
Abstract
Background:
Integrated palliative home care (IHPC) is delivered to patients with progressive end-stage diseases. During the COVID-19 pandemic, IHPC needed to provide high-quality home care services for patients who were treated at home, with the goal of avoiding unnecessary care, hospital admissions, and emergency department (ED) visits. This study aimed to compare the ED visits of IHPC recipients in a large Italian region before and during the first two waves of the COVID-19 pandemic and to find sociodemographic or clinical characteristics associated with changes in ED visits during the first two waves of COVID-19 pandemic, compared with the period before.
Methods:
Administrative databases were used to identify sociodemographic and clinical variables of IHPC recipients admitted before and during the pandemic. The obtained data were balanced by applying a propensity score. The average number of ED visits before and during the pandemic was calculated by using the Welch’s t test and stratified by all the variables.
Results:
Before and during the pandemic, 5155 and 3177 recipients were admitted to IHPC, respectively. These individuals were primarily affected by neoplasms. ED visits of IHPC recipients reduced from 1346 to 467 before and during the pandemic, respectively. A reduced mortality among IHCP patients who had at least one ED visit during the pandemic (8% during the pandemic versus 15% before the pandemic) was found. The average number of ED visits decreased during the pandemic [0.143, confidence interval (CI) = (0.128–0.158) versus 0.264, CI = (0.242–0.286) before the pandemic; p < 0.001] for all ages and IHPC duration classes. The presence of a formal caregiver led to a significant decrease in ED use. Medium and high emergency ED admissions showed no difference, whereas a decrease in low-level emergency ED admissions during the pandemic [1.27, CI = (1.194–1.345) versus 1.439, CI = (1.3–1.579) before the pandemic; p = 0.036] was found.
Conclusion:
ED visits among IHPC recipients were significantly decreased during the first two waves of the COVID-19 pandemic, especially in those individuals characterized by a low level of emergency. This did not result in an increase in mortality among IHPC recipients. These findings could inform the reorganization of home care services after the pandemic.
Keywords
Introduction
Palliative care has been developed in recent decades as a social movement and a medical specialty that addresses the physical, psychosocial, and spiritual needs of those individuals with life-threatening illnesses and their families. 1 In Italy, palliative care was officially recognized by the National Law 38/2010, 2 which guarantees the right of access to patients with progressive end-stage diseases, such as neoplasms, heart failure, chronic obstructive pulmonary disease, and dementia. 3 This type of care is provided in each of the 20 regions of Italy in multiple settings, including hospices, hospitals, residential facilities, and at home, wherein it is referred to as integrated palliative home care (IHPC).
In Italy, IHPC is initiated following the request of the general practitioner, and it is delivered and administered by palliative care units, which create multiprofessional teams that ensure medical, nursing, rehabilitation, social and psychological support, pharmaceutical assistance, and diagnostic tests. The multiprofessional teams evaluate whether a recipient can receive IHPC based on multiprofessional assessment measures, and they then prepare an individual care plan. This plan must be shared with the recipient and their family and caregivers, as it constitutes a therapeutic care contract. The individual care plan aims to identify the goals of care and the most appropriate interventions in the case of any issue, as well as to guarantee a comprehensive, coordinated approach across different health care professionals, thus avoiding unnecessary care, hospital admissions, and emergency department (ED) visits.
