
Abstract
Background:
New public health approaches in palliative care attribute an active role to civic society in providing care for those who are seriously ill, caring, or bereaved. Accordingly, Civic Engagement In Neighbourhoods regarding serious illness, dying and loss (CEIN) are emerging worldwide. However, study protocols that advise on how to evaluate the impact and complex social change processes underlying these civic engagement initiatives are lacking.
Objectives:
The main objective of this study is to describe the study protocol for the evaluation of civic engagement initiatives in serious illness, dying, and loss in two neighbourhoods in Flanders, Belgium.
Design:
A convergent-parallel mixed-method process and outcome evaluation for the CEIN study.
Methods & analysis:
We look at the evaluation of CEIN through a critical realist lens, thereby including the social, political, and economic determinants of social change in CEIN, the mechanisms to achieve this social change, the outcomes, and the mutual connection between these three aspects. We will conduct a convergent-parallel mixed-method process and outcome evaluation in which qualitative (i.e. observations, interviews, group discussions, and ego network mapping) and quantitative data (i.e. a pre–post survey) are simultaneously but separately collected and analysed and in the last stage combined by narrative synthesis.
Discussion:
This protocol illustrates the difficulty of operationalising the desired long-term impact of social changes regarding serious illness, dying, and loss into more manageable outcomes. We recommend a well-cogitated logic model that connects the outcomes of the study to its potential actions. Applying this protocol in practice is a constant exercise between providing sufficient flexibility to meet feasibility, desirability, and context-specific needs in the CEIN study and providing sufficient guidelines to structure and control the evaluation process.
Keywords
Background
Following a new public health approach in palliative care, citizens have attributed to caring for their fellow human beings in times of serious illness, dying, and loss. 1 Communities that embody such societal actions are typically called compassionate communities and are defined as ‘a community of people who are passionate and committed to improving the experiences and well-being of individuals who are dealing with a serious health challenge, and those who are caregiving, dying, or grieving’ (p.1). 2 Compassionate communities, especially on the level of the neighbourhood, are initiated from an asset-based community development approach that draws on the existing neighbourhood networks and initiatives. This Civic Engagement In Neighbourhoods regarding serious illness, dying and loss (CEIN) study uses the existing societal capital (e.g. volunteer organisations, neighbourhood committees, clubs, organisations, and (digital) platforms in the neighbourhoods) to achieve social change and is initiated in the context of compassionate cities in which local governments; cultural and care organisations; and schools, workplaces, and places of worship work together in developing capacity regarding serious illness, dying, and loss.3,4 The societal actions in CEIN are interpreted as actions of civic engagement, which we define as all collective action undertaken to help improve connections between, or conditions for people in the community around serious illness, death, and loss, including all forms of collective formal or informal volunteering.5–7 Based on this definition, we conducted a systematic review of CEIN initiatives worldwide. 8
We found 19 CEIN initiatives, their activities ranging from social, emotional, and practical support, to navigation for ill people to community resources. 8 Many of these initiatives showed promising results such as an increased understanding and knowledge of death, loss of palliative care in the community, 9 and increased empowerment of volunteers to provide end-of-life care for older persons in their communities. 10 However, the quality of the evaluation and the strength of evidence varied greatly between the studies as they applied different evaluation aims, designs, data collection methods, and outcomes. 8 In addition, most of the evaluation studies were limited, as they focused either on a process or an outcome evaluation and mostly focused on one particular aspect of the initiative (e.g. training for volunteers). This review showed the potential for CEIN initiatives to achieve social change around illness, death, and loss, 11 but it also illustrated that compassionate communities are complex adaptive processes that are difficult to study with classical methods aimed at linearity and predictability. 8 With the number of compassionate communities emerging worldwide, so is the question of how to measure its process of development and its impact adequately.
In this article, we describe the study protocol for the evaluation of civic engagement initiatives in serious illness, dying, and loss in two neighbourhoods in Flanders (Belgium), following the SPIRIT 2013 reporting guidelines. 12 Since this CEIN study transcends a predictable health science model with predefined aims and outcomes, a research protocol is all the more important for avoiding different types of study design and conduct bias (e.g. describing what seems interesting without a predefined model).13,14 Consequently, this protocol presents a methodology for a convergent mixed-method process and outcome evaluation that aims to measure how the CEIN initiatives are developed by citizens and other key figures in the neighbourhood, and what the impact of these initiatives is. Furthermore, we reflect on how to apply this methodology in complex, adaptive processes of community development.
