
Abstract
Voluntary stopping of eating and drinking (VSED) is a well-known phenomenon among palliative care professionals. This study intent to distinguish between different forms of VSED. In a qualitative interview study 18 relatives were interviewed about their experiences of caring a person during VSED. Different forms of oral nutrition refusal and different forms of VSED were found and described. The study results help members of the multidisciplinary team to manage the situation appropriately.
Background
The intake of food and liquid is a highly social phenomenon.1,2 Therefore, it is not surprising that giving up food and liquids poses a great challenge to relatives and health professionals.3–8 The reasons for refusing nutrition can be very different. Mental diseases such as depression, advanced dementia, anorexia or cachexia can cause people to stop intake.5,9–11 Another reason for refusing nutrition may be eating disorders caused by physical impairments, such as pain in the mouth or difficulty swallowing.8,12–14 Besides psychological and physical causes, the refusal to eat (and drink) is also recorded in the context of a natural dying process. Often people who are dying tend to lack appetite and are too weak to eat.7,15,16 Another form of nutrition refusal is the politically motivated hunger strike to draw attention to grievances and to call on politicians and decision-makers to improve or change the current situation.17,18 In the cases listed, refusal to eat and drink can be considered a symptom of the underlying disease or motivation. It is not intended to take life prematurely, even if this is possible because of refusal. Besides these forms, another form of nutrition refusal exists, which differs significantly from the previous forms. It is about the voluntary stopping of eating and drinking (VSED). As the name implies, VSED occurs when a person deliberately stops eating and drinking, intending to end their own life prematurely. The course of VSED is marked in such a way that the person who is willing to die and is still able to eat and drink refrains from doing so voluntarily and self-determined.19–21 The decision to VSED is often based not only on somatic diseases or cancer but also on loneliness, social isolation or increasing dependence.19,22
In any case, professional care and support of the persons concerned are necessary. While mental illnesses and eating disorders can often be treated by medical and nursing measures, in the case of natural death, the intention is to accompany the dying. In the case of a hunger strike, a political agreement must be reached. As soon as the hunger strike is over, medical and nursing support is needed to strengthen the weakened body. The task of health professionals is to inform the person concerned and their relatives about the course of VSED. Furthermore, to check judgement of the person willing to die, to plan the course of accompaniment and finally to accompany the person willing to die and their relatives during VSED.23–25
Current research results explicitly indicate insufficient knowledge on VSED. 21 A distinction to different forms of VSED has not yet been published, and there is currently no clear distinction to other forms of nutrition refusal. Through preliminary data analysis of interviews with relatives who accompanied a loved one during VSED, it was possible to create a model of what different forms of nutrition refusal and VSED exist and which attributes distinguish them.
Aim of the study
This study aimed to identify and distinguish between different forms of oral nutrition refusal and different forms of VSED, and also to show a further awareness of different forms of nutrition refusal.
Methods
Study design
This qualitative interview study is a report on the second objective of open-ended semi-structured narrative interviews 26 conducted between February 2017 and Summer 2018, which examined the accompaniment of a loved one during VSED. While the study’s main objective is to identify the similarities and differences using a multiple case study, the second objective is to verify that the VSED criteria are met in those cases. An inductive–deductive thematic analysis was conducted,27,28 followed by an in-depth analysis based on the principles of grounded theory. 29
Recruitment
In this context, we surveyed healthcare professionals regarding the frequency and prevalence of VSED, and their experiences of and attitudes towards it. 30 Following media interest through newspapers31,32 and television, 33 we received requests from people who wanted to share their experiences of having a relative with VSED. These formed the basis for a case series that explored people’s experiences of supporting their relatives during VSED.
Data collection
After the relatives contacted us and agreed to participate in this study, we made an appointment for an interview. Interviews were conducted in a sheltered environment at university, by telephone or at a location of their choice (e.g. café). The authors (S.S. and A.F.) conducted open, semi-structured interviews. During the data collection, the interview guideline was developed iteratively. Through a narrative input question, the participants were given the impulse to describe the full course of the VSED, including the reasons for implementing VSED, the decision-making process with relatives and health professionals, and the course, duration and possible complications during VSED. The interviews, lasting 1 hour and 15 minutes on average, were digitally recorded and transcribed verbatim by one author (S.S.) and external service.
