
Abstract
Since 2016, when medical assistance in dying (MAiD) became legal in Canada, healthcare professionals (HCPs) have become familiar with exploring and acting upon patients’ wishes to hasten death (WTHD). In contrast to MAiD, the literature on the voluntary stopping of eating and drinking (VSED) is very limited and there are no standards of practice or legal guidance to support HCPs. In this article, the legal and ethical literature as regards VSED is critically reviewed and new standards of practice are proposed.
Introduction
John R, 65, a retired architect has been diagnosed with metastatic lung cancer. Oncology treatments have failed and he is now receiving palliative care at home. His prognosis is estimated to be less than 3 months. An L5 compression fracture and weakness result in dependence on his wife and adult daughter for Activities of Daily Living (ADLs). Always an active and gregarious man, John is now experiencing profound change and loss. His family physician, Dr S, has ascertained that he does not have a diagnosable mood disorder. John appreciates the comfort and support he receives from palliative care but has expressed repeatedly that he feels ‘done’ and wishes life to be over. After many discussions, it is clear that John and his wife, Susan, will not consider medical assistance in dying (MAiD) due to religious reasons. John asks Dr S, ‘is there anything to help me get out of this mess?’
Voluntary stopping of eating and drinking (VSED) is a considered, voluntary decision to stop eating and drinking because of refractory suffering. The patient intentionally refrains from receiving food and fluids by mouth with the primary intention to relieve suffering by hastening death. VSED, known by many terms in the literature,1–4 is limited to capable decisions to stop oral eating and drinking. It is separate and distinct from: the discontinuation of artificially supplied nutrition and hydration; the natural loss of appetite and thirst associated with ageing or progressive disease; decreased oral intake when feeding is unsafe because of dysphagia; the cessation of eating and drinking due to delusions, paranoia or other mental health reasons (such as anorexia nervosa); or stopping of eating or drinking as a form of political protest.
KEY POINTS
Little is known about the prevalence of VSED.
There is no specific case or statute law in Canada and no professional guidelines for VSED.
Despite broader MAiD criteria in Canada, VSED will remain a viable option for some patients.
More research is necessary before we will know how best to teach and implement VSED.
We propose considerations and a decision making process for HCP-supported VSED.
As in other jurisdictions, when medical assistance in dying (MAiD) became legal in Canada in 2016, healthcare professionals (HCPs) were able to explore and act upon patients’ wishes to hasten death (WTHD). Federal legislation gives Canadians who are suffering intolerably from a serious medical condition the choice of a medically assisted death.
In many jurisdictions, the problem for clinicians is that some patients who are not dying, but have a serious and incurable condition, may request VSED. However, in contrast to MAiD, the literature on VSED is relatively limited and there are no standards or legal guidance to support HCPs.
While VSED at first glance seems less complex than MAiD, it presents its own unique set of ethical challenges. As we illustrate, much of the ethical rationalization for MAiD does not apply neatly to VSED. In 2021, a revision to MAiD was passed 5 to comply with the Quebec Truchon decision, which found that certain limitations on MAiD were unconstitutional. 6 The legal framework revised conditions of acceptability for MAiD; however, the implications for VSED received no attention. The evolution of the legality of MAiD in Canada has led to a two-track approach as a way of protecting patients. Track 1 is for patients for whom death is reasonably foreseeable. Providing all the eligibility criteria for a patient for MAiD are met, there is no necessary minimum waiting (‘reflection’) period. Track 2 is for patients for whom death is not reasonably foreseeable and for these patients an assessment period of at least 90 days is required. 7
We reviewed background material on VSED; identified associated ethical considerations; compared and contrasted VSED and MAiD; and explored the implications of the altered ethical and legal climate as it affects palliative care. The last decade has witnessed a sea change in medical care of the dying and the critically ill, with profound implications for patients and practitioners alike. Openly adopting VSED – discussing it and at times perhaps promoting it – is part of that change in the public expectation of HCPs; VSED is a choice some patients will make and HCPs should be prepared to sensitively explore this option with patients and their families. 8
Background
Very few studies have measured the prevalence of VSED. Chabot and Goedhart 9 ‘computed an annual frequency of 2.1%’ in the Netherlands. Others surveyed HCP or caregiver recollection, encompassing inherent problems with this methodology.10–12 A study of VSED in Switzerland found ‘a big gap between the prevalence of VSED and the knowledge about it’. 12 There is no Canadian prevalence data: (1) most deaths are not reported as such; they are classed by the underlying disease (e.g. cancer); (2) unlike MAiD, there are no provincial or federal reporting regulations or portals; (3) patients may undertake VSED at home without HCP involvement, further limiting what is known about its prevalence; (4) VSED used as a bridge to MAiD is not reported when a MAiD death is reported; and (5) most of the few studies conducted rely on provider recollection. Further research is clearly needed to examine the prevalence and efficacy of VSED not only in Canada but in other jurisdictions and cultures as well.