Methods
Setting
The study takes place in two neighbourhoods in two semi-urbanised areas in Flanders, Belgium. 15 The first neighbourhood is situated in Sint-Kruis with a total number of 16,225 inhabitants and the second neighbourhood is in Herzele with 18,477 inhabitants. Together with municipality representatives in Herzele and Sint-Kruis, we demarcated the neighbourhoods as the geographical area that is most centrally located and is most likely to entail neighbourhood participation around serious illness, death, and loss. In Sint-Kruis, this neighbourhood (4222 inhabitants) coincided with the two geographical areas Sint-Kruis Centrum and Sint-Kruis Kruispoort. In Herzele, the neighbourhood (3210 inhabitants) was chosen in a radius of 1.5 km around this local service centre.
Design
A critical realist paradigm
Since civic engagement initiatives regarding serious illness, dying, and loss go beyond clinical and medical approaches to increase societal capacity in these topics, there is an increasing awareness that their evaluation would surpass a mere health science approach with predefined outcomes and that their evaluation would acknowledge the complex mechanisms that underlie social change.16,17 A critical realist philosophy recognises that in complex change processes, there is both an objective context in which the change takes place and a subjective context that entails people’s interpretations, perceptions, language, and relationships. 18 Consequently, critical realism recognises that we should not only observe and measure visible change but also the ‘causal powers’ or the mechanisms that are at play. 18 By looking at the evaluation of CEIN through a critical realist lens, we recognise that the desired social changes around serious illness, death, and loss cannot be isolated from the political, social, and cultural context in which they occur. Consequently, by identifying the mechanisms of social change in CEIN, we look at the broader societal context, as well as the developed actions and initiatives, their desired impact, and the interrelation between these three aspects. Given the theory-driven character of critical realism, we started the CEIN study by conducting a systematic review of civic engagement initiatives around serious illness, death, and loss worldwide, to provide us with first assumptions on how social change might occur in CEIN. These assumptions were captured in a logic model which must be considered a dynamic instrument that will be adapted throughout the study.
A logic model
We developed a logic model visualising the mutual connection between the inputs of CEIN, the CEIN initiatives and actions that are developed and their potential outcomes and impact (Figure 1). Although we drew up this initial logic model, it is a dynamic instrument that will be adjusted in the course of the study.

Logic model for the CEIN study.
Input: The inputs for developing CEIN initiatives are threefold and entail initiating the study in the context of a Compassionate City, having a Compassionate Community facilitator who enables the process of development and having a neighbourhood worker that enhances connections between the different key figures.
- A Compassionate City context: Both neighbourhoods in which the CEIN initiatives are developed are situated in Compassionate Cities. As a result, CEIN is embedded in a supportive local policy that stimulates participation in actions of civic engagement in different city domains (e.g. schools, workplaces, public spaces, and neighbourhoods).
- A Compassionate Community facilitator: All CEIN initiatives and actions are developed in collaboration with a community facilitator that enables the process of co-creating CEIN with the different social partners and key figures (e.g. neighbourhood committees, mailmen, and volunteers) in the neighbourhood. The community facilitator will consider the different aspirations of these interested parties and will guard whether the CEIN actions that are being developed are in line with the desired social change regarding serious illness, dying, and loss.
- A neighbourhood worker: In both neighbourhoods, there is the need for someone who initiates and strengthens social networks and makes the connection between the different key figures. The neighbourhood worker is a very visible and approachable person for people.
- Stakeholders: The stakeholders in the neighbourhood are all the social partners and key figures (e.g. volunteers, people from neighbourhood committees, and local merchants) who are motivated to develop CEIN and to engage in the topics of serious illness, death, and loss.
Actions:
- Meetings with a Compassionate City core team of stakeholders: The CEIN study will be initiated with the formation of a Compassionate City core team of social partners who already work around serious illness, death, or loss in the larger city context. Together they address the main direction of the Compassionate City and they brainstorm about the assets from which the CEIN initiatives can be developed.
