
Abstract
Palliative care has become an increasingly important public health issue due to the rising acceptance of implementing a health promoting palliative care approach. To explore communication pathways that would facilitate implementation of this approach, we conducted a scoping review examining communication and enactment of care plans for older adults with life-limiting illnesses across health, social and community sectors. We used a scoping review methodology to map the current literature on communication plans between primary care and other sectors (community, health, and social). Five databases were searched MEDLINE (ovid), CINAHL (EBSCO), EMBASE (Elsevier), PsychInfo (EBSCO), and Scopus. The database search identified 5,289 records, after screening and hand-searching a total of 28 articles were extracted. Three major themes were determined through the records: (1) the importance of professional relationships across sectors, (2) the importance of community navigators in sharing the care plan, and (3) and creating comprehensive and multidisciplinary care plans. Findings suggested that enacting quality care plans is important to healthcare providers; the use of an electronic health records system can be useful in ensuring that all healthcare and community systems are in place to aid patients for better community-based care. Community navigators were also key to ensure that plans are communicated properly and efficiently. Further research is needed to determine how having a clear and properly implemented communication system for a healthcare system could facilitate community sector involvement in implementing care plans.
Keywords
Introduction
The Canadian population is aging. In 2014, 15.6% of Canada’s population was aged 65 or older. 1 By 2030, there will be 9.5 million seniors living in Canada, comprising 23% of its population. 1 In addition to age, chronic disease rates in Canada are also increasing. It is estimated that one in five Canadians over the age of 20 have a chronic disease, while four out of five are at risk of diagnosis of a chronic disease. 2 Every year, over 150,000 Canadians die from such diseases, and, unfortunately, this fraction of Canada’s population is only expected to grow larger as it ages.2,3 These trends, in both aging and chronic disease rates, have been paralleled across the globe, presenting healthcare systems with new challenges in providing impactful patient care. 4 In addressing these challenges, interdisciplinary medical teams worldwide are initiating, exploring, and providing palliative approaches to care.5–7
The palliative approach to care aims to improve quality of life and reduce suffering for people living with life-limiting conditions. 8 Typical provisions of the palliative approach include pain and symptom management, psychological, social, emotional, spiritual, and practical support, as well as added support for caregivers during the illness and after the death of the person in their care. 8 A critical aspect of the palliative approach is its emphasis on patient- and family-centeredness, necessitating respect for and solicitation of the voices, opinions, and feelings of those with life-limiting illness and their families. 8
It is important to note that a palliative approach to care should begin at the time of diagnosis and promote early interventions for patients and family members that match their needs and wishes, address comfort measures, and align with goals of care. 9 Advance care planning (ACP) is an element central to the palliative approach. It is an ongoing process of discussing preferences and making care plans between healthcare providers and patients, in anticipation of future mental and physical decline. 10 The implementation of ACP has been suggested to be an effective method for patients to mitigate existential distress while conveying their wishes and improving the patient–provider communicative experience.11,12 Newton et al. 12 found that a higher percentage of patients achieved their preferred priorities of care if ACP documentation was initiated by a district nurse in comparison to when it was initiated by palliative care hospital staff, specialist care, hospice, or nursing home care teams.
Although evidence suggests that implementing the palliative approach in primary care is advantageous, various barriers to implementation exist. 13 Formal training on the palliative approach to care is not consistently incorporated into medical school curricula, thus physicians may not have ready access to evidence-based guidelines and resources and need to hunt for the necessary knowledge and practice skills. 14 Primary care providers (PCPs) provide first-contact services for patients, and can include team members in addition to general practitioners, such as physician assistants, nurses, nurse practitioners, and district nurses.15,16 PCPs are positioned well within healthcare systems to develop ongoing trusting relationships with patients while coordinating and providing personal end-of-life care. 10 However, the health system may not always support them taking time in their practice routines to develop trusting relationships with patients. 17 A barrier to care coordination may be less than optimal intra-team communications. 18
In addition to intra-team communication, advance care plans, and palliative approaches to care in general, often necessitate intersectoral communications between primary care and other health and social agencies. These communications can facilitate care that is consistent with patient preferences, and preferences of health professionals, specialists, nurses, psychologists, counselors, social workers, community workers, and volunteers, because they can assist patients with identifying and accessing critical community-based resources. Increasing the occurrence, efficiency, and effectiveness of such communications is imperative. Despite the understanding that communication between sectors is important, little is known about how sectors communicate with each other. For example, studies have looked into communication with or among different medical areas (i.e. oncology and primary care), however, little is known about how primary care communicates with community sectors.