Similar to any other health care system setting, the palliative home care program has also been influenced by the COVID-19 pandemic, albeit lacking evidence in the international literature. Indeed, an Italian study 4 highlighted that some research focused on the crucial role of palliative care in managing individuals who were seriously infected during the COVID-19 pandemic,5–7 but few studies have investigated the impact of the pandemic on palliative care services.4,8,9 As it was clear from the early stages of the pandemic that hospital care services could quickly become a critical resource, it was also necessary to maintain high-quality home care services (whenever possible) for recipients who were treated at home during such period. For this reason, home care workflows were necessarily replanned in terms of the readaptation of processes, flexibility, and precautions with the recipients. 10
From this perspective, it could be valuable to evaluate whether IHPC recipients had reduced ED visits in 2020 during the first two waves of the COVID-19 pandemic, compared with 2019. This is due to the fact that Italy was the first European country to be seriously affected by COVID-19, with an exponential increase in infections and deaths. In February 2020, a few positive cases of COVID-19 were reported in northern Italy; by the beginning of March 2020, the virus had spread to all Italian regions, with particularly severe infection incidence rates in northern regions, 11 as Piedmont. The Piedmont region is the second largest of Italy’s 20 regions, covering an area of 25,300 km2 in the north-west of the country, and the seventh most populated (4.3 million inhabitants). IHPC recipients in Piedmont receive the same care provision in each of the 20 regions of Italy, as the service and its organization are designed on a national basis. As far as we know, ED visits among IHPC recipients have been understudied in Italy. It might be possible that, as reported for the general population, ED visits also have reduced for IHPC recipients during the early stages of the COVID-19 pandemic. Furthermore, sociodemographic and clinical characteristics of IHPC recipients could have been associated with a reduction in ED visits in this particular population. Therefore, the primary aim of this study was to compare the ED visits of IHPC recipients in a large northern region of Italy before and during the first two waves of the COVID-19 pandemic, analyzing if there has been a reduction of these visits during the first phase of the pandemic. Another objective of this study was to find any sociodemographic or clinical characteristics associated with a change in ED visits during the first two waves of the COVID-19 pandemic, compared with the period before.
Methods
We collected the data of all the individuals who were admitted to the IHPC program of Piedmont from 1 March 2020 to 31 October 2020 (during the first two waves of the pandemic), which encompassed the peak months of the COVID-19 pandemic in Italy. After the first outbreak and consequent decrease in the infection rate from May 2020 and during the summer season, Italy experienced a sudden increase in cases and hospitalizations during September and October 2020. 12 Comparable data were also examined from the same time interval in 2019, from 1 March to 31 October (before the pandemic).
Data concerning the recipients and ED use were collected by merging two different sources: the Italian Official National Information System for Monitoring Palliative Home Care Services (the SIAD database) and the Italian National Information System for ED use database.
Data were collected for the following sociodemographic variables: sex, age, and presence of a formal caregiver. Age was stratified into four age groups (⩽65, 65–80, 81–90, and ⩾91 years of age). The following clinical variables were collected: outcome (alive or dead), principal diagnosis at IHPC admission (as defined by the International Classification of Diseases, Ninth Revision), triage assessment, and principal diagnosis at the time of ED admission. Moreover, the IHPC duration in days (⩽30, 31–90, and >90 days) and the arrival mode to the ED (autonomous, ambulance, or other modes) were collected.
The Italian triage assessment 13 is based on a four-color code evaluation with the goal of a rapid determination of safe and comprehensible treatment priorities. Specifically, white defines noncritically ill patients who do not need treatment in a short time; green defines minimally critically ill patients whose interventions can be postponed; yellow defines moderately critically ill patients whose interventions cannot be postponed; and red defines highly critically ill patients who need immediate emergency interventions. White and green indicate a low level of emergency, whereas yellow and red indicate a medium and high level of emergency, respectively.
Moreover, the principal symptoms at the time of the ED visit were recorded during each triage examination per recipient. For the purposes of this study, eight different types of the most recurrent symptoms that are included on the Italian National Information System for ED use were categorized as follows: abdominal pain, dyspnea, traumatic problems, fever, cardiac rhythm alteration, urological symptoms, neurological symptoms, and undefined symptoms.
All the data originated from the Health Information System of the Piedmont region, which was designed and administered to comply with the regional, national, and European regulations regarding the protection of personal data; in addition, it is used in support of the evaluation and monitoring of activities of the Piedmont region.
Data from these databases were merged by using the universal patient ID number, which is an anonymous, unique code that is centrally assigned to each patient. The data treatment phases have been exclusively performed by delegates of the regional epidemiology network (of which the Unit of Epidemiology-Regional Health Service-Local Health Unit TO3 is a node) who are in charge of the processing data for supporting regional evaluations stated in the regional regulation. 14 A formal agreement regulates the cooperation between the units that were involved in this study. Therefore, ethics committee approval was unnecessary.
Statistical analysis
To guarantee that no confounding effect could arise because of age and sex imbalances between the two time periods, a propensity score (PS) balancing method was applied to preprocess the data. The PS method has been implemented in R by using the WeigthIt package 15 to create equivalent groups in the observations with entropy balancing, 16 thus better balancing the covariates and minimizing the overdispersion of the weights that had been computed thus far.
