
Abstract
Background:
Healthcare professionals trained in palliative care (PC) improve satisfaction and decrease healthcare overutilization for patients with serious illness and their families. A continuing education (CE) series on primary PC aligned to the National Clinical Practice Guidelines for Quality PC was developed by local, interdisciplinary experts for a target audience of rural, primary care healthcare professionals. The modules were accessed on an online learning management system platform.
Objective:
The study objectives were to assess differences in participants’ knowledge, competence, performance, and ability to improve patient care as well as commitment to change practice after taking each of the CE modules.
Design and Methods:
To achieve these objectives, a descriptive design was used with a convenience sample of healthcare professionals who registered for the CE series and completed at least one module. Participants completed demographic questions and an evaluation survey after completing each module.
Results:
So far, 158 healthcare professionals have registered for the series with the majority being nurses and social workers. Although the professionals reported having extensive healthcare experience, they did not report having the same level of PC experience. The professionals represent nine different states. All the CE modules increased teamwork skills for most participants. The CE modules on cultural aspects and self-care had the biggest influence on participants’ ability to improve patient outcomes. Cultural aspects, care of the actively dying, and advance care planning had the greatest impact on participants’ knowledge, competence, and performance.
Conclusion:
The primary PC education series improved self-reported skills in teamwork, practice habits, and meeting goals of healthcare professionals from a variety of disciplines and settings. These enhanced primary PC skills will improve the incorporation of PC into a variety of practice settings, by multiple disciplines to enhance access to PC outside of, and potentially referrals to, specialty PC programs.
Palliative care (PC) is an emerging field of healthcare aimed at positively affecting patients living with serious illness and their families. An important factor that influences a health professional’s successful delivery of PC may be their knowledge, experiences, and confidence. PC training provided to healthcare professionals improves patients’ and healthcare professionals’ satisfaction and reduces healthcare expenditures through cost savings and cost avoidance.1,2
Background
Primary care clinics are often the first point of contact in managing patients living with serious illness. The healthcare professionals often have developed long-term relationships and know the family and background of the patients; this is particularly true in the rural settings. 3 Rural residents have less access to specialty PC services when compared with urban residents.4,5 At times, healthcare professionals in rural regions must coordinate with specialty professionals to manage more complex or difficult cases. This is especially true for patients living with serious illness given the complexity associated with identifying resources to assist with coordination of care in a rural setting. Common challenges are specialty professionals not being familiar with local resources and patients traveling great distances to access resources. 6
Continuing professional development is a responsibility of all healthcare professionals; however, there are many barriers impacting rural healthcare professionals’ ability to obtain necessary continuing education (CE). These barriers include long travel distances to attend education modules, geographic isolation, lack of financial support, and inadequate staffing. 7 The coronavirus disease 2019 (COVID-19) pandemic further highlighted the difficulty in obtaining adequate CE with limited face-to-face education opportunities available; thus, healthcare professionals were prompted to seek online training and education to meet the requirements of their profession. 4
In 2018, the South Dakota Palliative Care Network (SDPCN) conducted focus groups with healthcare professionals, patients, and families across the state of South Dakota to better understand the perceptions and needs of PC, especially in rural areas. A key finding of this study was that many patients, families, and healthcare professionals do not understand PC and how it differs from hospice care. 8 To address this finding, the SDPCN received a Rural Health Network Development (RHND) grant which pulled together partners from clinical practice and academia to focus on increasing PC awareness and knowledge 9 with a consistent approach and message, including a standard definition. The first step was the collaborative development of 11 free, online learning modules for CE focusing on primary PC. Primary PC is defined as ‘Palliative care that is delivered by health care professionals who are not palliative care specialists . . . [and] are not certified in palliative care’. 10
Primary care clinicians must be competent in primary PC skills 11 and have a duty to provide primary PC wherever they practice. 12 Primary PC skills are best learned from those who are trained and work as part of a specialty PC team. Fellowship trained physicians, certified advanced practice providers, and their team members have additional knowledge, skill, and expertise in the care of patients living with serious illness and their families. In challenging the norm of offering education only in a face-to-face setting, the RHND grant allowed the project team to develop and offer online CE modules. Participation included CE credits for multiple disciplines and access to additional resources.