Despite the absence of empirical material, it is well known that patients seek to end their lives with VSED, either in secret or with the aid of others. MAiD criteria may or may not dissuade some patients from pursuing VSED; some patients will still choose VSED simply because they find it more acceptable. VSED has been pursued both to achieve death (i.e. as an end in itself)13–15 and to cause deterioration that allows the patient to qualify for MAiD (i.e. as a means to an end).14,16
HCPs have had, until recently, little guidance or education in the appropriate use of VSED. No Canadian professional societies provide guidance on VSED (see Figure 1). This leaves clinicians in a practice vacuum or introduces variability in practice, ultimately creating potential justice and equity issues.

Canadian policy search.
The Health Law Institute at Dalhousie University has reviewed Canadian provinces for common or statute law on stopping of eating and drinking.6,17–19 It found that it is legal in all provinces for a capable patient, or a substitute decision-maker (SDM) on behalf of an incapable patient, to stop oral food and fluids.
Important issues remain unresolved. First, whereas a clear legal structure distinguishes MAiD from suicide, no equivalent legal clarity distinguishes VSED from suicide. Accordingly, while a capable patient can refuse food and fluid, it is unclear whether HCPs who support VSED (e.g. through pain and symptom management) are aiding and abetting suicide. Second, considering VSED for incapable patients, case law finds that food and drink are ‘necessaries of life’, not treatments, and that they may not be withheld from an incapable patient who takes them when offered. Finally, it is unclear whether MAiD is permitted for patients who undertake VSED to further deteriorate their condition, thus making their death reasonably foreseeable. 20
The two tracks
Current amendments to the Criminal Code introduce two tracks for MAiD: (Track 1) Natural Death Reasonably Foreseeable (NDRF) and (Track 2) Natural Death Not Reasonably Foreseeable (NDNRF). This change introduces two novel concerns for HCPs in Canada who face requests for VSED and raises difficult questions that must be addressed.
First, as MAiD is now acceptable for people in the NDNRF track, should HCP-supported VSED be similarly viewed? Second, is it appropriate for a clinician to alleviate symptoms for a patient who stops oral intake so as to cause his or her health to deteriorate, allowing the patient to move from the NDNRF to the NDRF track?
VSED in lieu of MAiD
Some cases of VSED begin when a patient in poor health does not qualify for MAiD and wants to deteriorate his or her condition in order to qualify for it. If death is not reasonably foreseeable, VSED would allow a patient in Canada to forgo the 90-day assessment period for Track 2 and relieve suffering more quickly. But these are not the only reasons to prefer VSED over MAiD (Figure 2).8,12

VSED in lieu of MAiD.
As an end in itself, VSED has been used as a last resort. For example, if the patient cannot foresee a desirable future, 21 when applications for MAiD are repeatedly declined, and if the patient’s pain and other symptoms accelerate while awaiting a decision as regards MAiD. In addition, some patients may live in a ‘MAiD desert’ without access to an HCP willing to assess and provide MAiD. For patients like John (see case), VSED may be viewed as a more morally acceptable, ‘natural’ way of dying. 22
Additional reasons in favour of VSED include having greater autonomy, as patients may have more time before they lose decision-making capacity. 23 This means there are chances to interact and bid farewell with friends and family but also more time to reconsider the decision as a whole; a time to reflect, to grieve, and to prepare for death.
Ethical considerations for healthcare providers: MAiD versus VSED
Loss of decision-making capacity
In Canada, only a capable patient may consent to MAiD. In other words, there is no role for an SDM. This provides a safeguard against other individuals authorizing the termination of the patient’s life. The applicability of this principle to VSED is challenging and the considerations here extend beyond Canada.