After balancing the population, we resorted to an independent sample test for the two groups (the Welch’s t test) to compare 2019 versus 2020 populations. The Welch’s t test is a two-sample test that is used to test the hypothesis that two populations have equal means, and it is more reliable than the Student’s t test when the two samples have unequal variances and/or unequal sample sizes. 17
The test is also supported by the Bayes factor computation. Specifically, this method can make more robust assumptions by helping to index evidence in favor of the null hypothesis if it cannot be rejected with the standard null hypothesis significance test approach.
The average numbers of ED visits before and during the pandemic periods were calculated. Analyses were stratified by all the variables.
All the analyses were performed by using the R package version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p < 0.05 and 95% confidence intervals (CIs).
Results
IHPC recipients’ characteristics and ED visits
A total of 5155 recipients were admitted to IHPC in 2019, and 3177 individuals were admitted in 2020. The characteristics of these two populations are shown in Table 1. The most noticeable differences among the groups were related to the IHPC duration, with 17.23% of the 2019 recipients compared with 11.61% of the 2020 recipients having a long (>90 days) IHPC duration, as well as the number of deaths (28.4% in 2019 versus 35.76% in 2020). For both groups, the principal diagnosis at IHPC admission was neoplasm (81.53% in 2019 and 84.95% in 2020).
Characteristics of the 2019 and 2020 IHPC populations.
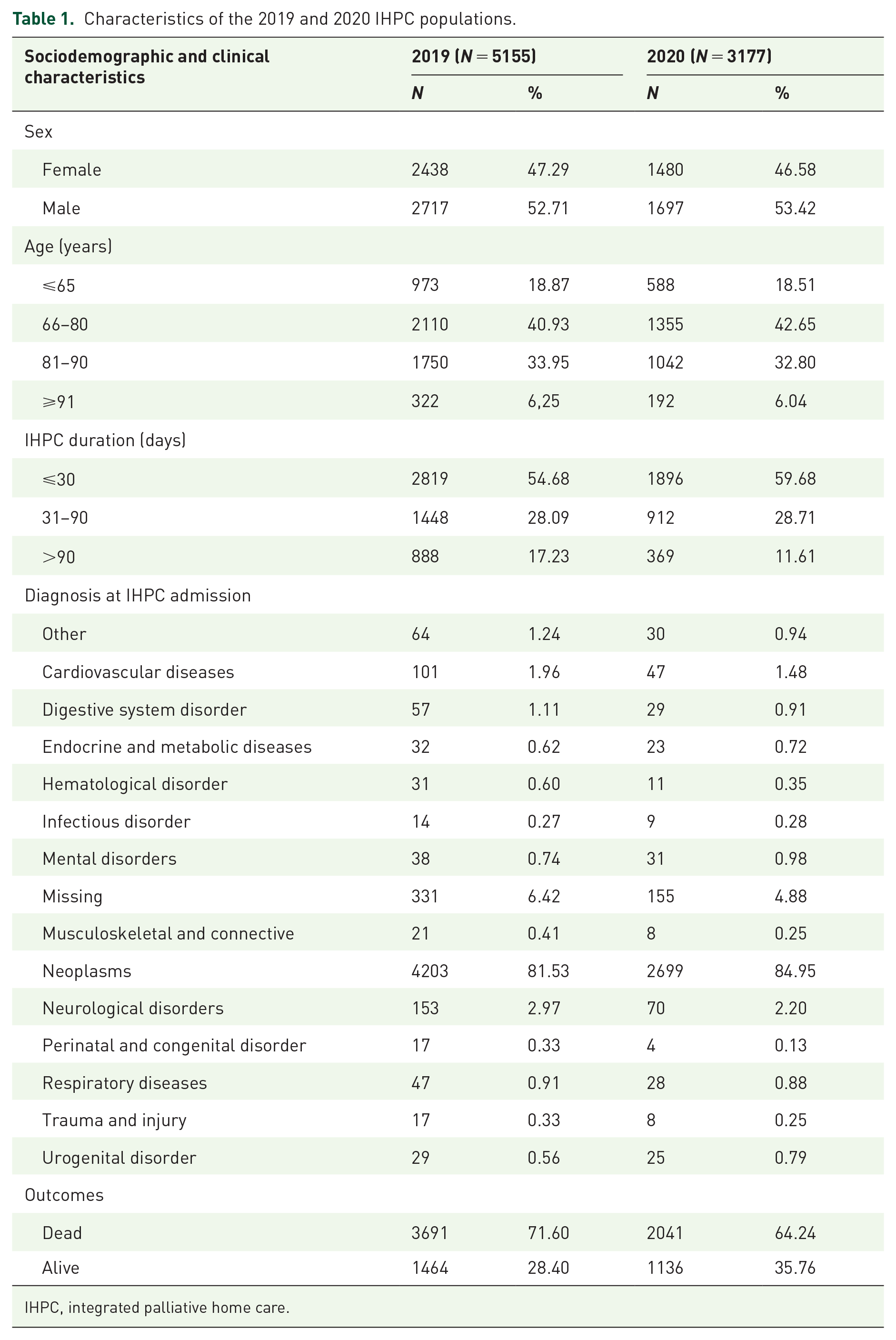
IHPC, integrated palliative home care.
