
Abstract
Background:
To contribute with knowledge to health policy development, this article presents a critical discourse analysis of two Norwegian official reports on palliative care published in 1999 and 2017.
Methods:
We identify, describe and discuss how linguistic features in policy documents contribute to and engender a distinct change from 1999 to 2017 in how patients are framed, documenting the development of palliative care.
Results:
The analysis identifies and considers two interwoven discourses: the discourse of accountability and the discourse of complexity. The patient moves from being described as in need of care, in the 1999 report, to being described as an active and responsible patient making proper choices, in the 2017 report.
Conclusion:
Result of this policy development might be less involvement of professionals and focus on existential questions, and more responsibility on patients for their prospective wellbeing and health: a change that we argue should be considered and counteracted in upcoming policy processes considering palliative care.
Introduction
Annually, close to 57 million people are in need of palliative care. 1 The World Health Organization (WHO) estimates that because of the ageing population and the rising prevalence of non-communicable diseases, the need for palliative care services will continue to grow. 2 This article discusses some related changes in how authorities approach palliative care, using the case of Norway and analysing two official policy documents on the subject.3,4 The article’s analytical framework and findings make it relevant to a broader audience interested in the study of policy discourses and changing palliative care policies in comparable countries.
Governmental support and grants are fundamental components of developing palliative care services. Related policies include laws, national standards for health, strategies on palliative care implementation and clinical guidelines. 5 A global programme has been monitoring country-level development in palliative care since 2006, with the last update taking place in 2017. 6 This mapping found continuously large variations among the 198 countries that were monitored. One indicator of quality in palliative care is the existence of a national strategy or plan. 6 Norway meets this requirement and is included by mapping in a group of 30 countries categorised as having ‘advanced integrated palliative care in health care services’. 1
In Norway, the Ministry of Health and Care Services first launched palliative care policies through an official report in 1984 and then later in 1999 and 2017. Norwegian official reports (NOU) deal with complex policy questions of national importance 7 and are the products of nominated committees. These committees investigate specific policy-related challenges and problems and propose appropriate solutions based on a thorough examination of the issue. The committees’ advice mainly feeds into the policy formulation stage before the government proposes the concrete results. In 2020, the Norwegian government launched its first white paper 8 on palliative care, building on the NOU from 2017. This event was an important way to concretise the future of palliative care in Norway. In analysing palliative care policy changes over time, we decided to examine and compare similar NOUs.
Policy texts, such as NOUs, are charged with assumptions and claims about the subject matter, relating meaningfully to former and contemporary public documents; the object of this article is to identify how language figures as an element in political and social change in the field of palliative care. We identify, describe, and discuss how linguistic features contribute to discourses about palliative care in the NOUs from 1999 and from 2017 (hereafter, the NOU1999 and NOU2017). By examining and comparing these two policy documents published 18 years apart, we identify and critically discuss the emergence of new concepts and strategies in Norwegian palliative care and their possible effects: effects that we argue should be considered and counteracted in upcoming policy processes considering palliative care.
Methodology
As tools for government, policy documents play a key role in the development, maintenance, and circulation of particular discourses. 9 Discourse analysis is a useful tool to challenge taken-for-granted views, assumptions, and knowledge at play in policy documents in general 10 and to reveal powerful meanings in palliative care policies in particular.11–14 We apply the critical discourse analysis (CDA) framework developed by Fairclough,9,15 who sees language as both a symptom and a cause of social change. For the purpose of this analysis, we understand ‘palliative care discourses’ as the analytical groupings of utterances, sentences, or statements that are enacted within and determined by a particular social context: here, the field of palliative care. 16 Drawing from the two NOUs under study, we describe how palliative care is approached and framed and investigate how different stakeholders (authorities, professionals, and patients) are described, highlighted, and empowered. Furthermore, we discuss some of the possible consequences of these embedded discourses.
Initially, we read the two reports entirely and thoroughly to familiarise ourselves with their content and to gain a sense of the embedded aims and messages in both documents. We then extracted central concepts, themes, that organised our observations to enable the comparison of the two documents. The NOU1999 establishes a context, that is, a background, which enables to identify changes in the pattern of language use and that which is discursively at stake in the NOU2017. Both reports are available in Norwegian only; for present purposes, we translated relevant passages into English.
