terrain of their emerging occupation’ (p. 306), across several decades, and DDs may be destined to follow the same path. 18 The professionalisation of the DD role, while still controversial within the DD arena, can also be seen as a way in which to help define the DD role within healthcare, such as in hospital and hospice and to legitimize it. 8 However, not all DD see this integration in a positive light, asserting that their role is independent and should remain so. 9
The professional ambivalence of DDs appears to be marked by their desire to avoid medicalization of death and dying with the emphasis on the non-medical ‘care work’, 18 in what Francis 6 has termed the ‘personal service industry’. However, this is countered by a drive to be acknowledged as worthy by health professionals in seeking authenticity via qualifications or professional legitimacy. 6 In our previous study, tensions were identified by DDs in interviews where they described that: Health Care Professionals (HCPs) don’t understand their work, that some feel threatened by them, that some are fundamentally opposed to the role, with a few HCP actually quite scathing in their views. 4 However, it should be noted that there are HCPs who do in fact refer patients to DDs. 3 Page and Husain 2 recognize that there are barriers to gaining recognition and acceptance, citing the birth doula movement as a forerunner in this area.
There is diversity in the qualifications of the trainers employed by organisations, and it is important to distinguish between qualifications which identify academic expertise and qualifications relating to relevance or life experience. Relative to this, the drivers of DD course development appear to have evolved from individual passion such as noting a gap in what the owner felt was lacking, and attracting like-minded people, rather than the planned development and professionalisation of a role. 18 There was little indication of a business model in development of the organisations even as some organisations teach DDs about establishing their own business. Most curricula appear to be based on personal knowledge with some descriptions of evidence-based content but little report of the use of pedagogical frameworks, with a diversity in approaches and expectations.
Krawczyk and Rush 5 in their interviews with DDs found that the majority of their participants were able to outline different training models. However, in the current study of DD training organisations, we found that providers did not always know what other organisations offered but did think that commonalities occurred. In our previous survey of DDs, 3 nearly a fifth of respondents took more than one course and others took more than 3 courses which arguably would then allow them to see similarities and differences. This may also suggest that DDs take several courses as no single DD course meets all of their needs.
Registration
When questioned on their views of DD registration and standardised training going forward, respondents had quite polarized views. It is unsurprising then that this mirrors our findings in the 2018 survey of DD themselves with respondents quite divided, and in that study also reflective of the general consensus of uncertainly or equivocation nearly a third were neutral. 3 A lack of core competencies for DDs and a lack of requirement for registration with a peak body remains a major gap when there is the expectation that people in the community will pay for this service; however, we note that both are currently being explored in Australia.
Voluntary assisted dying
Voluntary assisted dying (VAD) is currently legislated in many, but not all, states and territories in Australia as well as in many countries overseas. 19 The majority of our respondents were in favor of being present with someone who was accessing VAD (or MAiD) and as DDs are engaged by the dying person and their family, this could foreseeably be within their remit. Maintaining the non-medical role throughout was emphasized by at least one respondent though, and this distinction may be the difference between views of HCPs who are required to be more actively involved (such as medical specialists) and who may not be willing to take this role on.19,20
Strengths and limitations
This is the first study internationally to source the views of organisations that train and support DDs, and we were successful in gaining input from DD organisations in 6 different countries. Nonetheless, we are aware of the possibility of social desirability in responses, 21 especially as anonymity was not guaranteed. This in itself could also speak to motivation in that while participants willingly contributed to the further development of DD training (i.e. self-selected), they would also be visible in their contributions. Alternatively, it could have prevented participation if organisations did not wish to be identified. It is also unknown how DD training organisations who did not respond or participate would differ from those who did.
Conclusion
Independent organisations are driving the DD movement by laying foundations in terms of philosophies, approaches, knowledge and recommendations for practice. The development of each organisation appears to be based on personal perspectives, with variations in how the organisation evolved, the pedagogy or evidence base behind curricula development, the qualifications of trainers, and aspects of the curricula. The visibility of the death doula role in the media driven in part by the training organizations is normalizing the role, providing pseudo-legitimation in the absence of any formalized national or international processes for registration and standardisation of education delivery. Our empirical research has focused a spotlight on this lack of consensus on these requirements, highlighting the polarized views of those involved.
There remain implications for those working alongside a DD and those who engage them, as transparency in what a DD offers is vital for potential clients/consumers and health care professionals alike. The DD training organisations will drive the professionalisation of the role, although this is likely to happen in the background to a sector where the number of DD training organisations and indeed DDs are growing significantly.