First, it is not clear to what a VSED patient gives consent. With MAiD, the patient gives consent to a specific, discrete medical intervention that will result in the termination of life. On the contrary, VSED is an autonomous decision made by a competent patient without the need for medical interventions or support to stop eating and drinking; food and drink are not considered by most to be medical treatment.18,24 Although the patient may need medical support if, and when, symptoms occur, 25 an HCP may choose not to provide symptom management on grounds of conscience. The patient may well choose to proceed regardless.
Second, while patients may be capable when initiating VSED, they are expected to lose decision-making capacity after a period of dehydration as ketones and other metabolites increase. 26 Between that loss of capacity and death, it is not clear who provides ongoing consent to medical treatments (i.e. pain and symptom management) that facilitate VSED. Would Susan (see case), as a surrogate, be expected to follow and consent to John’s wish for VSED if, and when, he becomes incapable?
Finally, it is unclear how HCPs should respond to a patient who requested VSED while capable, becomes incapable as a result of dehydration, and now requests oral food and fluid. Providing food and fluid would violate the wishes expressed by the patient while capable; not providing food and fluid would bind patient and HCP in a ‘Ulysses contract’, a controversial concept without legal basis in many jurisdictions. In contrast, MAiD legislation permits a ‘Waiver of Final Consent’ 27 that allows a clinician to administer MAiD to an incapable patient who, before losing capacity, met all MAiD criteria; has a written agreement which permits the administration if incapable; and was informed by the clinician of their risk of losing capacity before the day specified in the agreement. The safeguard is that the patient must ‘not demonstrate – by words, sounds or gestures – refusal to have the substance administered or resistance to its administration’. 28 Should the same provisions apply for VSED? Should a patient be permitted to sign an agreement that allows VSED to continue, irrespective of what the patient says in a delirious or delusional state? In other words, is a Ulysses contract valid for VSED? These concerns surround the ethical rationale for VSED, no matter what the law says and no matter the jurisdiction.
HCP involvement
MAiD requires a specific, discrete action by an HCP that leads to the termination of life. By contrast, the process by which VSED hastens death is entirely patient-driven; the role of the HCP is to provide symptom management, education and counselling.
Current context in Canada
In what follows, we review the main implications of current MAiD legislation for VSED in Canada.5,28 Appendix 1 provides a summary of similarities and differences between MAiD and VSED.
Mental illness
A 2-year sunset clause (until 17 March 2023) excludes mental illness as the sole underlying reason for a MAiD request. In the interim, a Special Joint Committee 29 will review reports developed for parliament by the Council of Canadian Academies, 30 hear from experts and propose legislation. There is no parallel statement or guidance for HCPs who encounter patients seeking VSED with mental illness as the sole underlying reason. However, we think that VSED would not apply to patients with a history of refusing food on account of anorexia nervosa.
HCP involvement under MAiD: conscientious objection/conscientious practice
In Ontario, 638 medical doctors (MDs) and 46 nurse practitioners (NPs) have been involved in MAiD to date. 31 This amounts to 1–2% of all MDs and NPs in the province.
Because NDNRF cases require more complex assessment, fewer assessors and clinicians may be willing to provide MAiD in these cases. Effective referral remains established policy, 32 but potential issues in distributive justice issue loom large if fewer HCPs are willing to provide MAiD to the NDNRF group.
Analogous to MAiD, support for VSED will vary: some HCPs will support VSED regardless of proximity to death, whereas some will limit their support to patients who are NDRF. Given its controversial nature, it is likely that fewer HCPs will support VSED for patients who are NDNRF. Since there are no reporting requirements for VSED, we do not have reliable statistics on how many cases there are or how many clinicians participate. There could be access issues, but we do not know.
If an effective referral is required for clinicians who conscientiously object to MAiD, it is only reasonable to require clinicians who do not want to participate in VSED to make an effective referral. But to whom do you refer? This question will weigh more heavily on MDs and NPs in standalone practice, providers in remote areas and providers in MAiD deserts. Furthermore, is there a role for the ‘Care Coordination Service’ 33 in effective referrals for VSED? The analogy to MAiD is obvious: potential distributive justice issues if access to HCPs is limited. These questions urgently deserve attention and debate.