To better understand these communication channels, this scoping review was guided by the following research question: how do PCPs communicate and enact care plans for older adults with life-limiting illnesses across health, social, and community sectors? Specifically, we wanted to identify the various care plans, forms of communication, and communication pathways shared between PCPs and other health, social, and community sectors.
Methods
A scoping review aims to map the existing literature in a particular field or topic to understand what types of knowledge or evidence exist. It is intended to incorporate a broad array of sources to understand the depth of existing evidence from the research and gray literature. 19 This type of review is of particular use for research questions that have not yet been extensively reviewed, are complex, or heterogeneous in nature. 20 A scoping review provides a rigorous and transparent methodology for mapping the extent of the evidence available. Our interest in exploring communication across health, social, and community sectors fits well within the purview of a scoping review.
Database search of the existing literature
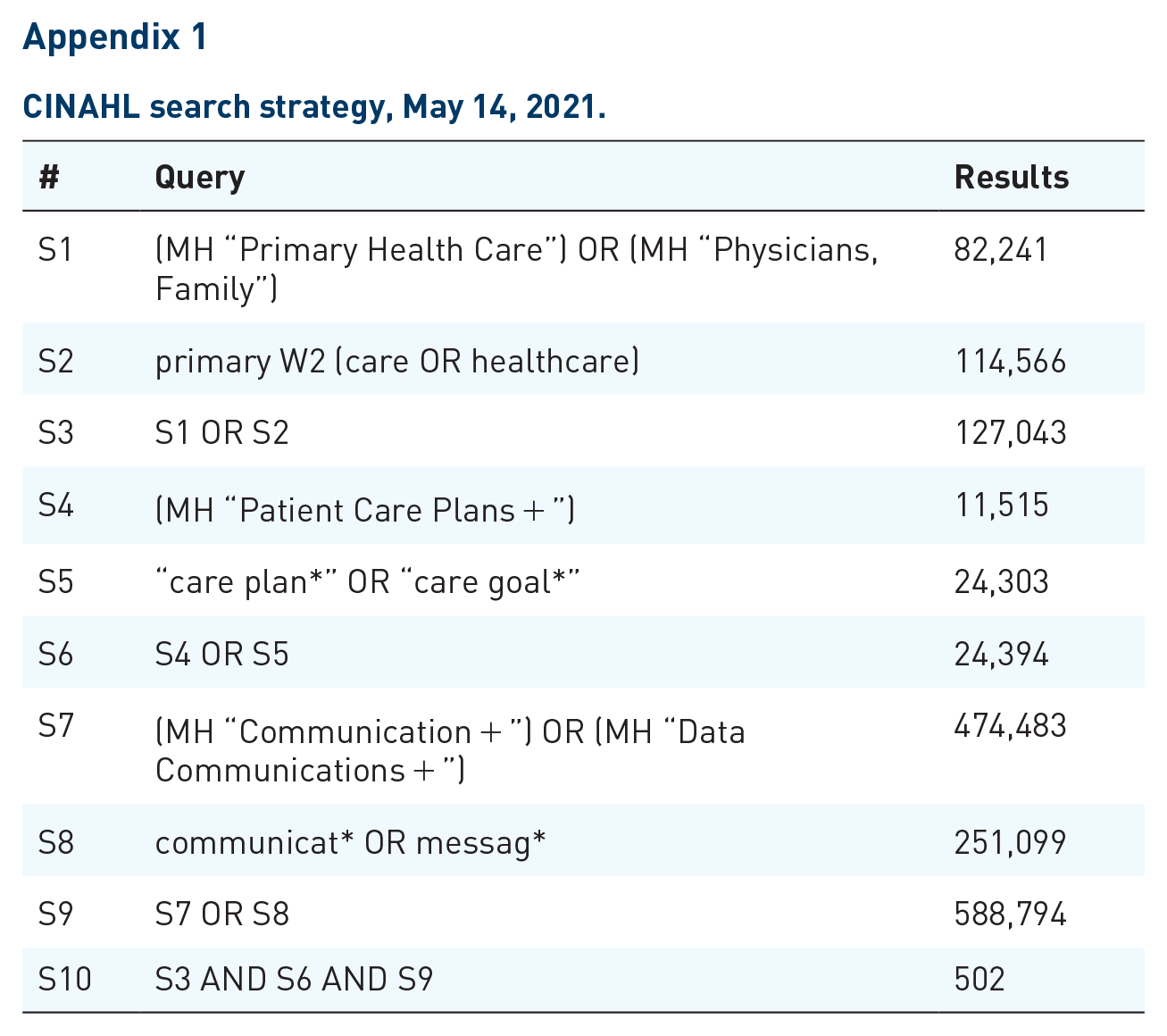
To conduct the scoping review, a comprehensive search of the existing literature was carried out in collaboration with an academic librarian. The database search was conducted in MEDLINE (ovid), CINAHL (EBSCO), EMBASE (Elsevier), PsychInfo (EBSCO), and Scopus in June 2021. Articles were retrieved from database inception—June 2021. Sample search terms used for the CINAHL search are in Appendix 1.
To be included, studies had to:
a. Be written in English,
b. Focus on how PCPs create, communicate, and enact plans,
c. Be about communicating or creating care plans for older adults with chronic illness,
d. Describe communications between health, social, and community sectors,
e. Be specific to older adults or mention age range 50 or older,