The total numbers of ED visits of the IHPC recipients were 1346 in 2019 and 467 in 2020. A considerable number (20.4%; n = 1054) of IHPC recipients had at least one ED visit in 2019, whereas this number decreased to 12.1% (n = 383) in 2020. In particular, 15.39% of the IHPC patients who died in 2019 and 8.77% of those who died in 2020 had at least one ED visit.
ED visits before versus during the COVID-19 pandemic
The average number of ED visits among the IHPC recipients was reduced in 2020 compared with 2019 [0.264, CI = (0.242–0.286) in 2019 and 0.143, CI = (0.128–0.158) in 2020; p < 0.001].
The observed reduction in the average number of ED visits was affected by several variables (Table 2).
Comparison of the average number of ED visits in the 2019 and 2020 IHPC populations.
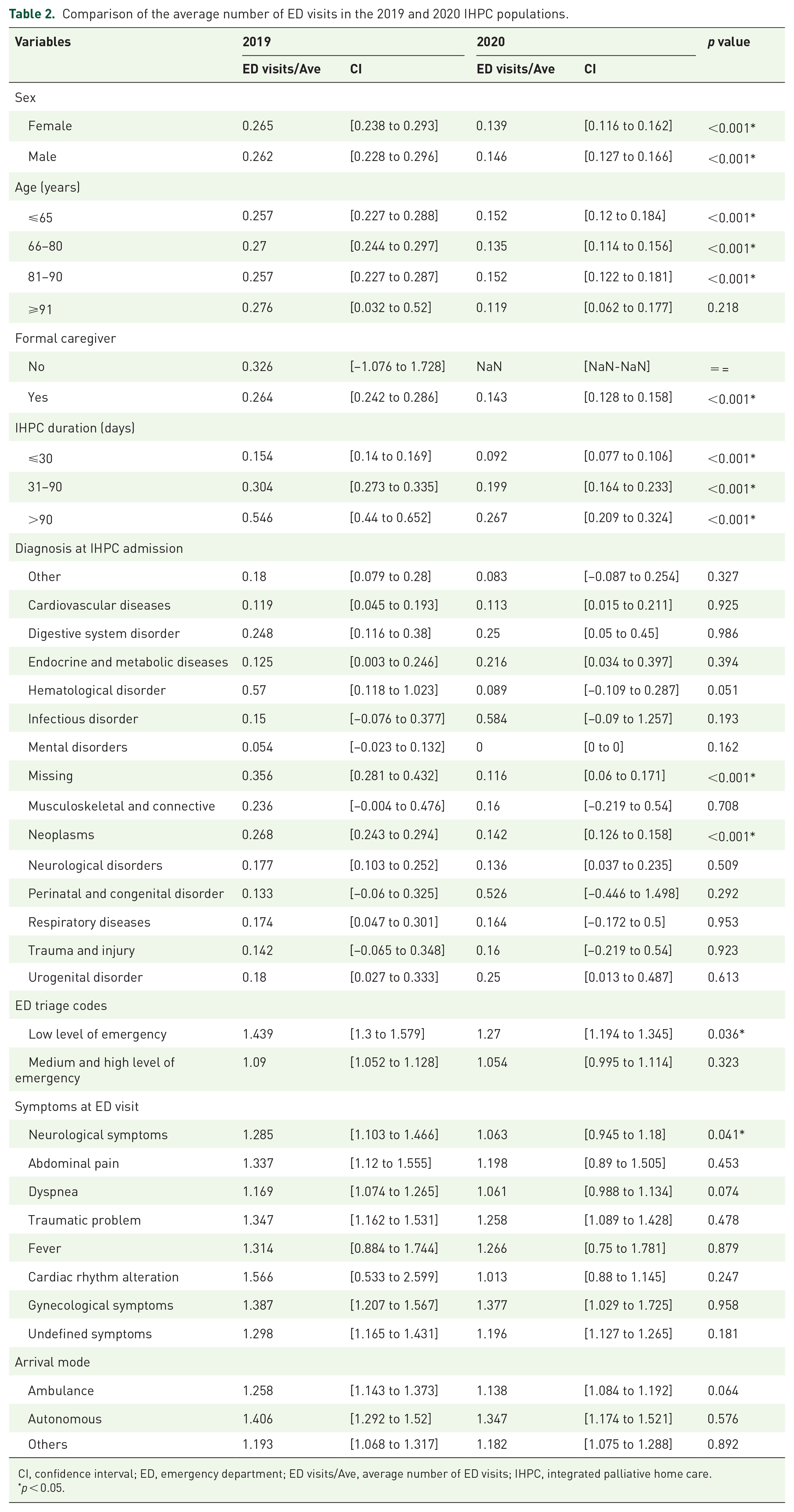
CI, confidence interval; ED, emergency department; ED visits/Ave, average number of ED visits; IHPC, integrated palliative home care.
p < 0.05.
The average number of ED visits was reduced in 2020 for female and male recipients, for all age classes (except for those individuals aged >91 years), and for all IHPC duration classes. In addition, the presence of a formal caregiver led to a significant decrease in ED use [from 0.264, CI = (0.242–0.286) in 2019 to 0.143, CI = (0.128–0.158) in 2020; p < 0.001]. No significant differences were found in the arrival mode to the ED among the groups.
