
Abstract
Aims:
The study aimed to explore the quality and impact of care provided through an innovative palliative care project to improve the quality of life of older people in an urban informal settlement in Bangladesh.
Methods:
Center for Palliative Care (CPC) at Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, in collaboration with the Worldwide Hospice Palliative Care Alliance (WHPCA) has been operating this community project since 2015. A cross-sectional observational design was used in this program evaluation study. A total of 594 people received services including 227 patients (Group-1) receiving regular and intensive palliative care and 367 patients with less intense needs (Group-2) receiving relatively less support based on need. In addition, current group-1 patients (total 114) and a matched cohort of 58 group-2 patients were interviewed with an experience of care survey questionnaire. Baseline and demographic data were presented in tables. The Z-test was used to measure mean statistical differences between two groups.
Results:
Multiple comorbidities were common. Pain was the most frequently noted physical symptom along with anxiety, sadness, and depression as common psychological concerns. Compassionate palliative care for the older people had significant (p < 0.05) impact on psycho-social and spiritual care, caregiver training, responding to emergencies, and reduction of out of pocket healthcare expenditure among the intensive intervention group.
Conclusion:
Using a community-based approach following this model may play a significant part in expansion of palliative care throughout Bangladesh to meet the huge need and scarcity of such services.
Introduction
In Bangladesh, a country of South Asia with more than 166 million people, the Government has adopted a target of reducing poverty to 14% and entering middle-income country status by 2021 as part of the Vision 2021 plan and the associated Perspective Plan 2010–2021.1,2 More than 30% of south Asian people live in informal settlements (generally known as slums) analogous with the world scenario. 3 About 14,000 tenement housings were counted housing 2.2 million slum dwellers (6.33% of the urban population) in 2014 in Bangladesh; only 24.35% of these settlements were recognized in Dhaka city corporations. 4
Although receiving greater attention recently, the health of neglected impoverished populations such as those observed in Bangladesh has always lagged behind general healthcare policy. 5 These highly populated urban residential areas were found to have worse health outcomes than rural areas in countries as varied as Kenya, Egypt, and India. 6
Every year, over 85% of ‘premature’ deaths occur in low- and middle-income countries due to non-communicable diseases (NCDs), also known as chronic diseases. 7 A high prevalence of NCD risk factors was documented in the slum population in Bangladesh in a recent survey 8 consistent with the finding of increasing deaths due to NCDs. 9 In the WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020, palliative care is unambiguously recognized as part of the comprehensive service and management for NCDs. 10
The World Health Assembly recommended that countries integrate palliative care services into national health policy. 11 In spite of over 600,000 incurable patients in need of palliative care every year in Bangladesh,12,13 it is very difficult to encourage policy-makers to focus on palliative care rather than curative care in an underprivileged socioeconomic country where primary care is rarely available and quality-of-life issues are rarely practiced. But a civilized society cannot overlook the significance of palliative care as a means to reduce the suffering of dying patients each year. 14
Korail is one of the largest informal settlements in Bangladesh, established around 1985 with approximately 2.5 million inhabitants. 15 ‘Compassionate Korail’, a community-based palliative care project conducted by the Center for Palliative Care (CPC) of Bangabandhu Sheikh Mujib Medical University (BSMMU) Dhaka, in collaboration with the Worldwide Hospice Palliative Care Alliance (WHPCA) has been supporting its extremely poor population with practically no primary health care facilities since 2015. It began as a 1-year pilot and continued as regular project for two more years. The aim of the project was to evolve a community-based sustainable model of palliative care for older people with serious illness, frailty, and unmet care needs in Korail through a compassionate community approach. As the project addressed important local needs in terms of health and humanity and had national and global impact, funding was extended through December 2020. It should be noted that the population for this program was broader than the traditional palliative care population in line with the compassionate community philosophy.
Basic community health workers trained as palliative care assistants (PCAs) were the primary providers of care to patients and families served in this program. They were supervised and supported by medical doctors, nurses, and physiotherapists who made regular visits. Regular weekly outpatient clinics, monthly eye camps, and gynecology outpatient services were also added to strengthen primary health care services in the community and to gain trust among residents. Training programs and meetings with volunteers, including weekly courtyard meetings with the community residents were conducted to promote local participation. After the training volunteers they went to patients’ residences with PCAs to provide additional help. This included assistance distributing the food pack, referring the people in need to the program, spreading news about services among local people, collecting donations for the program’s charity box, encouraging others to volunteering and so forth.
Awareness programs in different parts of Korail included meetings with community-based organizations, leaflet and poster distribution, collaboration and coordination with other NGOs, weekly charity shop and donation collection, photo exhibition, and celebrating World Hospice and Palliative Care Day every year were aimed at mobilizing the community and enhancing the sustainability of the project. The project attempted to engage local support both within and beyond the boundaries of Korail and continued to attract interest and visits for fund raising and publicity.