Proposed guidelines for the HCP presented with VSED
Literature is devoid of guidance for HCP-supported VSED in Canada; while there is no VSED specific legislation, there is also nothing stating it to be illegal. Due to the backdrop of legal ambiguity, we developed the following recommendations to provide structure to practice, with the aim of relieving serious issues in distributive justice and equity. We propose adopting our list of clinical considerations (Table 1). These should drive the evaluations of health care professionals looking after patients at, or close to, life’s closure. In essence, they are based on existing policies and complement MAiD guidelines and standards of practice. Finally, to promote consistency, we propose a patient-oriented decision algorithm (Appendix 2). Recommendations are grounded in the ethical principles of autonomy, justice, nonmaleficence and beneficence.

HCPs, healthcare professionals; SDM, substitute decision-maker; VSED, voluntary stopping of eating and drinking.
Recommendations
We recommend the following:
HCP-supported VSED remains a clinical decision, based on assessment(s) by one clinician.
HCPs provide appropriate supportive and palliative care (emotional support, pain and symptom management) to all patients, including those who have chosen to undergo VSED.
HCPs adopt Appendix 2 to promote consistent practice.
HCPs consult with colleagues when faced with a NDNRF patient who wishes to undergo VSED to hasten deterioration and enter the NDRF track of MAiD.
HCPs ensure that patients, whether or not they are capable, be provided food or fluid if they request it while undertaking VSED. As the dilemma of Ulysses contracts is raised, patients should be informed before VSED that if they request food or fluids, they will be provided.
HCPs ensure that the capable patient provides the initial consent for HCP-Supported VSED. SDM can provide the ongoing consent.
Until the end of the sunset clause – 17 March 2023 – and until we have clarification on mental illness as a sole underlying reason for MAiD, HCP-supported VSED should not be provided to patients whose mental illness is the sole underlying reason for the request.
Conscientious objection must be respected when clinicians abstain from participating in HCP-VSED.
HCP who conscientiously objects should be required to make an effective referral as per the rules of their respective province.
Conclusion
VSED is a compelling issue in palliative care. As literature and guidance on VSED are limited, we present a novel set of recommendations, criteria and a decision-making model to mitigate potential distributive and equity concerns. Although Canada has recently expanded the boundaries of MAiD, considerations over VSED are relevant to jurisdictions that may not have yet legalized MAiD. It could be argued that another ethical burden has been placed on HCPs; it may also mean we have more work to do in understanding and optimally supporting our patients at the close of life.