IHPC recipients with neoplasms and missing principal diagnoses at the time of IHPC admission showed a significantly lower number of ED visits in 2020 than in 2019 [from 0.268, CI = (0.243–0.294) in 2019 to 0.142, CI = (0.126–0.158) in 2020 for neoplasms; from 0.356, CI = (0.281–0.432) in 2019 to 0.116, CI = (0.06–0.171) in 2020 for missing diagnoses].
No principal symptoms recorded at the time of the ED visits were significantly different among the IHPC recipient groups, except for a decrease in neurological symptoms [from 1.285, CI = (1.103–1.466) in 2019 to 1.063, CI = (0.945–1.18) in 2020; p = 0.04].
When accounting for the triage tags, which indicates the level of the emergency at the time of ED admission, the average number of ED visits with a low level of emergency significantly decreased in 2020 compared with 2019 [from 1.439, CI = (1.3–1.579) in 2019 to 1.27, CI = (1.194–1.345) in 2020; p = 0.036]. In contrast, the average number of medium and high emergency levels at the time of ED admission in 2020 showed no differences compared with 2019.
Discussion
This study aimed to describe the impact of the COVID-19 pandemic on ED visits among palliative care recipients in a large northern region of Italy. Our results highlighted the fact that during the early stages of the COVID-19 pandemic (when no vaccinations were available), there was a significant reduction in ED visits compared with 2019 among IHPC recipients. Our results confirm the general trend of a reduction in ED use during the pandemic compared with previous years, as has been observed in other studies.18–21 Furthermore, this reduction was mainly found for people with neoplasms, formal caregivers, and ED visits characterized by a low level of emergency.