The evolving concept of ‘Compassionate Community’ is based on the motivation of communities to take more responsibility in their own healthcare and to provide care at the end of life.16,17 This model of community-based palliative care in Korail may play a potential role in development of palliative care for chronic diseases throughout Bangladesh in the future. An overall evaluation of the services provided in community and home settings by the healthcare providers will help determine ways in which this model can be improved.
Methods
Study design
A cross-sectional observational design was used in this program evaluation study.
Aim of the study
To explore the views of service users with regard to the quality and impact of care provided by the community palliative care team in Korail.
Study setting
‘Compassionate Korail’, community-based palliative care project in Korail.
Study population
The patients in this study were all residents of the Korail indigent community in Dhaka, Bangladesh, who had evidence of some degree of life-limiting conditions, for example, cardiac, respiratory, or neurological diseases; cancer; and so on. Study subjects were divided into two groups depending on an assessment of their needs. Those with more intense needs, bedridden and incapacitated were assigned to Group 1 to receive palliative care along with food and medicine support. Some were isolated/abandoned by the family or in serious financial crisis. While those with less-intense needs, mobile, able to walk to the hub were assigned to Group 2 and received primary outpatient care.
Inclusion/exclusion criteria
Inclusion: To be eligible to avail this service, the study subjects needed to be suffering from any life-limiting or chronic illness along with at least one of the following criteria:
Bedridden and ill people of any age.
Incapacitated but may not be bedridden.
Older people without any income.
Isolated/lonely people.
Exclusion: No children under the age of 18 are included.
Data source and instrument
Baseline and demographic data were collected from patient information sheets completed during enrollment into the project. A separate analysis of data regarding service quality and impact was collected through structured questionnaires. The focus was mainly on whether pain and other concerns were adequately addressed or not, response of the team to their emergency needs, reduction of out-of-pocket expenditure, recommending service to others, overall service rating and interest in volunteering. An interviewer was trained on the questionnaire and study objectives before data were collected. The interviewer read the questions aloud, helped patients to understand them, and transcribed the patient’s answers.
IRB approval
The institutional review board of Bangabandhu Sheikh Mujib Medical University approved the protocol (No. BSMMU/2018/480, Date: 14.01.2018) before study commencement. Participants were informed of the study purpose, risks, and benefits and invited to voluntarily participate in the study. All participants signed an informed consent form before participation.
Data confidentiality and protection
Participants were identified by a numerical study ID assigned at recruitment in the order participants were recruited. The master list linking patient name and ID numbers was kept in a password-protected database separate from all study data. Personal Health Information was not released externally and was stored securely at all times. Mobile devices (e.g. laptops, USB keys) that contain study information was also stored securely. Patient data were all de-identified for analysis. Electronic files stored on mobile devices was password-protected and encrypted. Only research team members had access to the patient’s data.
Data analysis
All data were checked, verified for consistency, and edited for finalized result. Data were entered directly into the computer by using SPSS software (version: 21.0). The descriptive statistics for the whole population are presented in tables with means and percentages.
Separately analysis was conducted to look at the two subgroups in the population of patients depending on the level of interventions they received. One group received palliative care and the second group only primary care. All patients in Group 1 who were still enrolled were interviewed at the end of the project to evaluate the services they received. A random selection of patients in Group 2 was also interviewed as a comparison group.
The statistical Z-test was used to examine the probability that the mean scores of the two groups were or were not significantly different statistically. This approach is used with sample sizes that are reasonably large and where raw data are believed to be normally distributed. All data were rechecked to avoid data entry error and ensure analysis using appropriate statistics.
Results
A total of 594 elderly people suffering with various life-limiting conditions were supported through December 2019. Among them, 227 patients with intense palliative care need belonged to Group 1 and 367 patients who received only general primary outpatient care to Group 2. Group 1 patients received services from the physician, nurse, and physiotherapist on the basis of need, and PCAs provided follow-up visits on a regular basis (goal: minimum 2 days/week per patient). They were also provided with social supports including essential palliative medicines (EPM), monthly food package, commode chair, blanket, and dressing materials as needed.
Group-2 patients had comparatively better physical condition than Group 1. They attended general outpatient care only and some of them received prescribed essential medicines within a limited budget but none availed the monthly food package or palliative care. A group of dedicated volunteers from Korail community provided follow-up to our enrolled patients. As of March 2020, 318 (114 in Group 1 and 204 in Group 2) of these patients were receiving active care.