Dr S felt it would be in John’s best interest to offer VSED as an option in end-of-life care. After an initial discussion, John revealed that he had heard of VSED but was reluctant to raise it with his family and his doctors; he was concerned they would see him as giving up. After a period of reflection and discussion with his wife, John opted to pursue VSED. As he was uncertain of his resolve, and also worried about how he might feel, John did not suddenly stop his oral intake. He initially requested water and small amounts of Ensure. His interest in any form of sustenance rapidly declined. John was provided with immaculate oral care and died peacefully at home eight days later with his family at his side.
Footnotes
Appendix
MAiD–VSED comparison.
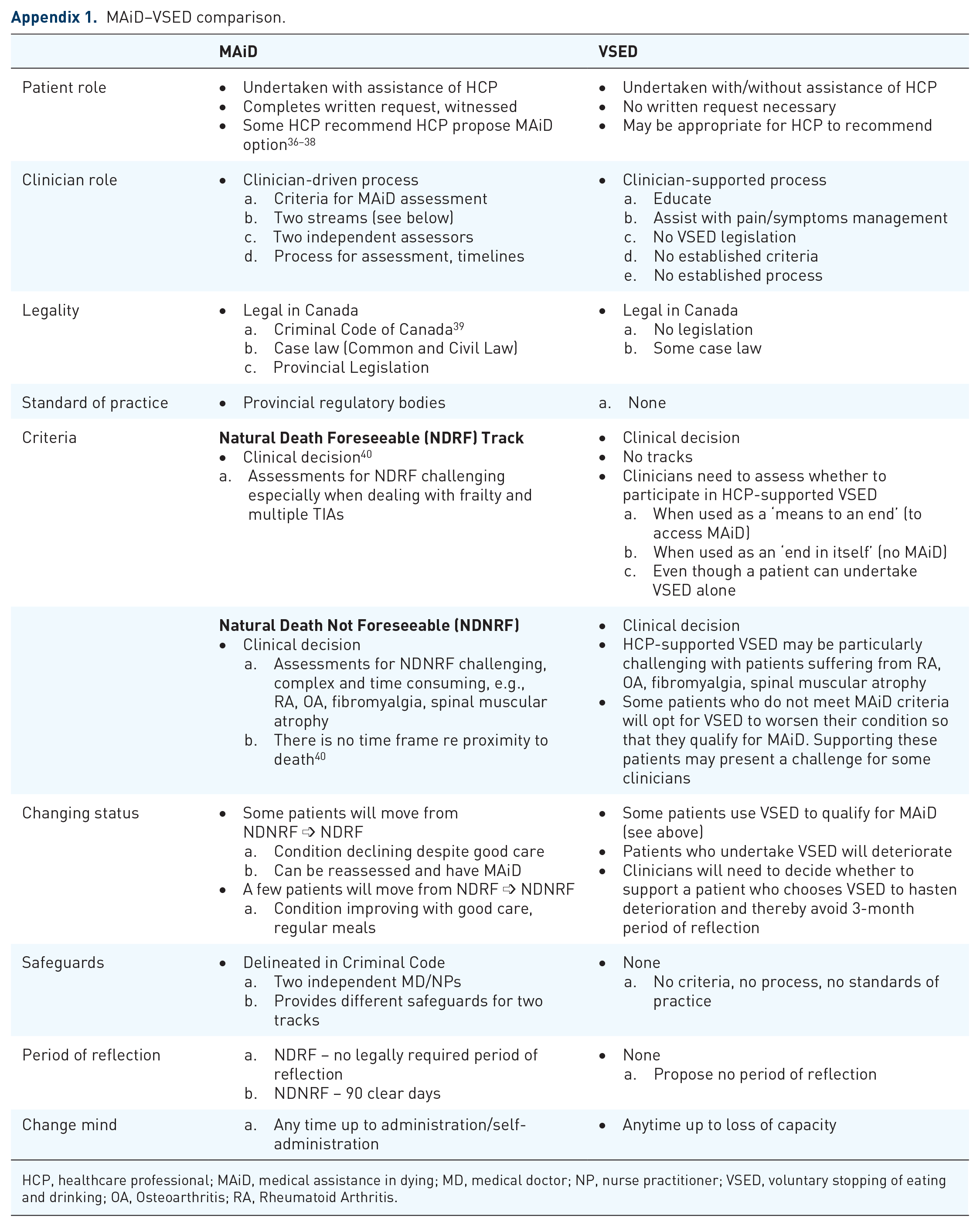
| MAiD | VSED | |
|---|---|---|
| Patient role | • Undertaken with assistance of HCP • Completes written request, witnessed • Some HCP recommend HCP propose MAiD option36–38 |
• Undertaken with/without assistance of HCP • No written request necessary • May be appropriate for HCP to recommend |
| Clinician role | • Clinician-driven process a. Criteria for MAiD assessment b. Two streams (see below) c. Two independent assessors d. Process for assessment, timelines |
• Clinician-supported process a. Educate b. Assist with pain/symptoms management c. No VSED legislation d. No established criteria e. No established process |
| Legality | • Legal in Canada a. Criminal Code of Canada 39 b. Case law (Common and Civil Law) c. Provincial Legislation |
• Legal in Canada a. No legislation b. Some case law |
| Standard of practice | • Provincial regulatory bodies | a. None |
| Criteria | • Clinical decision 40 a. Assessments for NDRF challenging especially when dealing with frailty and multiple TIAs |
• Clinical decision • No tracks • Clinicians need to assess whether to participate in HCP-supported VSED a. When used as a ‘means to an end’ (to access MAiD) b. When used as an ‘end in itself’ (no MAiD) c. Even though a patient can undertake VSED alone |
| • Clinical decision |
||
| Changing status | • Some patients will move from NDNRF ➩ NDRF |
• Some patients use VSED to qualify for MAiD (see above) |
| Safeguards | • Delineated in Criminal Code |
• None |
| Period of reflection | a. NDRF – no legally required period of reflection |
• None |
| Change mind | a. Any time up to administration/self-administration | • Anytime up to loss of capacity |
HCP, healthcare professional; MAiD, medical assistance in dying; MD, medical doctor; NP, nurse practitioner; VSED, voluntary stopping of eating and drinking; OA, Osteoarthritis; RA, Rheumatoid Arthritis.
Acknowledgements
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.