- Neighbourhood talks with different stakeholders: Given the asset-based community development approach of the CEIN study, the initiatives and actions will not be determined by the researcher in advance, but are decided upon by the social partners and key figures in the neighbourhood. Through conversations with the researcher and community facilitator, the social partners and key figures will be made aware of the study and will be enabled in forming networks around serious illness, dying, and loss in their neighbourhood.
- Civic engagement actions: The CEIN actions can take different forms ranging from neighbourhood networks providing social, practical, medical, or spiritual support, to peer-support groups, and offering navigation for people with care needs to the appropriate organisations or other community resources. The Compassionate Community facilitator is responsible for ensuring that all the developed actions are in line with the desired outcomes and impact of the CEIN study.
Outcomes: The desired impact of CEIN, broadly speaking, is a social change regarding serious illness, death, and loss in the two neighbourhoods. Based on neighbourhood talks with stakeholders and city representatives in the two chosen neighbourhoods, we translated this long-term impact to middle- and short-term outcomes (i.e. increased neighbourhood social cohesion, increased neighbourhood support regarding serious illness, dying, and loss, and increased connections between formal and informal stakeholders (i.e. social partners and key figures) in the neighbourhoods).
Participatory action research
Observational studies have a long tradition of being linked to community research, as it is considered an objective means to capture the complex political and social context of development, as well as the internal group dynamics. 19 However, in the CEIN study, the researcher is not an outsider to the development process, as is the case in purely observational studies, but is a contributor to the development by facilitating the neighbourhood networks and guarding the long-term impact of social change regarding serious illness, dying, and loss. Although CEIN is thereby a participatory action research, the general public remains the main stakeholder in creating initiatives for issues concerning serious illness, dying, and loss in their neighbourhood.
Convergent – parallel mixed-method process and outcome evaluation
Our CEIN study will be evaluated by conducting a convergent-parallel mixed-method process and outcome evaluation in which we will simultaneously collect qualitative (i.e. observation, interviews and focus groups, and document analysis) and quantitative data (i.e. pre-post survey, Most Significant Change Technique, and ego network mapping). 20 The qualitative and quantitative results will be analysed and reported separately and will then be synthesised into overarching interpretations and insights about the change process in CEIN (Figure 2).20,21 Data will be synthesised by using a joint display that allows to compare and merge the data based on identified descriptive themes (see also 3.3. Synthesising the data). 22 Our mixed-method research design provides the opportunity to look beyond typical quantitative methods for measuring impact (e.g. a pre–post survey) 23 and allows us to measure impact using qualitative data collection methods as well, e.g. the Most Significant Change technique. 24

Convergent-parallel mixed-methods approach of CEIN.
The process evaluation is structured following the 6F model, a framework for analysing social innovation actions and initiatives. 25 This framework includes Foundations (the context of CEIN and the Compassionate Community philosophy behind CEIN), Focus (the challenge CEIN is seeking to address and the desired impact of CEIN), Function (the CEIN actions that are being developed), Form (the development process of CEIN), Facilitators (the enablers or barriers that influenced the development of CEIN), and Followers (all interested parties involved in CEIN). The outcome evaluation is based on the outcomes that are formulated in the logic model. An overview of the research questions and data collection methods can be found in Figure 3.