f. Be either theoretical (e.g. best practices for creating and communicating care plans), empirical (e.g. protocol, evaluation), text and opinion papers, or reviews.
Studies were excluded if they
a. Discussed communication within primary care (i.e. primary care physician with primary care nurse) or from hospital to primary care (i.e. discharge planning).
b. When study protocols or studies detailed training for health professionals.
Once the search was completed records were downloaded into Covidence (a review management software system) and duplicates were removed. Covidence was then used to organize the screening and extraction for the review. Reviewers scanned the same 50 articles to validate the inclusion process then met to review their results. There were two stages to the review process. The title and abstract phase focused on identifying articles that reflected key study concepts and the full-text stage explored whether key concepts are operationalized in a way that could address the research question.
A team of five research members independently scanned the title and abstract of every record retrieved, with at least two reviewers per article (JL, NJ, TH, EK, and GW) Potentially relevant papers were retrieved in full and their citation details imported into the Covidence software. Next, two of three independent reviewers (JL, NJ, and TH) assessed the full text of included articles in detail against the inclusion criteria. In addition, reference lists in the included articles were reviewed to identify additional relevant literature. Data were extracted by two independent reviewers (JL and NK). Data were extracted using the Covidence software and pre-coded data extraction categories, see Appendix 2 for detailed template. When conflicts arose during the screening and extraction processes a senior team member with substantial background in the review topic (GW) resolved them. The group then would have a discussion on areas of conflict to ensure all team members had the same understanding of what articles to include and what data should be extracted.