Both authors are qualified nurses; one is an experienced researcher in health service palliative care studies and the other is an experienced critical policy discourse analyst with no previous exposure to the field of palliative care. As such, the analysis captures both an ‘insider’s’ close-up perspective and an outsider’s objective perspective.17,18
Textual corpus
As established above, our key documents are NOUs 1999:10, ‘Help to live. Treatment and care to incurably ill and dying’ 3 and 2017:16, ‘On life and death. Palliative care for severely ill and dying’. 4 As in many other countries, the development of care for severely ill and dying patients in Norway is influenced by Cicely Saunders’ concerns surrounding the medical neglect of the dying and her innovative ideas regarding how end-of-life care could be improved. 19 An open attitude towards death that involves the patient and family and offers holistic care to meet the patient’s total pain while managing related symptoms 20 was the main idea that came to affect the development of terminal and palliative care in Norway. However, these ideas evolved over time, and the NOU1999 can be understood in the context of a transition from the phase of pioneering and establishing palliative care in Norway to the phase of organisation and professionalisation. 19 Over the years, the development of Norwegian palliative health care policies and services has included the description of, and involved, more specially trained health care professionals. As such, the NOU2017 is imbued with scientific knowledge and professionals’ experiences, constructing an even more professionalised context for the field. 21 The publications of these NOUs were important discursive events in Norwegian palliative care policy development, as these documents were likely to be widely read and acted upon by professionals and other stakeholders in the field. The mandates for both committees were issued by the health care minister at the time, and they were more or less similar, assessing contemporary palliative care in Norway and suggesting improvements through better organisation and education.3,4
Analysis
The linguistic analysis and comparison of these two NOUs drew attention to the way particular words and concepts were high on the agenda of one NOU but not the other. The included table illustrates important examples of these differences.
The two documents have some obvious differences. First, the number of pages doubled from 98 in the 1999 report to 198 in the 2017 report. The reference lists spread over one and nine pages, respectively. The NOU1999 mostly refers to statistics, juridical regulations, and governmental documents. The NOU2017 adds Norwegian and international research, as well as various guidelines on palliative care. As such, the NOU2017 mirrors the ‘expertisation’ 22 of policy making, meaning the authorities’ responsibility to react to, control and eliminate medical conditions, alongside its trend towards becoming increasingly evidence-based. 7
The NOU1999 consists of 14 chapters addressing, for instance, former national and international palliative care policy, central concepts (‘help to live’, palliative care and quality of life), legal grounds and suggestions for future palliative care health services. In a separate section, a historical and theoretical reflection on dying and death is included. In this section, chapter 5, ‘Values and attitudes’, situates the concepts of dying and death in their historical context and points to both national and international developments. It highlights Philippe Aries’ historical presentation of Western death mentalities 23 and refers to changing Norwegian perspectives and traditions. 24 We mention this section as in the NOU2017, the use of the term ‘dying/death’ has decreased considerably and lacks this broader historical framing. This change might be related to a biomedicalisation of palliative care and a focus on treatment of symptoms rather than on existential questions.
Furthermore, the NOU1999 describes challenges in palliative care related to issues of communication, information and competence. Providing concrete solutions, the document suggests increased efforts in producing education and research. Simultaneously, the NOU1999 introduces a novel concept: ‘help to live’ [Norwegian ‘livshjelp’]. The document defines ‘help to live’ as a professional approach to addressing anxiety, depression and pain in palliative patients, decreasing feelings of redundancy and burdening others. The objective of the ‘help to live’ initiative is to provide proper care that is guided by values and ideals based in humanity, solidarity, respect, commitment and empathy. 3 By being helped to live, patients will be guided towards experiencing the last phase of life as meaningful rather than unbearable. The NOU1999 explains that many patients in the palliative phase no longer wish to live, longing for death, and some will also ask for permission and help to die. A ‘help to live’ approach rather emphasises the importance of professionals, a multidisciplinary team surrounding the patient with ‘all-embracing care’. 25 The concept of ‘help to live’ is not found in the NOU2017, which we argue confirms the document’s rooting in the biomedical genre. This means that, in contrast to the NOU1999, where questions concerning euthanasia are met with the ‘help to live’ intervention, the NOU2017 does not mention issues concerning euthanasia at all.