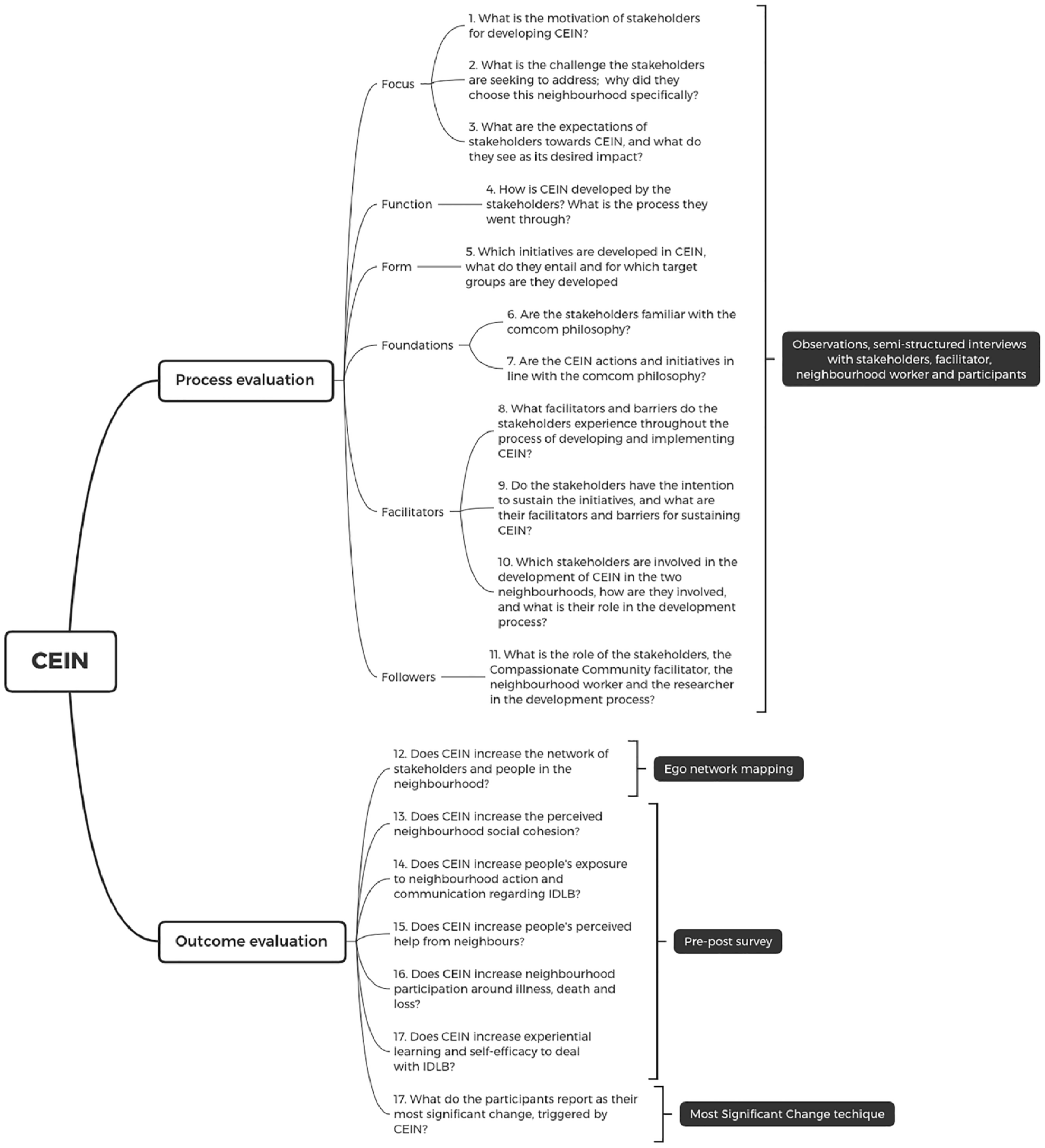
Overview of research questions and data collection methods.
Data collection
Since the CEIN study will be co-created with stakeholders (i.e. social partners and key figures), there is a need for flexibility in the choice of data collection methods and for adaptability in using these data collection methods depending on the direction in which CEIN is developing. This means that some of the data collection methods may not be used after all because they are no longer desirable or relevant, and others may be adapted to meet context-specific needs. Keeping this in mind, we describe several possible data collection methods for the process and outcome evaluation of the CEIN initiatives. The described quantitative and qualitative data collection methods will be applied simultaneously following the convergent-parallel mixed-methods approach. 19
Data collection methods for the process evaluation
Observations
Aim: Observations are conducted to gain insight into how CEIN initiatives are developed by the stakeholders (social partners and key figures), which initiatives are being developed, and which barriers and facilitators present themselves in this development process.
Data collection procedure: The researcher (LDEE) will conduct observations during meetings with the core team and during the entire process of developing and implementing CEIN in both neighbourhoods. The observations are conducted following a predefined template that provides flexibility in measuring topics that are not explicitly vocalised by the stakeholders. The observational data will be further explored via interviews or group discussions.
Timing: The observations are conducted in all relevant meetings and actions.