Development of the continuing education series
A CE planning committee was formed to meet the requirements of Joint Accreditation Standards for Interprofessional Continuing Education, 13 including representation from multiple disciplines, a variety of practice locations, and different health systems. With a goal of creating accessible, high-quality education, the CE modules were created for rural, primary care healthcare professionals wanting to learn about PC. A significant need for PC training was identified, as PC delivery lacks consistency when incorporated into primary care. The professional practice gaps identified for current healthcare professionals were not knowing:
The difference between PC and hospice.
What benefits PC can provide patients and families.
Having the knowledge and skills to incorporate PC into primary care.
To determine the best design for the educational series on primary PC addressing the mentioned practice gaps, the CE planning committee identified three necessary items for the education: (1) Recruit local experts in the topic area to ensure applicability to the state’s frontier and rural areas; (2) Complete disclosures to mitigate conflicts of interest; and (3) Develop evidence-based education. The committee decided to base the CE series on the latest edition of the National Consensus Project Clinical Practice Guidelines for Quality PC 4th ed (NCP Guidelines). 12 The CE planning committee also determined the large-scale education series desired it to be available from a single access site versus education scattered among the individual member organizations would be most impactful. Using the framework of the eight domains from the clinical practice guidelines, 12 the content was divided into CE modules that were approximately 1 h in length. With the intent of creating education relevant for several healthcare disciplines, the type of CE credit offered varied based on the professions the education was targeted to reach (Table 1).
CE module descriptions for primary PC series.

PC, palliative care; MSW, master of social work; CSW-PIP, certified social worker in private, independent practice.
The initial educational delivery design was to have live presentations which would be recorded and available for on-demand learning on an online learning management system (LMS) platform. This decision to offer online on-demand education delivery was changed due to the geographical area of the target audience, which represents the entire state of South Dakota as well as the financial and time constraints it would put on facilities to offer live modules for in-person learning. In addition, the large geographical distances from urban facilities to rural facilities with content experts continued to justify the value of online education delivery.
The goal of the CE planning committee was to have the first live session by July 2021; however, the COVID-19 pandemic offered additional constraints. The presenter for the first session was rescheduled multiple times due to practice obligations. Due to the new demand COVID-19 had placed on healthcare, the planning committee pivoted how the education was going to be offered. Instead of having both live and on-demand education, the change was made to only offer online on-demand education as it allows for the greatest flexibility for speakers as well as the greatest access for the healthcare professionals. The first education offering in the series was launched on 15 September 2021. Ultimately, 10 additional modules were recorded and placed on the LMS platform and offered at no cost with open access at any time for healthcare professionals who want to learn more about primary PC.
An important part of the educational evaluation was functionality of learning and evaluation, which is measured by the commitment to change evaluation section. This evaluation section provides information regarding what participants learn right away and long-term changes participants plan to make to their practice or approach to practice and ultimately, if successful incorporation of those changes into their practice.
Once education was created, the next step was making others aware of the free educational series. Marketing the series started through the SDPCN quarterly newsletter to over 250 members. Marketing was augmented by the directors of the SDPCN presenting to almost 1000 people in the upper Midwest and the CE planning committee members sharing through their own networks, key collaborators in PC, and healthcare settings. The opportunities to share the PC education series expanded as the network grew and the number of available CE modules increased throughout the study.
Objective
The study objectives were to assess differences in participants’ knowledge, competence, performance, and ability to improve patient care as well as commitment to change practice after taking each of the CE modules.
Design and methods
A descriptive research design was conducted to achieve these objectives. A convenience sample of healthcare professionals who registered and completed at least one CE module within the primary PC education series was utilized. The study was determined to be exempt by the Institutional Review Board at the health system that manages the LMS platform.