A 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart was created as a visual summary of the number identified through database search and other sources, as well as the number of records included and excluded. 21
Data analysis
Evidence from the search strategy on intersectoral communication between primary care and social or community services regarding older adults was synthesized. Data analysis was completed in five phases: data reduction, data display, data comparison, conclusion drawing, and verification. 22 All data were combined to provide one complete data set for analysis and cleaned by one author (JL). Data were condensed and coded thematically by a single author (JL) and checked for consistency by a second author (NJ). The extracted data were presented in a tabular format that aligns with the study’s objectives. Results were classified under the main conceptual categories (including country of origin, study population, study design, and setting); aim; outcome measures; communication pathway; type of communication; communication tools; and key findings and implications.
Data evaluation
Given the focus of this scoping review on mapping existing literature, the Tomlin & Borgetto’s 23 classification of research pyramid was used to assess the level of evidence. This pyramid breaks down articles into four separate categories (descriptive, experimental, outcomes, and qualitative research) to evaluate the level of evidence of studies included from different study designs. Each category describes four levels of evidence from most to least rigorous. Descriptive research is divided into Level 1: Systematic reviews of related descriptive studies; Level 2: Association, correlational studies; Level 3: Multiple case studies (series), normative studies, descriptive surveys; and Level 4: Individual case studies. Experimental research is divided into Level 1: meta-analyses of related experimental studies; Level 2: individual (blinded) randomized controlled trials; Level 3: controlled clinical trials; and Level 4: single-subject studies. Outcome research is divided into Level 1: meta-analyses of related outcomes studies; Level 2: pre-existing groups’ comparisons with covariate analysis; Level 3: case–control studies; pre-existing groups’ comparisons; and Level 4: one-group pre–post studies. Finally, qualitative research is divided into Level 1: meta-synthesis of related qualitative studies; Level 2: group qualitative studies with more rigor (a, b, and c); Level 3: group qualitative studies with less rigor—(a) prolonged engagement with participants, (b) triangulation of data (multiple sources), and (c) confirmation of data analysis and interpretation (peer and member checking); and Level 4: qualitative studies with a single informant. As part of the review, we included non-studies, such as commentaries and opinion papers identified in our search strategy. Given there is no consensus on how to evaluate these articles, we used Enago’s Academy article 24 to help categorize and assess these articles.