The significant reduction that was observed in ED use for IHCP recipients with neoplasms during the COVID-19 pandemic could have different interpretations from both an individual and political perspective. Moreover, because of the fact that people with neoplasms represent a large majority of palliative care recipients, 22 a minor ED use by this population could explain the overall amount of reduced ED admissions that occurred during 2020 in our sample. In this regard, this reduction could be more pronounced in our sample, which almost entirely consisted of oncological care recipients. Nevertheless, this high ratio of people with neoplasms taken care of by IHPC is not surprising. In the Italian context, advanced nononcological diseases are usually enrolled in general home care services. Specifically, from a report from the Italian Ministry of Health, the rate of IHPC recipients with neoplasms was 80%, while those with other chronic conditions accounted for 20% in both 2016 and 2017. 23
People with neoplasms are frail and at higher risks for COVID-19 infection, which is frequently associated with complications, intensive care admission, and increased mortality.24,25 During the pandemic, more frail and more immunocompromised individuals could have felt anxious and afraid of being infected in health care facilities, thus leading them to reduce the use of medical services, such as ED. In this regard, a review by O’Rielly et al. 26 reported that during the early stages of the COVID-19 pandemic, many patients canceled or delayed their routine visits or procedures because of concerns with safety and nosocomial infections. National health policies may also have enhanced this trend. Indeed, significant efforts have been made throughout the world to reduce the risk of contagion in these individuals and to maintain the treatment of frail patients outside of health care facilities and hospitals. The Italian Ministry of Health and National Health Service (NHS) has recommended that the population should avoid being directly admitted to hospitals; instead, they should dial the emergency number dedicated to evaluating patients at home and decide on eventual transport to the hospital, thus giving priority to the access of EDs through emergency vehicles. 27 Even in the United Kingdom, during the first lockdown period, the public was instructed to ‘stay at home, save lives, and protect the NHS’. This resulted in increased anxiety in the population over visiting hospitals, and a higher use of emergency numbers and helplines occurred, 28 which resulted in a decline in the number of ED visits with minor health issues.19,28,29 Fear of contagion, the deterrence of accessing the ED, and the effect of travel restrictions likely led to seeking medical care for more severe conditions. Our finding supports the assumption that ED visits for medium and high emergency levels did not show a significant decrease during the COVID-19 pandemic. Although highlighted in a small population, the significant reduction in ED visits in oncologic IHPC recipients may be explained by the tendency to protect frail people during the first two waves of the COVID-19 pandemic.
In the midst of the COVID-19 pandemic, home palliative care teams may have played an essential role in providing care during a time period that was characterized by extensive changes in health care services while facing an emergency. In the home care setting, an infectious disease spread represents a severe problem from four points of view. The first view is the need to readjust care provision, adapt therapeutic processes, and guarantee flexibility. The second view is the risk of the patients being infected, which leads to the adoption of precautions with patients. 10 The third view is the risk of health care workers being infected, 10 whereas the fourth view is protecting the caregiver’s health, whose role was pivotal during the COVID-19 pandemic and whose contagion may limit the capacity to care for their patients. 30 In this context, ensuring continuity and quality of home care for patients, and reducing unnecessary hospital admissions and avoidable ED visits during a pandemic were essential and challenging aspects of health management. A common response by health care policies to the COVID-19 pandemic has been the digitalization of care via increased technological provisions and skill development by health care professionals, recipients, and their caregivers. 31 IHCP teams coped with new work challenges by adapting their usual care provision routines, improving their communication with caregivers, and implementing frequent phone or video calls for both recipients and colleagues. During the COVID-19 pandemic, the key messages from IHCP providers have been flexible, resilient, and able to rapidly implement new solutions in response to evolving care needs, such as by replacing traditional nurse visits with video consultations and improving compliance with medications and the education of the recipients. 32 The increase in telemedicine use contributed to an increase in virtual primary care consultations, thus filling the gap in primary care due to the COVID-19 pandemic.19,29,33 In our setting, a faster symptom assessment and the ability to communicate in real time by adjusting the medication regimen, combined with a lower number of IHCP recipients, may have contributed to a more timely response by IHCP teams, with the result of a reduced use of ED, especially for less severe emergencies.