To meet the Joint Accreditation Standards for Interprofessional Continuing Education, 13 the post-evaluation survey completed by participants is a standardized survey template required by the CE department. Based on approximately 12,000 participants per year, the survey questions are analyzed by the CE department annually for continuous improvement. The evaluation survey assesses: (1) Effect on teamwork skills (5-point Likert-type scale from Strongly Agree to Strongly Disagree); (2) Change in knowledge, competence, performance, and ability to improve patient outcomes (Answer choices are: No change, No, Yes); and (3) Meeting professional and personal goals as well as influence on practice habits (5-point Likert-type scale from Strongly Agree to Strongly Disagree). Learners are also able to enter comments at the end of the evaluation survey (see Appendix 1).
Data collection
Within the LMS platform, learners were required to register once for the series rather than for each CE module to prevent duplication of data. The registration form contained demographic questions and permission to use their de-identified data in this study (see Appendix 1). Upon completion of the registration form, the learner was sent a code which allowed them to take all CE modules. This code was sent to each learner whether or not they gave permission for their data to be used in this study. Individual CE modules cannot be taken unless they have the code and have registered for the series which facilitated collection of data.
After completion of each CE module, a post-evaluation survey is available to the learner within the CE portal. To earn CE credits, the learner must take this post-evaluation survey, aiding data collection. As part of the initial evaluation, learners identify what changes to their practice they anticipate making and how long it will take to implement. The second phase of evaluation was not required to be completed for the learner to be awarded CE credit. This phase entailed learners being able to select 30, 60, or 90 days at which time the long-term survey was sent to identify what changes to their practice they were able to successfully implement or what barriers they encountered in doing so.
Data analysis
The data for this study were exported from the LMS platform and analyzed for descriptive statistics. The evaluation comments were read for exemplars and constructive feedback of the CE series. Only data from learners who gave permission for their de-identified data to be used in this study were analyzed.
Results
For the period of 15 September 2021 to 30 December 2022, 158 healthcare professionals registered to participate in the primary PC education series. Most of the healthcare professionals were nurses [licensed practical nurses (LPNs), registered nurses (RNs), advanced practice registered nurses (APRNs)] and social workers who worked for the health system that manages the online LMS and practiced in a hospital or clinic setting. The healthcare professionals were mainly Caucasian and 25–44 years old. While 55% of the healthcare professionals reported having 10 years or more of healthcare experience, only 23% reported having 10 years or more of palliative and end-of-life care experience (see Table 2).
CE series registrants’ demographics.

CE, continuing education; EOL, end of life; PC, palliative care; APP, advanced practice provider.
When the healthcare professionals registered for the series, they entered their zip codes which were analyzed to determine the geographical impact of the CE series. Participants were from nine states in the United States (see Figure 1).

States represented by the healthcare professional participants.
To discover the rural and frontier versus urban locations of the participants, zip codes of the participants from South Dakota were grouped according to the state’s 66 counties (see Figure 2). The state is made up of 66 counties. Participants represented 3 urban, 17 of the 25 rural, and 6 of the 38 frontier counties in the state.

Counties in South Dakota represented by the healthcare professional participants.
Participation in the various modules varied and has been impacted based on how long the module has been available on the LMS platform. The first module to be available on the LMS platform was What is Palliative Care?, which has had the most participation with 76 participants. The next 10 modules became available over the subsequent 10 months with varying numbers of registration and completions of the evaluation (see Table 3).
Number of participants and evaluations per CE module.