In comparison, the NOU2017 is divided into 15 chapters that address a range of medical, ethical and legal issues. Featuring a nine-page list of citations and three attachments, the document is rooted in the biomedical field. For that reason, the report is less likely to appeal to lay readers, such as patients, relatives or volunteers, despite the importance of the responsibilities that are assigned to them. The report’s first page calls for a turn from a disease-centred approach towards a patient-centred approach in palliative care. A focus on individual’s symptoms and problems reflects the biomedical acknowledgement of what is considered normal, and the reasoning that individuals must be involved in processes of treatment. This shift and suggestions for future developments are considered in chapter 5, ‘Perspectives’. Here, the report describes contemporary shifts from paternalism to patient involvement, from palliative care being mainly for cancer patients to including a diversity of diagnoses and patients, and from mainly addressing end-of-life care needs to becoming an integrated part of the illness trajectory.
The document upholds the strategy of a patient-centred approach throughout the text, addressing the ‘patient’ or ‘user’ repeatedly (see Table 1). To the word ‘patient’, words such as ‘autonomy’, ‘involvement’, ‘preferences’, ‘choice’ and ‘tailored pathways’ are appended. Chapter 4, named ‘Values’, addresses patient autonomy and patient involvement in planning for health care and decision-making as main ideals of the report. This chapter explains that patient autonomy is an approach to caring for the severely ill and the dying, describing ways of handling patient involvement and choice with reference to advance care planning: Advance care planning enables individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with family and health-care providers, and to record and review these preferences if appropriate. (p. 33)
Numbers of particular words and concepts in NOU1999 and NOU2017.
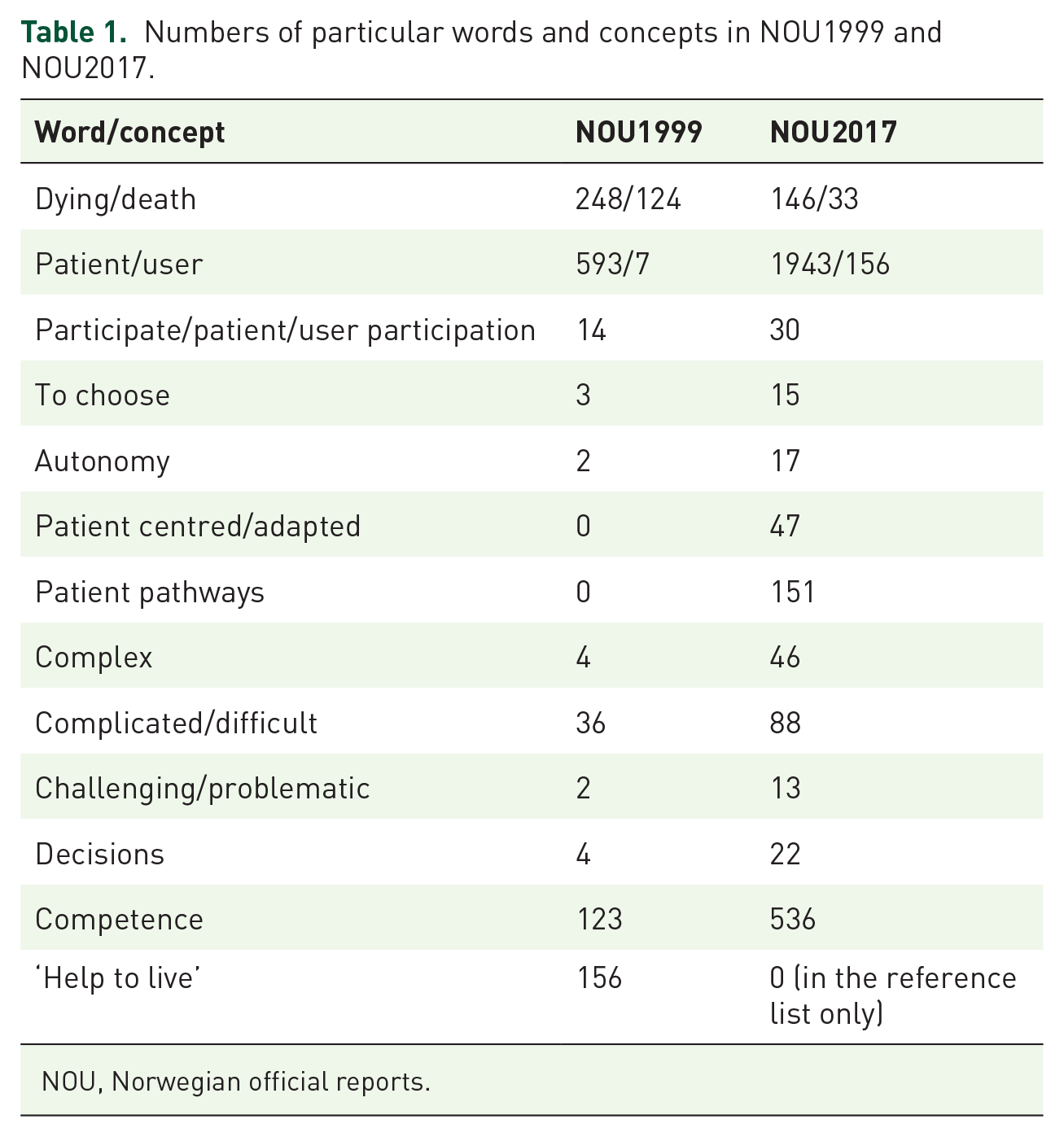
NOU, Norwegian official reports.