The findings from this study showed that the presence of formal caregivers was associated with a significant reduction in ED visits during the COVID-19 pandemic. Previous evidence has shown that the presence of formal caregivers could reduce the risk of ED visits, as they are often trained in patient monitoring and supervision techniques, as well as being completely committed to their care and assistance.34,35 In addition, patients who rely on available and skilled caregivers have been shown to be significantly more inclined to meet health care goals. 36 Hence, it is plausible that during the COVID-19 pandemic, having a formal caregiver could have represented a protective factor to deal with symptoms and struggles that are treated in the home setting, instead of accessing the ED. The COVID-19 pandemic may have played a positive role in leading IHCP teams, recipients, and their caregivers to enhance symptom management at home,18,37 thus resulting in the referral of those urgent cases to the ED and limiting the use of emergency services for less acute visits. This is because, especially during the early stages of the COVID-19 pandemic, ED visits through emergency vehicles were exclusively directed to those infected or in life-threatening situations. 38 In this respect, the reduction in the mortality rate in 2020 compared with 2019 would appear to be congruent with the timely management of IHCP recipients that could potentially incur any clinical deterioration and, especially in the palliative care setting, experience secondary conditions to hospitalization. Our results may suggest that the forced response of IHCP teams to the COVID-19 pandemic positively influenced the care that is provided to IHCP recipients and their families. This may have been mediated by a more rapid response by IHCP teams to the needs of a smaller number of recipients and a better coordination with their caregivers.
Taken together, these results could prompt the conduction of studies aimed at testing the presence of a positive correlation between the pandemic and an improvement of the provision of IHPC at home, which could be suggested by the reduced low-acuity ED visits and reduced mortality. During the first wave of the COVID-19 pandemic, Italian mortality was high, exceeding 74,000 expected deaths in the Northern regions. 12 Because this increase was probably due to deaths related to COVID-19, it is conceivable that the opposite mortality trend we observed in IHPC recipients in the first two waves of the pandemic was due to better caring of this fragile population by home care services. This hypothesis could be explained by the forced resilience of home care services and the improved care delivery (which was not necessarily demonstrated in the presence of health care workers) that occurred during the most acute phase of the pandemic. On the other hand, there may have been unmet care needs by people necessitating IHPC, potentially leading to receiving such care, and deaths that were not detected.
Although supporting the hypotheses that during the early stages of the COVID-19 pandemic, ED visits among IHPC recipients decreased and that there were sociodemographic and clinical characteristics associated with this reduction, our study presented several limitations. The study population refers to a specific region of Northern Italy, and IHPC recipients were mostly people with neoplasms; therefore, our findings cannot be generalized to other regions or countries where the first two waves of the pandemic had a different spread or in which other models of palliative home care delivery were adopted. Moreover, our results are based on administrative databases and may correspondingly suffer in regard to coding accuracy because of clerical error and the limited precision of codes to describe conditions or procedures in detail. Finally, the examined administrative databases could not trace the number of home care visits made by the palliative care team. An in-depth study of the differences in providing such visits before and during the COVID-19 pandemic could comprehensively explain the reduced ED visits among IHPC recipients. While unable to provide a causal link between IHPC provision and reduced ED visits, which can be obtained only through longitudinal studies, our study represents the first investigation of this phenomenon during the early stages of the pandemic. Indeed, our focus on a cohort of patients who were admitted to the IHPC program, as well as the availability of data individually linked to administrative databases, represents a strength of our study because they provide evidence that the first two waves of COVID-19 have also had a significant impact on health service delivery at home.
Conclusion
This study demonstrated a significant reduction in ED visits among IHPC recipients during the COVID-19 pandemic, especially those individuals with neoplasms who relied on formal caregivers. Correspondingly, the ED visits characterized by a low level of emergency were significantly reduced. The decline in ED visits did not result in an increase in mortality among IHPC recipients. The rationalization of resources by identifying an appropriate ratio between IHPC providers and implementations aimed at improving telemedicine in palliative care represents future research topics in this area. Moreover, it would be worth understanding whether, in the Italian context, the reduction in ED visits from IHPC during the COVID-19 pandemic is comparable to that experienced in general home care. Future studies should demonstrate the efficacy of IHPC longitudinally in reducing the use of emergency services, providing policymakers with a broader perspective to enhance the delivery of care to all patients by strengthening IHPC teams. The adaptation of existing home care services by implementing innovative solutions should encourage health policies to maintain good practices adopted during the COVID-19 pandemic, thus reducing the burden on emergency services and improving the care of recipients and their families.