Results
The database search of existing research literature identified 27 sources that discussed intersectoral communication within a primary care setting and another health, social, or community sector. There was an additional article found through hand-searching references of included articles, resulting in 28 articles reviewed. These articles discussed goals of care and were targeted toward a more senior population. Search results are in the PRISMA diagram of Figure 1.
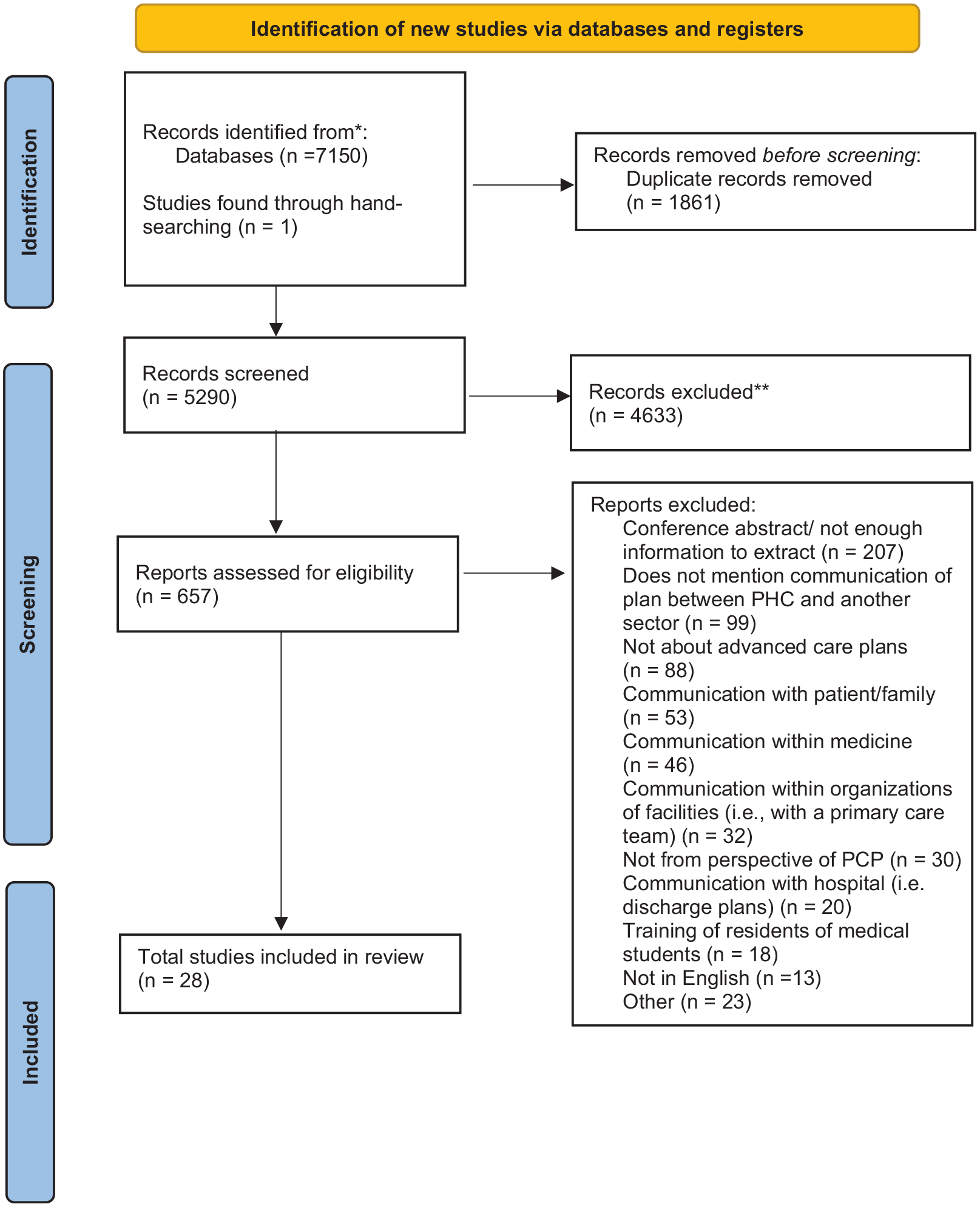
Review process.
Records identified
The sources involved any form of communication between primary care and another health, social, or community sector about goals of care and referral of older adults to community resources. All 28 articles were published from 1998 to 2021, with a wide variety of geographical locations, including United States (9), Australia (6), United Kingdom (7), Canada (2), Denmark (2), the Netherlands (1), and Norway (1). Thirteen articles specifically discussed the use of electronic health records (EHRs) and how those could facilitate, or in one case hinder, communication across sectors. The study methods varied with the most common being qualitative research (8), text & opinion papers (6), mixed methods (4), quantitative (4), case report (1), and other (4). The communication pathways ranged from primary care communicating directly with community (12), primary care with disease management teams (1), all communication across different sectors (6), primary care with pharmacy (2), primary to patient portal (2), and community providers with other providers (4).
A summary of the extracted data from the included articles identified is provided below, more information is provided in Table 1 with more details regarding care plans and communication in Table 2.
Characteristics of studies that reviewed how care plans were communicated from primary care to another sector.

ACP, advance care planning; CIM, complex intervention for multi-morbidity; CMLTC, case management for long-term conditions; DMP, disease management program; EPC, Enhanced Primary Care; GP, general practitioner; GSF, Gold Standard Framework; HBPC, home-based primary care; MDPOA, Medical Durable Power of Attorney.
Communication plans and tools of studies that reviewed how care plans were communicated from primary care to another sector.

ACP, advance care planning; CMLTC, case management for long-term conditions; GP, general practitioner; HBPC, home-based primary care; MDPOA, Medical Durable Power of Attorney; NP, nurse practitioner; VIP, virtual integrated practice.