Semi-structured interviews and group discussions
Aim: Semi-structured interviews and group discussions will be conducted to gain insight into the motivations for initiating CEIN, the expectations towards it, the desired impact and the facilitators and barriers in the development process. The interviews and group discussions will be conducted with the stakeholders, the neighbourhood worker and the Compassionate Community facilitator.
Data collection procedure. A topic guide is prepared in advance based on the research questions in Figure 2.
Timing: The interviews with the Community Facilitator and the neighbourhood worker are conducted every 3 months. The frequency of the interviews or focus groups with social partners and key figures will depend on what is feasible and acceptable in a specific phase of the research.
Data analysis for observations, semi-structured interviews, and group discussions
Data will be transcribed and thematically analysed in NVivo, following a six-phase approach: familiarising ourselves with the data by transcribing and rereading it, generating initial codes, searching for themes, reviewing potential themes, defining the themes and naming them, and reporting the results. 26 The thematic analysis will be conducted both deductively following the Consolidated Framework for Implementation Research 27 and inductively, comprising new themes that emerge from the data.
Data collection methods for the outcome evaluation
Pre–post survey
Survey population: We take a random sample of approximately 1,000 inhabitants who are 18 years or older in each neighbourhood.
Aim and timing: The survey measures seven concepts (i.e. perceived neighbourhood social cohesion; perceived help from neighbours; generic neighbourhood participation; neighbourhood participation around illness, caring, death, and loss; self-efficacy around dealing with illness, caring, dying, and loss; personal experiences with these topics; and experiential learning). The survey will be administered at two points in time: pre-implementation, to have a baseline measurement of what people already do around serious illness, death, and loss in their neighbourhood, and post-implementation to measure the impact of CEIN.
Data collection procedure: Respondents can choose to fill in a paper version of the survey and send it back via a pre-paid envelope or fill in the online survey. To guarantee confidentiality, each survey contains a unique respondent number. Distribution of the survey and reminders sent is based on the Total Design Method. 28 The stakeholders will be asked if they want to add questions to the survey regarding their interests in CEIN.
Analysis: The data will be subjected to descriptive and inferential statistical analyses in SPSS.
Ego network mapping
Aim: Ego network mapping will be conducted to measure if the social support network of people in the two neighbourhoods increased as a result of CEIN.
Data collection: Via a semi-structured interview, participants will be asked about their supportive network of friends and family but especially of people in their neighbourhood. This network will be illustrated on a map with circles, which represents the closeness of each of these supportive actors. In addition, data will be collected to gain insight into people’s current support needs, satisfaction with their current network and insight into which people have the potential of being included in their network.
Timing: Before and after the implementation of CEIN.
Analysis: The drawn networks will be compared quantitatively on the number of people and their closeness. The qualitative data will be thematically analysed.
Most significant change sessions
Aim: Most Significant Change sessions will be conducted to measure the outcomes of the study qualitatively. This method enables us to capture unexpected experiences and outcomes of the CEIN study, and the most salient ones.
Data collection: Most Significant Change stories are collected through group discussions with the stakeholders that are involved in the CEIN study. The story that is most significant is chosen by iterative voting.
Timing: The Most Significant Change session will be conducted at the end of the study.
Analysis: The significant change stories will be transcribed and thematically analysed. 26
Synthesising the data
Applying a critical realist lens to the data synthesis, we aim to first identify mechanisms of change that are context-specific of the two CEIN neighbourhoods and then combine these data into generalised insights and interpretations. 18 We use a convergent-parallel mixed-method research design in which we will simultaneously collect qualitative and quantitative data that we analyse and report upon separately but in the last phase narratively synthesise. 20 We will describe per neighbourhood the context and the development of the CEIN initiatives, resulting in descriptive themes which we will put into the first column of a joint display; a second column will include the qualitative findings on that specific theme, a third column will include the quantitative findings and a fourth column will describe the inferences.22,29 When there is a discordance between the qualitative and quantitative findings, we will seek for explanations in literature.22,29
Discussion
Worldwide, more and more neighbourhood civic engagement initiatives regarding serious illness, dying, and loss are emerging. Although most of the published initiatives have been evaluated, the methodological choices are often not described or explained or they have methodological shortcomings (e.g. focusing either on processes or outcomes). 8 This article presents the design and data collection methods of the CEIN study, a study aiming to evaluate the development and implementation of civic engagement actions in serious illness, death, and loss in two neighbourhoods. It includes a methodology to capture complex social change in serious illness, death, and loss via a convergent mixed-method process and outcome evaluation. The research is situated within a critical realist paradigm that includes the socio-ecologic factors of the study and uses a logic model as an instrument to guide the evaluation process. Furthermore, the protocol describes different data collection methods (e.g. observations, interviews, and ego network mapping) that can be used to evaluate the CEIN initiatives.