Echoing these ideas, chapter 6 (‘Patient-tailored pathways’) introduces palliative care pathways to improve these services, with detailed advance care plans safeguarding and guiding palliative treatment (p. 61). The chapter simultaneously highlights how patients’ preferences can be best be identified and incorporated in such predefined treatment courses. Like the NOU1999, the NOU2017 9 proposes increased efforts to provide courses, educate professionals and advance research to improve palliative care services in Norway.
Generating a total impression based on different analytical steps led to the identification and construction of two interwoven key discourses: 9 a discourse of accountability and a discourse of complexity. The discourses will be further analysed and discussed in the following section.
Results and discussion
In line with the CDA framework, 9 the analysis identified two interwoven key discourses in the development of palliative care policies.
The discourse of accountability
The discourse of accountability includes taking responsibility for one’s own actions.
26
The changing patterns of language used in the NOU1999 and the NOU2017 construe a contemporary and novel role for the patient in Norwegian palliative care. Instead of being described as a patient in need for care or ‘help to live’, as is the mantra in the 1999 report, the patient in the 2017 report is an active and responsible patient making proper choices, in accordance with the authorities’ advice. Our observation fits with what Borgstrøm and Walter refer to as the ‘choice discourse or agenda within English end-of-life care policy’ in 2008.13,27 They argue that the shift towards individuality is a remarkable change in English health-based political strategies, as the word choice was not found to the same extent in comparable strategies from other Anglophone countries at that time. Nine years later, the Norwegian policies also apply this same rhetoric, presenting individuals who receive palliative care as capable and competent individuals able to choose their own actions over the course of their disease. We see this development as a marker of authorities’ governance to empower individuals, in line with the current global health development consensus.
28
However, with the NOU2017’s empowering strategy, we identified an additional transfer of responsibility to patients in treatment and care processes: Health care personnel must actively facilitate [patient] participation. The anticipation that the patient must take on responsibility in his or her treatment and care must be made clear. One reason for this is that patient participation will improve the quality of health care services. (p. 29)
The report understands the patients not only as capable and competent but also as a contributor to their palliative care process. Diverging from the representation of the patient as a receiver of treatment and care, the political subject becomes an individual whose citizenship is active and manifest in their pursuit of personal fulfilment. 29 The discourses embedded in the NOU2017 thus seem to assume that the patient can understand and foresee all aspects of the disease, including symptoms, pros and cons of treatment options, and even future challenges. In this way, the report assigns discretionary powers to health professionals to activate the patient, a task superior to that of providing care. Originating in ideas of service quality, the document imposes responsibility on professionals to engage patients as accountable partners in the process. From a Foucauldian perspective, 30 this development engenders a paradox; while still characterising palliative care as highly complex (as will be further elaborated below), the discourse of accountability legitimises a partial transfer of responsibility from the professionals to the individual in this difficult and demanding phase of their life.
We contend that there is a flaw in how the NOU2017 construes the self-confident, autonomous individual, as living with severe and life-threatening illness often entails chaos, vulnerability, frailty and death, all of which limit an individual’s sense of choice and control.13,31,32
The discourse of complexity
The analysis also identified the emergence of a discourse of complexity in developing palliative care policies. Barely mentioned in the NOU1999, as evidenced by Table 1, the use of the word complex increases significantly in the NOU2017. Examples include: ‘Patients’ experiences involve a complex set of feelings, meanings and expressions’ (p. 12); ‘Palliative needs are complex’ (p. 13); ‘The clinical picture is complex’ (p. 14); ‘The conditions are complex’ (p. 14); ‘The treatment is complex’ (p. 42); and ‘Complexity increases with the number of actors involved, the patient’s state of health, involvement of peers, and seriousness of the disease’ (p. 52).