Summary of included articles
Thematic analysis
Information from this review was sorted into three themes: (1) the importance of relationships across sectors, (2) the importance of community navigators in sharing the care plan and goals of care, and (3) and creating comprehensive and multidisciplinary care plans. The breakdown of all studies and which ones correspond with certain themes is detailed in Table 3.
All included studies and their corresponding themes.

The importance of relationships across sectors Sources reviewed featured a variety of intersectoral communication relationships and pathways. Twelve sources examined communication from health to community sectors25,31–33,36,37,39,41,43,49,51,52 and four investigated the opposite direction of communication; community programs communicating to the health sector.26,27,46,48 Five sources included communication between health and social sectors,26,28,30,38,47 and another four explored interactions between health sectors (primary, secondary, tertiary),38,40,47,50 other pathways included primary care to pharmacy45,47 and informal care providers. 53 Communicating between key individuals was considered to be a strong facilitator.
Several sources24,25,30,31,39,41,44 emphasized the importance of having strong, foundational relationships between all healthcare practitioners involved in an individual’s care, and suggested that multiple sectors need to be involved in the planning and design of the communication pathway. This collaboration was fostered when there were supportive and trusting relationships31,48 or when individuals had defined roles or ‘to-do’ lists.37,46,51 To ensure all providers felt part of a team, Rowlands et al. 48 highlighted the importance of making carers aware that there were available supports when navigating patient care. When referring to community services it was important for general practitioners (GPs) and other HCPs to understand what was provided. Aids to understanding community services, as well as promoting effective communication between sectors, described by sources included using standardized letters, 52 mentoring programs, 45 specific flow charts, 46 constant telephone communication, 30 centralizing communication, 27 and using shared documents for assessments. 26 In addition, sources emphasized the transparency of roles. 37 Anderson et al. 29 found that EHRs were a barrier to communicating plans as they lacked the proper system- wide rollout to be useful and lead to some miscommunication between providers and finding patient history from other providers.
Overall, interpersonal relationships were key to aiding providers in navigating the healthcare system. There is a need to foster communication using practices that help develop interpersonal relationships to better support intersectoral communication. Providers need to look at each other as collaborators to nurture a system that is truly multidisciplinary and becomes the standard of care and best practice.
The importance of community navigators in sharing the care plan and goals of care To facilitate communication between health sectors, the importance of an individual that acted as a liaison between sectors, often acting as a broker between various practices, was noted by several sources.33,43,49–51,53,54 This figure took on numerous titles; namely, community matron, 33 nurse navigator, 54 a broker, 50 nurse facilitator, 43 or liaison nurse. 49 In considering the aforementioned articles depicted the importance of this role and its usefulness from both the perspective of patients and the care team. These healthcare providers aided in communication as they took the burden off the primary provider to find sources, as well facilitating an in-depth discussion with patients about areas they wanted to prioritize. Given community navigators’ extensive experience identifying and reaching out to other community resources they were well equipped to translate between what the PCP wanted and what was available in the community.
In creating and sharing the care plan, community navigators acted as an accessible source to patients, and were tasked with knowing community programs that may be needed to facilitate best care for older patients. It is important for all parties involved (providers, community navigator, family/ friend caregivers, and patient) to work together to better patient care.