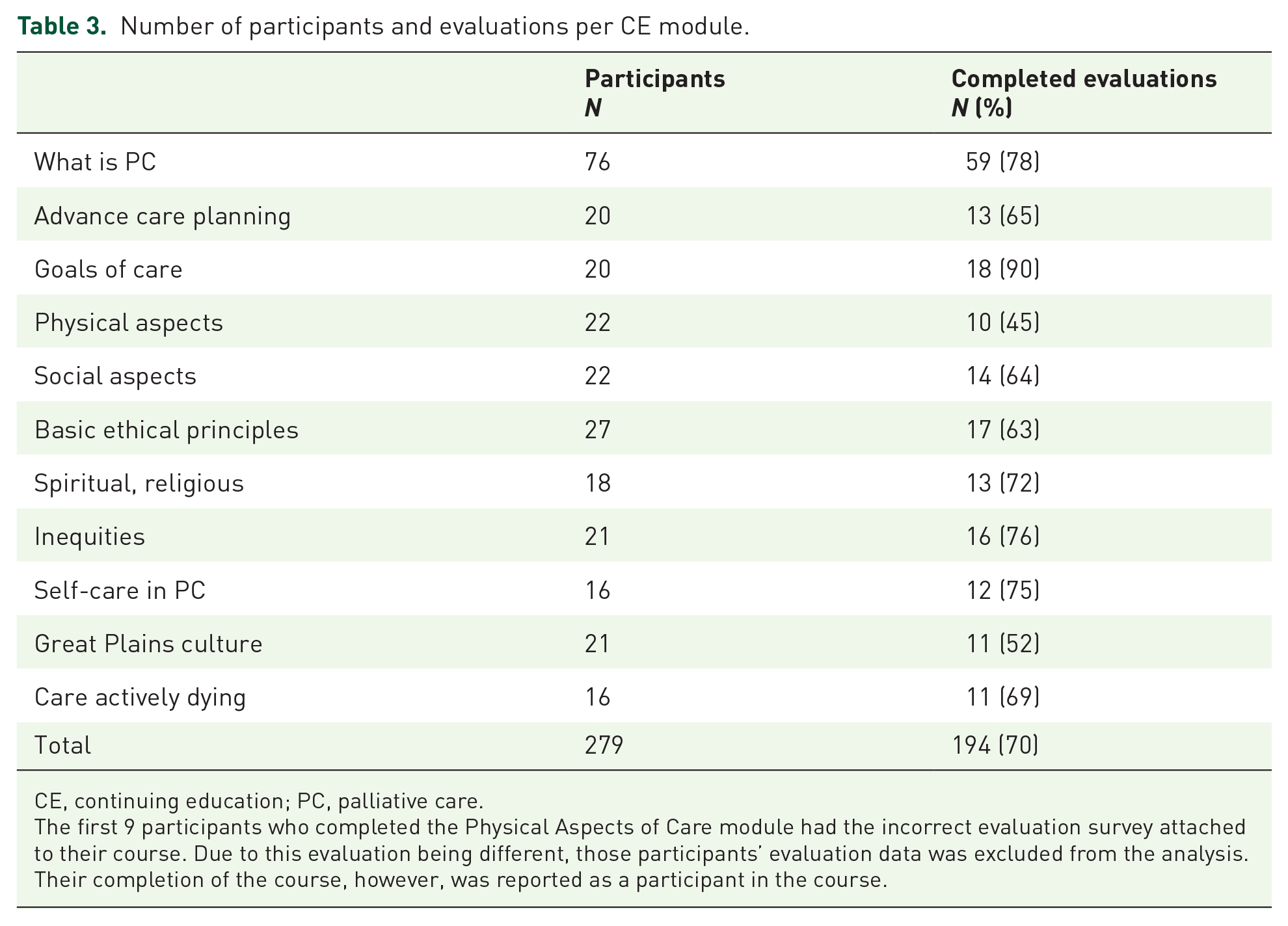
CE, continuing education; PC, palliative care.
The first 9 participants who completed the Physical Aspects of Care module had the incorrect evaluation survey attached to their course. Due to this evaluation being different, those participants’ evaluation data was excluded from the analysis. Their completion of the course, however, was reported as a participant in the course.
Teamwork skills were positively impacted by the CE series with 90% or more of the participants indicating these skills increased due to the education. While an unanticipated finding, it is a key finding since quality PC is delivered by an interdisciplinary care team. Table 4 shows participants who indicated they strongly agreed or agreed the CE module enhanced their teamwork skills. Most participants reported being able to apply what they learned in the module to work in a team environment, which included being better able to collaborate and communicate with multidisciplinary teams as well as state how teamwork contributes to patient care.
Impact of education on teamwork.

PC, palliative care.
The CE module on Great Plains Native American Culture demonstrated the greatest impact on participants’ self-reported increase of knowledge, competence, and performance as well as ability to improve patient outcomes. The second highest impact in participants’ self-reported increase of knowledge, competence, and performance was related to the CE module on Care of the Actively Dying, followed by Advance Care Planning. The CE module on Self-Care showed the second greatest impact on participants’ self-reported ability to improve patient outcomes followed by Advance Care Planning and Spiritual/Religious Aspects of Care (see Table 5).