Data analyses
Transcripts were imported into MAXQDA 18 and processed using the inductive–deductive thematic analysis approach. It is an iterative process of coding to identify the patterns between the concepts.27,28 Two people (S.S. and A.F.), with experience in VSED and qualitative research methods, reviewed and coded the transcripts. We developed a series of codes from repeating themes and co-coded them until we had a consensus. An axial coding with inductive and deductive techniques was also used. 29 The initial descriptive element within the case analysis allowed us to identify deviant cases that contradict to VSED. 26 These provide a substantial basis for a better understanding and description of VSED.
Ethical approval
The responsible and independent ethics committee of the Greater Region of Eastern Switzerland approved this study (EKOS 17/083), and the participants signed an informed consent form before the interview. Thus, no personally identifiable information was collected. Participation was voluntary, and participants had irreversible anonymity. The participants also sought contact with the researchers themselves. There were no disadvantages in refusing to participate in the interviews. Participants were informed in detail of the aim and purpose of the study, as well as the use of generated data and their rights. This ethical approach is based on the principles of the ‘Declaration of Helsinki’ and ‘informed consent’. Anonymity and respect for human dignity were guaranteed at all times during the research process. Drawing conclusions about the respondents will not be possible at any time. 34
Results
Description of the participants
A total of 15 women and 3 men signed up to share their experiences of caring for a relative during VSED. While most interviews were held with one person, two interviews were held with a couple. The case series includes nine women and four men aged between 27 and 93 years.
A model of different forms of oral nutrition refusal and different forms of VSED
The analysis of the case descriptions clearly showed that other unknown forms exist besides the classical form of VSED as an explicit wish to die. For a better overview of the different forms of oral nutrition refusal, see Figure 1. The x-axis defines the reason for not eating, which can be traced to the left either as a symptom of an underlying disease/motivation or to the right as a conscious decision by a person willing to die. On the y-axis, it is a question of whether the nutrition renunciation is known to others. While in the upper half the reasons for the refusal to eat are known, in the lower half it is not known to others.
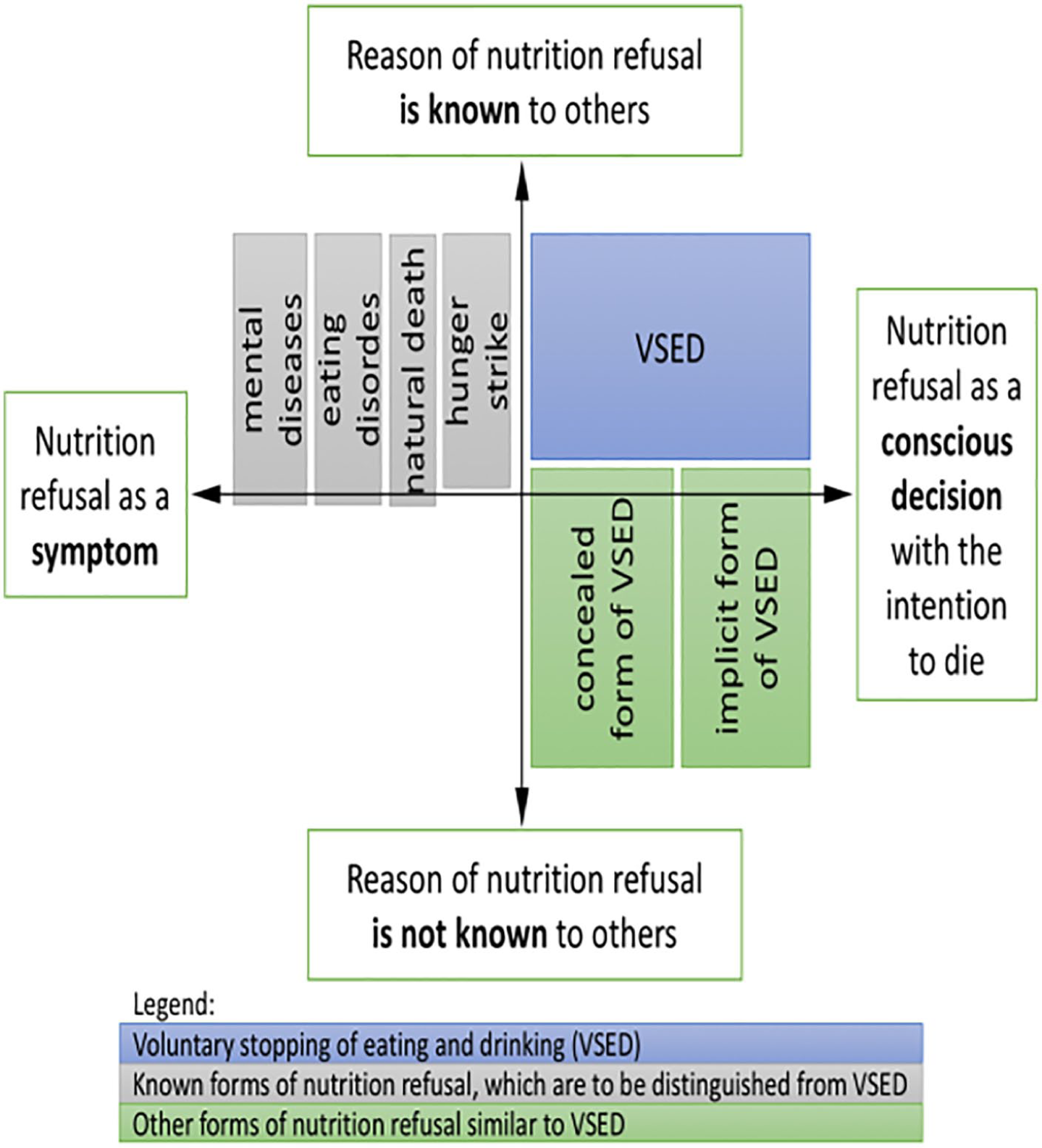
Different forms of oral nutrition refusal and different forms of VSED.