Creating comprehensive and multidisciplinary care plans Care plans described by the included sources all focused on addressing patients’ goals of care, specifically goals of care nearing end of life. Eight studies incorporated ACP,28,31,32,34,35,43,44,48 with one using an EHR ACP interface to allow for standardized planning. 44 Sources also focused on providing home-based care, featuring home assessments and interdisciplinary care home visits.30,41,46,49,52 In addition, chronic care management was featured in four studies.31,32,42,45 Important to most care plans was the inclusion of multiple sectors into a single care plan, this entailed a plan that thought of the patient from multiple viewpoints and points of care. This often-involved collaboration between primary and community sectors, aiming to provide patient-centered care. Other plans included support for surrogate decision-makers, 35 patient-centered goal setting,25,31,47 and virtual integrated practices. 47 Proactively implementing care plans was crucial, and it was suggested that this planning be completed early in the disease trajectory.32,46 Emphasis was placed on the importance of effectively and accurately identifying patients that needed, or were expected to need, comprehensive care. 29 Comprehensive care entailed using a multi-level lens and enrapturing multiple healthcare viewpoints, being part of a multi-dimensional practice could add in this practice 29 as well as triaging and calling on community resources if needed. 36
When the care plan was comprehensive and multidisciplinary, patients viewed their entirety of care from a team-based and holistic perspective. As well, the burden of creating a plan was lessened when multiple sources contributed to what needed to be included in the plan. 49 These comprehensive plans often encompassed patients’ desires and goals of care.
Discussion
The aim of this review was to examine the communication between primary care and other health, social, or community sectors caring for older adults. Specifically, we wanted to identify the various care plans, forms of communication, and communication pathways shared between PCPs and other health, social, and community sectors. To do this, we synthesized literature from a wide variety of empirical, clinical, and theoretical sources to help gage our understanding of intersectoral communication. The themes identified from this review were relationships, community navigators, and comprehensive care plans.
Numerous intersectoral communication pathways were identified, illustrating the importance of maintaining open, trusting, and communicative relationships among interdisciplinary team members in caring for older adults. A significant communication pathway explored was between health and community sectors. Community-based palliative care is a growing field, and has been suggested by researchers to be the natural evolution of palliative care. 55 As such, research examining this communication pathway is helpful to the development of comprehensive palliative care in the future. Various tools were identified that assisted in fostering these intersectoral relationships, including mentoring programs, flow charts, and shared assessment documents, as well as constant telephone and centralized communication. EHR in theory would allow for a greater uptake of communication and a greater use of collaborative care, however in practice there has been struggles with integration, 56 alert fatigue, 57 and potentially time-consuming training. 58 Identified barriers to using EHRs is that they have high initial costs, require a change in work habits, may result reduce productivity in the initial stages and require technical knowledge. 59 Other research has suggested that differences in communication training between healthcare professions can be a barrier to effective relationship-building, citing how the highly descriptive form of communication taught to nurses often clashes with the succinct style taught to physicians. 60 Similar discrepancies may exist between different healthcare sectors as well, to which training programs, standardized tools, and simulations may serve as solutions. 60
In addition, having an individual act as a community navigator or care coordinator was another theme that emerged, suggesting that systematically integrating this role into healthcare may be critical in achieving successful intersectoral communication and interdisciplinary care. For example, integration was found to be beneficial in facilitating connections and communications between various sectors and patients. The care coordinator role has also been suggested to have positive impacts on pediatric, 61 orthopedic, 62 and chronic disease 63 care in addition to the palliative approaches described in this review. This role is often accomplished by a nurse. One barrier to this may be the availability or cost of nurses fulfilling this role. A possible solution is training other individuals to complete this role. Volunteers running community-based program have been found to be cost-effective and effective for helping community patients navigate the healthcare system. 64 In a study examining the feasibility and impact of a volunteer-led healthcare coordination project, volunteers assumed the role of navigators in early palliative care, they found this role to be rewarding and meaningful. 65 Furthermore, clients were highly satisfied with the volunteer program, noting that volunteers assisted them with coordinating access to services and awareness of available community resources. 65 A similar study found that volunteer initiatives decreased nurse involvement, but did not replace their participation altogether. It was noted that mentorship provided by nurse navigators was critical to volunteers in understanding their role, and support from these nurses was helpful as volunteers learned their scope and boundaries. 64
The third theme identified consisted of comprehensive care plans. Literature reviewed examined various forms of care plans, including ACP, home-based care, and chronic care management. This wide range of care plans shows the need for early, comprehensive care plan integration of a palliative approach to care that will keep individuals in their community by increasing the supportive care in their community. 66 As well, this confirms prior literature that care plans need to be communicated to all sectors to ensure patients and family’s needs are met at the end of life. 17 The inclusion of intersectoral input in these care plans was emphasized by multiple sources in our review.