Research and theory referring to complex systems are often characterised as complexity science, reflecting the concept of complexity’s wide range of meanings. Complexity can be described as ‘a dynamic and constantly emerging set of processes and objects that not only interact with each other but come to be defined by those interactions’. 33 The NOU2017 uses the term ‘complexity’ to describe both the nature of a (concrete) situation and the (abstract) difficulty of finding solutions to problems. Although the NOU1999 emphasises a quite advanced and abstracted approach to palliative care as it relates to historical and philosophical perspectives, it does not present palliative care as complex. Accordingly, as the 2017 report generally refers to all palliative care–related matters as increasingly complex, we might reasonably expect some explanation of the concept. However, the report does not provide any; instead, the frequent reference takes for granted the word’s familiarity and inherent meaning and, by implication, the reader’s comprehension.
Grant et al. 34 refer to complexity as a relatively new concept in palliative care. Thus, it seems that the NOU2017 was on the frontlines by introducing the concept into palliative care policy. Over recent years, literature on complexity in palliative care has seen extensive growth,35,36 and the word ‘complex’ or ‘complexity’ is used broadly to describe nearly all aspects of specialised palliative care,37,38 epidemiology and patterns of care at the end of life, 39 interactions and communication in clinical practice, 40 decision-making, 41 existential suffering, 42 grief 43 and end-of-life care in dementia. 44 Based on Bronfenbrenner’s ecological systems theory, 45 Pask et al. 46 have developed a conceptual framework to understand complexity in specialist palliative care. The authors claim that complexity goes far beyond the four domains of the holistic approach upon which palliative care usually leans, and rather we ‘. . . need to consider pre-existing and cumulative complexity, the dynamic aspects of complexity, invisible complexity, service-/system-level factors and societal influences to consider and meet patients’ needs comprehensively and effectively’. 46
The significant role of complexity in the NOU2017 and the palliative care literature more broadly reflects its inter-discursive relationship with what is presented as a new paradigm in health care. 47 Modern health care systems are increasingly non-linear and involve multiple networks, including (among others) patients and their peers, health care professionals and leaders from different levels and sectors, including policy developers and decision-makers. Health care strategies require these stakeholders to cooperate, contribute and comply in various ways. Greenhalgh and Papoutsi 48 conclude that ‘it is fashionable to talk of complex interventions, complex systems, complex patients, wicked problems, and the like’. Accordingly, a ‘truth’ is established in the NOU2017 that the totality of topics and relations in palliative care are highly complex, creating a distance and distinction between stakes and stakeholders. Few aspects of palliative care are considered simple or straightforward, and as the NOU2017 is embedded in a biomedical discourse, we argue it thus legitimises a structure in which only those considered to be experts, that is, possessing the highest levels of knowledge and insight (and perhaps also the highest level of education, thus excluding certain demographics), can comprehend and contribute to care. This view seems to be confirmed by Pask et al., 46 who point to the importance of a shared understanding of complexity across different specialist palliative care providers. Foucault’s lens 30 highlights a second paradox here, as these strategies entail the decreased involvement of professionals and institutions, with less use of medical and instrumental care and greater patient accountability, as discussed above.
In summary, we contend that it is appropriate to question the ways in which palliative care strategies serve to produce uneven (objective) structures that assign powerful positions to authorities and professionals while already vulnerable individuals experiencing severe illness and facing death are rendered powerless.
Conclusion
This article identifies how the linguistic features of palliative care policy engender a change in what is expected from patients and in the development of the field. The discourse analysis of the NOU1999 and NOU2017 first revealed the discourse of accountability, which construes the patient in need of palliative care as being empowered and active. In empowering the patients, health care professionals expand their professional gaze 25 to include the patient’s capability to take responsibility for their own health processes. We contend that the NOU2017’s empowering strategies rather lead to ‘certain disempowerment’ 25 by legitimising a partial transfer of responsibility for care from the professionals to the individual. The discourse of complexity further empowers the professionals and institutions that organise services and symptom management, creating a conceptual distance between the individual patient and what is to happen and thus augmenting the asymmetry in power relations between experts and patients.
We argue that the dialogical relationship between the policy discourse around activating patients and managing complex processes seems especially harsh, constructing palliative care in ways that emphasise the responsibility of patients for their prospective wellbeing and health. In line with Borgstrøm and Walter, we argue that ‘choice can become a burden’ 13 by turning the patient’s attention away from existential questions when facing death. 32 We conclude that such consequences of policy development should be considered and counteracted in upcoming policy processes regarding palliative care and are also a matter of further research.