Literature shows that in asset-based community development research, social reality is so complex that a thorough process evaluation is necessary to fully understand which mechanisms are at play. 30 Since the development of CEIN is a co-creative process with stakeholders, their collaboration in the development is naturally the first factor to be considered in the process evaluation (e.g. their intrinsic motivation and their thoughts on developing actions). However, there is an increasing realisation that social change is not only accomplished within the co-creative process itself but that the context of development is an equally important factor. 31 The fact that the CEIN study is initiated in two Compassionate Cities, in which there is also city-wide attention for the topics of serious illness, death, and loss, influences the development of CEIN initiatives. Consequently, we started this protocol from a critical realist paradigm with attention to the broader socio-ecological context of the project, e.g., the city policy, the political landscape of the city, the community capacity and readiness to engage in the study. In light of replicating the CEIN study, and Compassionate Communities in general, we believe there is great value in documenting and describing these contextual factors and sharing them internationally.
Compassionate Communities, including CEIN, generally aim to increase people’s capacity to deal with serious illness, death, and loss; thereby aspiring for social change in the community. 11 However, since a social change in serious illness, death, and loss, is very complex and dependent on the context, it can be operationalised in many different ways.32,33 A first implication is that a flexible and adaptive attitude is required from the researcher, who at the start of the study has no full knowledge of the outcomes that will be formulated by the community and the initiatives that will be developed. 34 A logic model can assist in closing the disparity between community actions and the desired social change, by displaying their interconnectedness. In addition, the chosen data collection methods should be used flexibly to capture the dynamic aspects of social change and should be adaptable to what we want to measure in a specific phase of the research. We argue there is added value in documenting the adaptations that were made in the data collection process. This study protocol is the first step in documenting this for the CEIN study. In addition, we consider international discussions on the operationalisation of social change essential to inspire the development of CEIN initiatives and to guide how to evaluate them.
Strengths and limitations
This study protocol is the first to describe a convergent mixed-method process and outcome evaluation for evaluating Compassionate Communities, to present a range of possible data collection methods and to provide a reflection on the flexibility with which they should be applied. In addition, this protocol suggests instruments that offer guidance and control in evaluating complex and dynamic social change programmes, i.e. a critical realist paradigm that connects the context of the study to its impact and mechanisms of impact and a logic model that reinforces this evaluation paradigm by visually demonstrating the interconnectedness of the community actions and their impact. Challenges of evaluating neighbourhood civic engagement initiatives regarding serious illness, death, and loss are the flexibility needed to adapt the data collection methods to the specific context of the study, and the flexibility of the researcher in applying these dynamic data collection methods.
Conclusion
This study protocol describes a process-and-outcome evaluation that can serve as an inspiration for others who aspire to evaluate similar initiatives. We emphasise the importance of a process to fully understand the contextual factors of the study, the mechanisms that lead to impact and to stimulate a successful replication of Compassionate Communities in different contexts. Furthermore, this protocol shows the difficulty of operationalising the desired long-term impact of social changes regarding serious illness, death, and loss into more manageable outcomes, and subsequently into more specific community actions. We recommend a well-cogitated logic model that connects the short-, middle-, and long-term outcomes of the study to the potential actions that are being developed. In addition, we highlight the need for a flexible attitude of the researcher in adapting data collection to what is feasible or acceptable in a particular context. International discussions on how to operationalise and capture social changes in serious illness, dying, and loss are needed to inspire civic engagement initiatives around serious illness, death, and loss and their evaluation. Applying such a study protocol in practice is a constant exercise between providing sufficient flexibility to adapt it to a specific context and providing sufficient guidelines to structure and control the evaluation.