Impact of education on self-reported clinical performance.
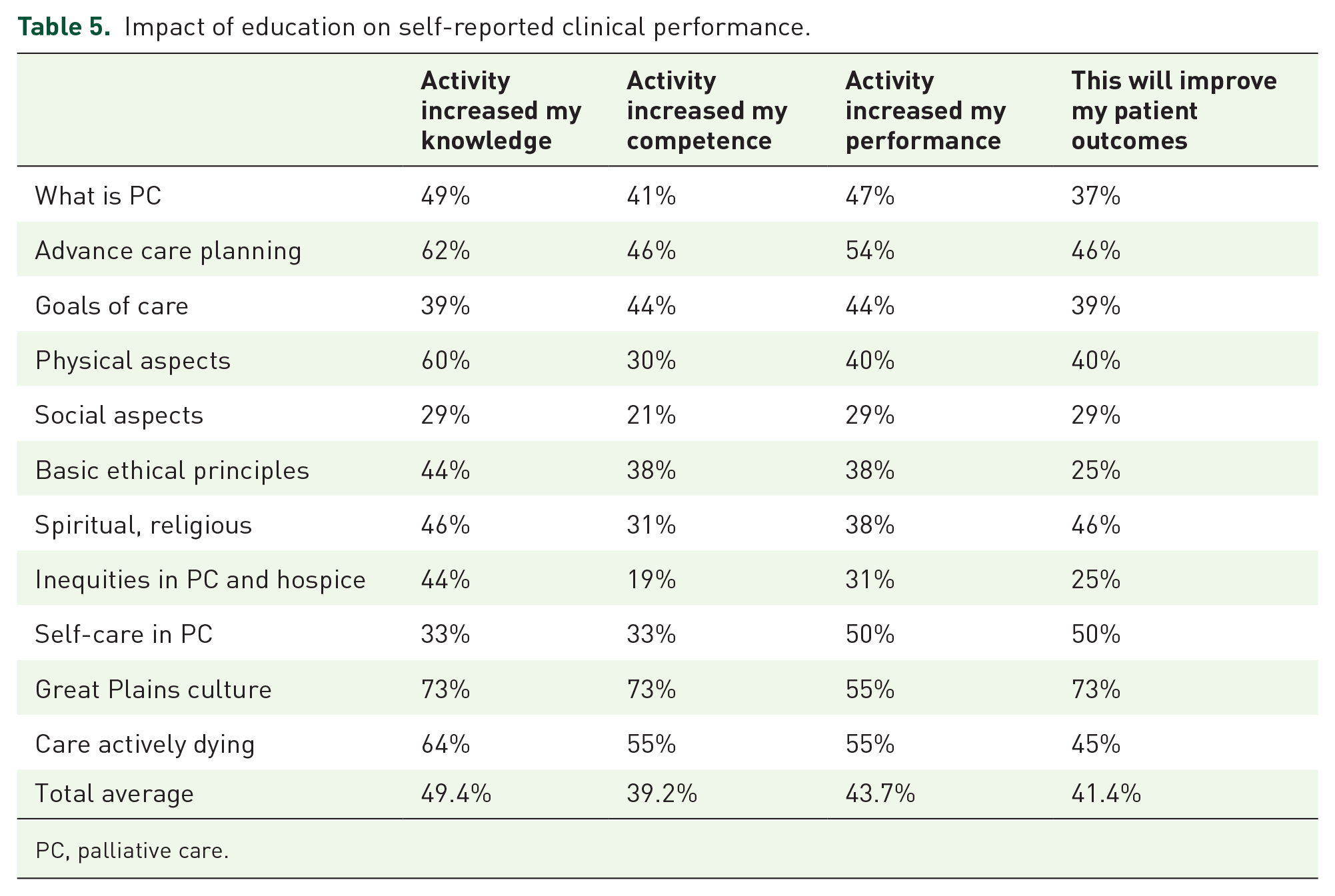
PC, palliative care.