The use of EHRs that are continually updated and able to be accessed by multiple healthcare providers may help enact a more comprehensive plan for patients. In our review there was an even split between using and not using EHRs to aid in communicating the plan among the care team. Given the positive effects of having an electronic portal system 35 that could enable uptake from practitioners and patients, this may be a viable option for healthcare systems. However, given the time-consuming education at the upfront of the use of EHRs 28 it may need to be implemented over time and gradually into the health system and with proper training and pilot testing of their use.
Limitations and future directions
The review was limited by our search strategy. Given the breadth of work and terminology in this area and the different nuances of care across health, social and community sectors we may have missed some sources. However, our search strategy was broadened by incorporating the services of an academic librarian, who conducted intensive preliminary searches to refine our final search terms. Our inclusion criteria were limited to studies published in English; therefore, our review may have missed studies in other languages that could have contributed different perspectives to our findings.
In our search, we included commentaries and opinion pieces. Although we did not do a gray literature search, we did conduct a preliminary search of Canadian websites (i.e. private, national, provincial, health authority) to identify existing communications to the public regarding ACP. This search resulted in 56 documents. Most were informational and/or provided guidance to the public on beginning ACP that were linked to region-specific resources for carrying out ACP. These documents did not focus on communications across sectors. It would be beneficial for future reviews to consider a comprehensive gray literature search to identify existing programs that target communication among sectors and community resources not represented in published sources. This search may necessitate contacting community agencies for more in-depth details. Unfortunately, often community programs do not have adequate resources to do program evaluations or to disseminate findings.
Conclusion
The current scoping review offers a detailed analysis of communication plans across primary care and other sectors. We identified three major themes regarding how to enact and communicate care plans to enhance goals of care in patients. Subsequent evaluation research is needed to understand whether these tools work in practice or can be used on a larger scale. This review illustrates the need to disseminate care plans to all sectors and how additional supports (i.e. community navigators, comprehensive plans, and EHRs) can aid PCPs when working with their patients to achieve their goals of care. It is important that all sectors are aware of the patients’ goals of care and have a strong communication networks. The further development and testing of models that aid healthcare professionals with communicating care plans is needed to ground care plans, so that, they are best practices for patients.
Footnotes
Appendix 1
CINAHL search strategy, May 14, 2021.
| # | Query | Results |
|---|---|---|
| S1 | (MH “Primary Health Care”) OR (MH “Physicians, Family”) | 82,241 |
| S2 | primary W2 (care OR healthcare) | 114,566 |
| S3 | S1 OR S2 | 127,043 |
| S4 | (MH “Patient Care Plans + ”) | 11,515 |
| S5 | “care plan*” OR “care goal*” | 24,303 |
| S6 | S4 OR S5 | 24,394 |
| S7 | (MH “Communication + ”) OR (MH “Data Communications + ”) | 474,483 |
| S8 | communicat* OR messag* | 251,099 |
| S9 | S7 OR S8 | 588,794 |
| S10 | S3 AND S6 AND S9 | 502 |
Appendix 2
Data extraction template.

| Title of paper |
| Lead author last name |
| Publication date |
| Country in which study conducted |
| Aim of study |
| Study design |
| Dates of intervention/study |
| Population description |
| Inclusion criteria |
| Exclusion criteria |
| Definition of care plan |
| Type of communication |
| X sector communicating to Y sector |
| Electronic health records? |
| Tools to help with communicating plan |
| Main outcomes |
| Key findings |
| Implications |
| Limitations |
Author contribution(s)
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (grant no. 148655) and the Canadian Cancer Research Institute (grant no. 704887).