Baseline data with demographic characteristics were collected from all 227 patients with intense palliative care needs who received support from the beginning of the project and 367 Group-2 patients who received only general primary outpatient care (Table 1). All current Group-1 patients (total 114) and 58 of Group-2 patients gave written consent and volunteered to participate in a follow-up study by in-person interview with a survey questionnaire evaluating their care experience.
Demographics of the Group-1 (N = 227) and Group-2 (N = 367) patient population.
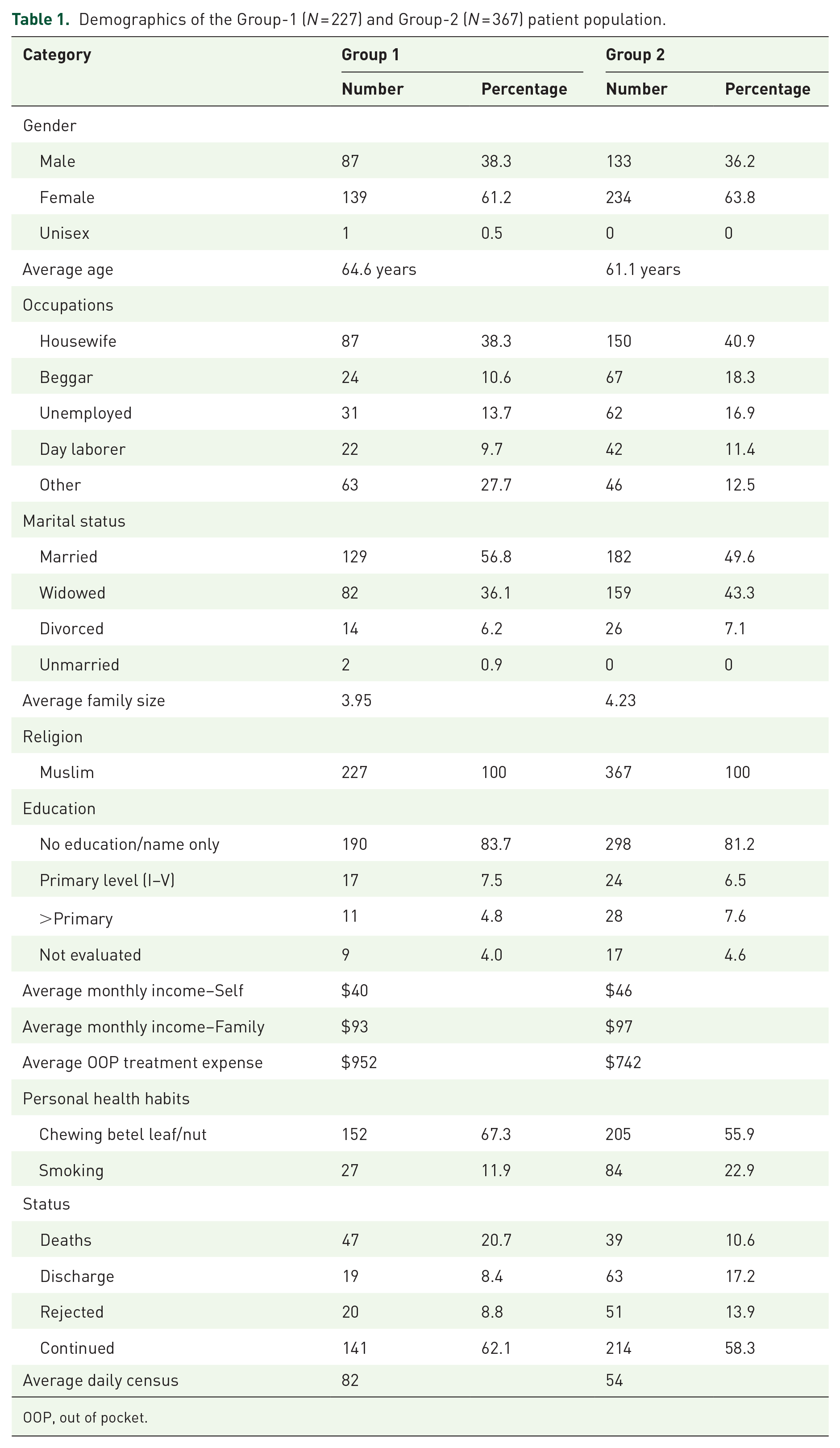
OOP, out of pocket.
Of the Group-1 patients, females were predominant among the service recipients, and most of them were married housewives with limited or no education. Among the total of 227 patients, 21% died during the project, and 19.1% of patients either rejected the service (9.8%) or discontinued (9.3%) for various reasons including; migration to home place of origin, or other places or they requested to discontinue services. Average monthly income was $40 and $93 for the patient individually and family, respectively. Average out-of-pocket expenditure for treatment before enrollment into the project was $952 (Table 1).