Participants who indicated they agree or strongly agreed to the questions ‘How well did this educational offering meet my professional development goals?’, ‘Is the content of this activity likely to influence your practice habits?’, and ‘Were your personal objectives met?’ are shown in Table 6. Overall, participants indicated the education met their professional development goals (76.9%), will influence their practice habits (91.8%), and felt their personal objectives were met (99.4%).
Impact of education on professional and personal goals.

PC, palliative care.
After completing each CE module, participants were asked which areas of practice they were planning to change because of completing the module. Participants were able to select multiple practice areas to change (see Table 7). The changes in practice area with the highest selection were patient education, followed by clinical/patient interprofessional communication and teamwork.
Impact of education on commitment to change.

PC, palliative care.
Participants were able to choose more than one commitment to change areas.
In addition, participants could add free text comments after completing each CE module which further demonstrates how the modules will impact their practice. Many of these comments focused on asking patients or their families more specific questions related to PC (see Table 8).
Participant quotes on discussing PC with patients and families.

PC, palliative care.
As part of the evaluation, open-ended questions were available for participants to provide feedback for improvement of future CE modules (see Table 9). Many of the positive comments as well as the areas for improvement focused on the value of having engaging education and high-quality presenters. The participants’ self-identified commitments to change their practice were varied, but largely focused around increasing communication and awareness of PC with patients and within their interdisciplinary teams. Upon follow up at the selected 30-, 60-, or 90-day time frame, a few participants were already able to self-report they had successfully changed their practice. The majority who were successful in implementing changes were concentrated around increasing PC communication or discussion and including PC content into nursing programs (see Table 9).
Participant overall feedback.

Overall, 90% of the healthcare professionals can explain how teamwork contributes to continuous and reliable patient care and 41.4% felt they would be able to improve patient outcomes due to this education. In addition, nearly all participants felt this education would influence their practice habits and it met their personal objectives of participating in the education. Further data collection and analysis will occur; however, these findings are very promising.
Discussion
Alignment of the primary PC education series to the NCP Guidelines 12 promotes access to quality PC by bringing PC knowledge to additional healthcare professionals who will be able to incorporate it into their practice teams. In addition, it fosters consistent standards and encourages continuity of PC across care settings.
The CE planning committee recruited local healthcare experts across different healthcare systems, settings, and disciplines as speakers which promotes shared responsibility across all disciplines for delivery of quality PC. The intention of offering CE credits for several disciplines was effective as participants represented more than six disciplines. Coupling this with the positive impact on teamwork skills by nearly all participants, the primary PC education series promotes interdisciplinary care which is key to quality PC delivery.
The goal of educating rural, primary care healthcare professionals was partially met as two-thirds of the rural counties and six frontier counties had healthcare professionals participate. This education series has the potential to address the known PC access gap in rural areas of the state 8 by educating healthcare professionals in those areas in primary PC. This is a foundational step on which to build upon to fulfill the SDPCN’s mission to improve access to PC across the state.
An unanticipated finding was that the number of years of healthcare experience was not associated with the number of years of palliative and end-of-life care experience. Their perspective on having less experience in palliative and end-of-life care may be their motivation to participate in the CE series. Due to this reported lack of PC experience, it can be deduced that they are likely practicing outside of a PC setting which was the intended audience for this series. Furthermore, the participants reported the education will likely influence their practice and ability to improve patient outcomes. This is a step toward universal access to PC.
Overall, just under half of the participants self-reported that the CE modules increased their knowledge, competence, and performance. The participants’ experience in PC may have contributed to these evaluation results as 56% of participants had 3 years or more of PC experience (see Table 2). They may have been exposed to this introductory information during their healthcare experience; hence, not reporting the CE modules increased their knowledge, competence, and performance along with meeting their professional development goals.
While the majority of participants did not report an increase in their knowledge, competence, and performance, the vast majority (91.8%) reported the education would influence their practice habits. The target audience for this education was broad with the majority having more than 10 years of healthcare experience, which may explain this contradiction. Another explanation is they had an increase in their comfort in applying existing knowledge or being able to apply existing knowledge in a palliative care context after completing the modules. Other possible explanations are the participants’ interpretation of the questions and motivation for completing the modules which may influence the evaluation responses.