The fields highlighted in grey are various forms of nutrition refusal known from the literature. Three of the four forms slightly exceed the y-axis in the graph, as the reasons for the nutrition refusal may not always be known from the beginning. The hunger strike, on the contrary, is immediately communicated as such. The different forms of VSED will now be explained using case descriptions.
Voluntary stopping of eating and drinking
Case history – Voluntary stopping of eating and drinking A boy was born with the disease Arthrogryposis multiplex congenita and was therefore physically severely restricted. In the course of his development, he was dependent on a wheelchair. The adolescent accepted his illness and quickly learned to take care of his therapy. At the age of 13, he suffered from severe pneumonia, was admitted to hospital as an emergency, was in a coma and had to be resuscitated. His left lung had collapsed. Since then, the adolescent has been terrified of suffocating. Knowing that the disease reduced his life expectancy, the boy never let himself be discouraged, completed education, and was a life-affirming person. At the age of 27, the young man’s condition deteriorated significantly, and the fear of suffocation increased. The concern was so great that the young man decided to end his life before the disease progressed. At first, he was informed about the assisted suicide that would have been granted to him in Switzerland but felt that this path was unsuitable and inappropriate. Finally, he discovered the VSED option during his research on the Internet and decided to follow this path himself. He informed his family and his doctor and said goodbye to everyone with written texts and in a personal conversation. He consistently stopped eating and drinking, refused sedation, and went out of life in full consciousness. The young man died after ten days in the sheltered domestic environment and cared for by his parents.
The case report shows that the decision to VSED is taken independently and voluntarily by a person capable of making a judgement to end life prematurely. Besides, it becomes clear that others are included in the decision-making process and in accompaniment, that is, this path is known and supported by all others.
The concealed form of VSED
Case history – The concealed form of VSED A 47-year-old woman had recurrent breast cancer and metastases in her liver and brain. When the pressure from suffering became unbearable, this deeply religious, Catholic woman decided to forego nutrition and fluid to hasten her death. She communicated her desire openly. However, her social environment – also deeply religious – denied this self-sufficient woman this desire in a patronising manner, as her decision was deemed incompatible with religiosity. Also, adequate pain treatment was forbidden by her husband. Palliative care professionals were subjected to pressure from relatives and did not listen to the vulnerable woman’s wishes. They denied her decision-making ability, and she received artificial food but still drank independently. To put an end to her suffering, she secretly decided to refrain from consuming fluids. The time to death lasted six weeks.
This is a previously unknown form of VSED, and we suspect that it is infrequent. One of the female patient’s dedicated nieces were able to tell us about this case. What looked like suicide to the relatives was a consistent and natural decision for the woman in question. Since she had to act in secret, adequate professional care was not ensured.
The unspoken or implicit form of nutrition refusal
Case history – The unspoken or implicit form of nutrition refusal A woman had become a widow at the age of 77. She was independent and educated, had a strong personality, and still drove a car till the age of 91. After a few falls at home, however, she was transferred directly to a nursing home after a hospital stay, since she could no longer care for herself on her own. She was dependent on nursing aid for mobilisation, and deafness severely restricted her communication. She felt socially and emotionally isolated, meaning that she had nobody with whom she could share her feelings and needs. She mentioned being ‘full of days’. Without it being noticed by the nurses, she dispensed with both food and fluids. Within three to four weeks, the woman died. Until her death, the staff did not recognise that she had chosen to stop eating and drinking – only her daughter was aware that she made this by choice.