Lessons learned
The CE planning committee’s decision to provide online on-demand education versus live education sessions was challenging as it was a shift from the original planned education delivery format. The committee planning members were unsure as to whether this education delivery method would be well-received by healthcare professionals. Ultimately, the flexibility and cost-effectiveness associated with the online on-demand education sessions may have increased access and allowed healthcare professionals who otherwise may not have been able to attend live sessions to obtain the PC education.
Early engagement with the CE planning committee ensured feasibility of the design and roll out of the education related to the technology available for the project. Thinking about the end objective and how the learners would experience the education from start to finish was key. The first technology-related challenge was collecting participant demographic information once, instead of each time a module was completed. Due to the available technology software, one registration page for the entire series was implemented. After completing the registration page, the participant received an email with an all-access code for the series. As a result of this approach, several questions regarding the access code were received from participants. A second technology-related barrier experienced was the follow-up survey as it did not allow customization which prevented the preference to ask targeted long-term follow-up questions in addition to changes made in their practice. Evaluating the availability and limitations of technology or potential vendor partnerships early was another key in determining educational program functional abilities and required technological support.
Extensive discussion surrounding potential resources on which to base the PC education series occurred throughout the early planning stages. Study results support the decision to base the series on the latest edition of the NCP Guidelines 12 as it was effective in meeting the goals of the education and providing a comprehensive evidence-based PC CE series for healthcare professionals.
Future directions
During the evaluation at the end of each CE module, participants were required to identify an area of their practice they intended to change related to participating in the education. A long-term evaluation was conducted to determine whether they were successful in implementing their change in practice. The first CE modules have been active for over 1 year with 32 participants responding to the long-term evaluation survey. This results in limited long-term evaluation data. This long-term evaluation will continue to be collected and analyzed. One barrier identified with this method was no mechanism to require participants to complete a long-term evaluation as CE credit had already been awarded. To improve the effectiveness of long-term evaluation surveys, future education should include an incentive as well as a brief discussion of the value of the long-term survey to improve data collection and assessing the long-term impact of the education. In addition, discussion with hospitals on the ability to measure increase in PC referrals or plans of care being completed would be valuable to demonstrate adoption into practice and impact on patient outcomes.
To improve the analysis of the effectiveness of the CE modules, future education evaluations should include surveys that are able to separate evaluations by professions, years of healthcare experience, and palliative and end-of-life care experience. Another area for improvement based on the wide range of PC experience of participants would be to create an assessment for learners to identify which areas of PC they have gaps in to create a custom learning plan. This would decrease education time per person and increase impact on areas with the greatest room for improvement.
The module, What is Palliative Care?, has been available the longest and was also the module included in the initial marketing push. Due to the lower participation in other courses as well as the significant participation of only employees who work for the health system that manages the online LMS, current and future marketing strategies should target other health systems, including independent healthcare facilities. These health systems or facilities should create plans to use and market this education to help with adoption and engagement with the content, such as including it as required education for staff. Additional marketing strategies will include focusing on rural and frontier counties of the state, especially those with no participant representation.
Conclusion
The primary PC education series is easy to access, free, and follows the NCP Guidelines 12 which improved self-reported teamwork skills, likelihood of influencing practice habits, and professional and personal goals of healthcare professionals from a variety of disciplines and settings. Hence, the CE series addresses the professional practice gaps identified by the CE planning committee. These enhanced primary PC skills will improve the incorporation of PC into a variety of practice settings by multiple disciplines, which enhances access to PC outside of, and potentially referrals to, specialty PC programs.
Footnotes
Appendix 1
Acknowledgements
The authors wish to acknowledge the individuals and organizations who are members of the South Dakota Palliative Care Network and have devoted time, input, and efforts to create the CE modules and promote access to CE education in the state and region. We also wish to acknowledge Dr Margie Washnok who was instrumental in the development of the CE education and the Population Health Evaluation Center at South Dakota State University who provided support for the study. Finally, we acknowledge the key additional individuals from the online learning platform, the grant partners, and content experts who produced the CE modules.