A rather unknown form of VSED is the ambiguously communicated, often silent, reduction in food and fluid intake. In our investigations, this is usually found in old age or the transition phase to the last stage of life. Individuals may decide to stop eating and drinking without explicitly expressing their decision, and they also do not hide their intention. It is common because they follow this path for themselves but do not want to or cannot communicate their decision. This variant is less the expression of a personal desire for autonomy and self-expression but can be understood in the context of life fatigue.
Discussion
This study aimed to distinguish between different forms of oral nutrition refusal and different forms of VSED. The decisive difference between nutrition refusal and VSED is that the refusal of oral nutrition is an expression of a disease or motivation and VSED is an explicit desire to die. Furthermore, it could be shown that other forms exist besides VSED. They differ in particular in the fact that the desire to die or the reason for the refusal to eat and drink is not explicitly communicated. The concealed and the implicit VSED are similar in the sense that the underlying desire to die is not known to most others. Therefore, no investigations, for example, regarding the ability to judge, are undertaken. What these two forms differ in is that the person willing to die actively tries to deceive others in the concealed VSED, while no attempts are made to disguise himself in the implicit VSED.
Important in the implicit VSED is the fact that the health care professionals involved can misjudge the situation. What is an active act by the person who is willing to die can be interpreted by the nurses as a dying process. Regarding the implicit VSED, would establish that there is a risk that professionals will generalize and label the behaviour of patients. There is a possibility that the situation may be misjudged. And people are accompanied in their deaths, although they could have been helped to live on with appropriate therapies. Occasionally, there is a lack of attention or no discussion of the reason why a person does not eat. However, this is not reflected, which is a problem. In the context of video analyses of the nutrition intake of people with dementia in the final stage of the disease, we found that experts managed food and fluid administration differently, depending on the following:
The continuing education and training of nurses;
An understanding of influential factors and underlying conditions;
Body stresses experienced by those affected, which prevent nutrition intake.
It seems that people with a reduced life prognosis, or with life fatigue, who do not want to or cannot die through physician-assisted suicide, tend to choose VSED. It is, therefore, necessary that healthcare institutions and professionals address this issue and discuss how to manage the phenomenon in the future. The differentiation of other forms of nutrition refusal and different forms of VSED described above allows those involved to avoid misinterpretations and allows healthcare professionals to evaluate the overall situation. As illustrated by cases mentioned above, VSED is selected by individuals who may be young or old and who may have an underlying illness or even be healthy. In addition to the lack of intake of food and fluids, other factors – which influence the ethical and moral judgement of the situation – such as the patient’s and relatives’ culture and religion need to be considered when managing VSED. We argue that those choosing VSED should, therefore, not be regarded as a homogeneous group. Instead, each person concerned should be managed holistically, based on the biopsychosocial model. 35
The influence of the relatives
When looking at the different forms of nutrition refusal, it becomes clear that relatives play an essential role in dealing with the condition. Our investigations show that relatives try to influence the decision of the person concerned and, thus, play an important role in the implementation of nutrition refusal. The available literature indicates that relatives fall into one of three groups concerning their attitude on the refusal of nutrition intake at the end of life: ‘agreement’, ‘fluctuating opinion’ and ‘disapproval’. Despite understanding the personal situation, the relatives wonder whether they could have done something to counter the decision. 2 It is therefore important for professionals to engage with relatives and provide information on the different forms close to VSED. 15
Treating VSED professionally
This article presents for the first time other forms of nutrition refusal and other forms of VSED. This differentiation indicates that it is no longer appropriate to consider nutrition refusal as a single phenomenon. To deal professionally with the decision of those concerned, it is crucial first to develop clear definitions of the specific forms. It is also important to raise specialists’ awareness of the explicit and, in particular, even the implicit and concealed form of VSED.
Footnotes
Implications for practice
VSED involves the autonomous and voluntary stopping of food and fluid intake by the person concerned, with the intention of prematurely ending their own life.
VSED should be considered as a multifaceted condition that must be distinguished from other forms of nutrition refusal and other forms of VSED. In particular, the implicit and concealed VSED should become known as forms in order to avoid confusion with the natural dying process.
Different forms of nutrition refusal close to VSED are associated with different needs, and professional support must be adapted accordingly.
Author Contributions
AF was project leader and decided on the design of the study, SS and AF collected and analyzed the data, WS was consulted for expert opinions, SS wrote the first draft, AF and WS revised the first draft, SS developed the graphic.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.