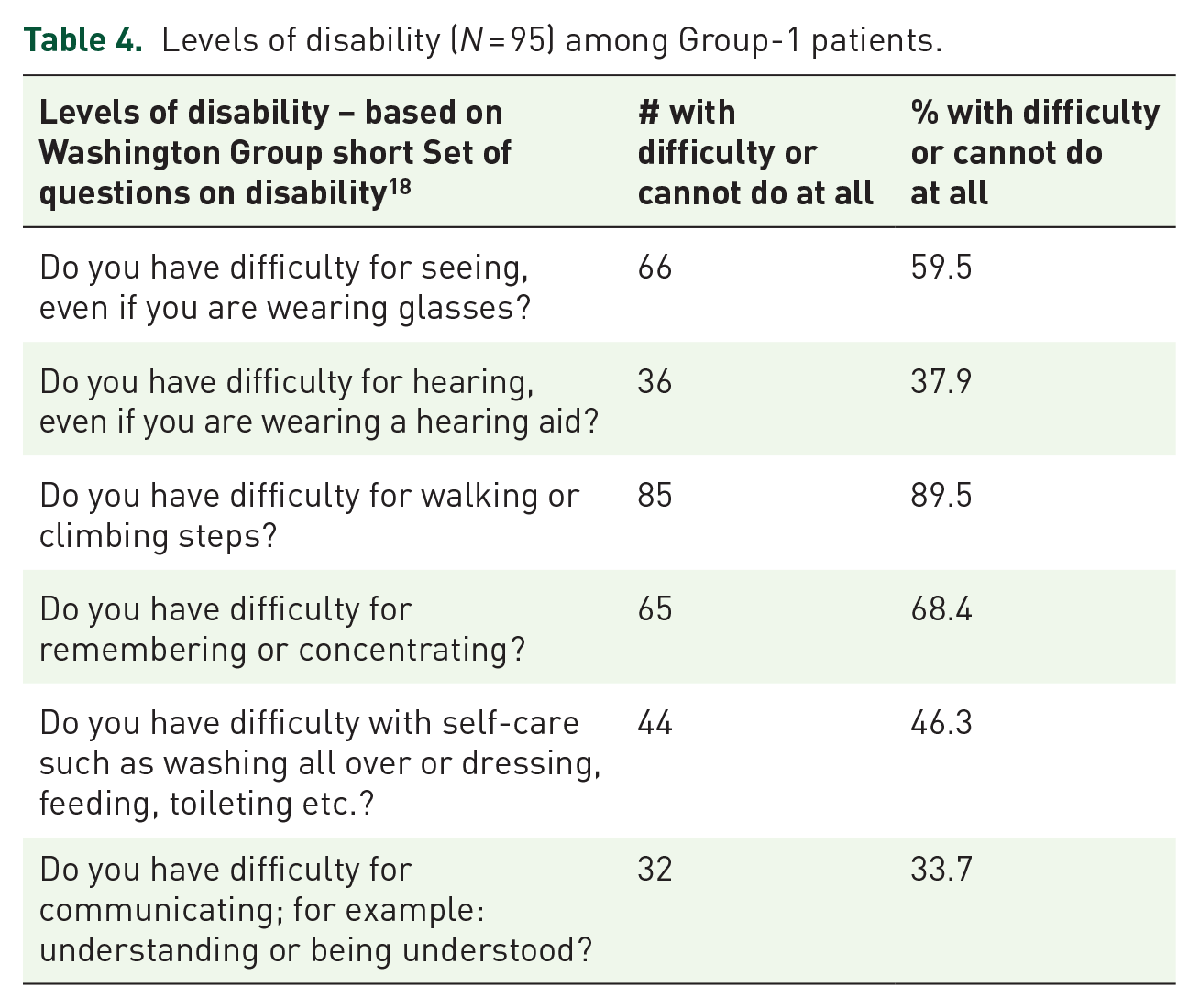
Many of the patients had multiple comorbidities; hypertension, stroke, cerebrovascular diseases, and chronic obstructive pulmonary disease (COPD) were most common. Only 8.8% patients were suffering from malignancy (Table 2). Pain was found to be one of the most documented symptoms among the patients followed by weakness, constipation, insomnia, anorexia, and others. The majority (61.8%) of the patients were ambulatory and able to carry out daily activities (ECOG-1) and only 4.5% were completely bedbound (ECOG-4) (Table 3). However, many of them were physically disabled, such as having ambulatory impairment (89.5%), cognitive impairment (68.4%), and vision impairment (59.5%) (Table 4).
Diagnoses (Multiple) among the Group-1 (N = 227) and Group-2 (N = 367) patient population.

COPD, chronic obstructive pulmonary disease; IHD, ischaemic heart disease.
Most common prevalent physical symptoms among Group-1 patients.
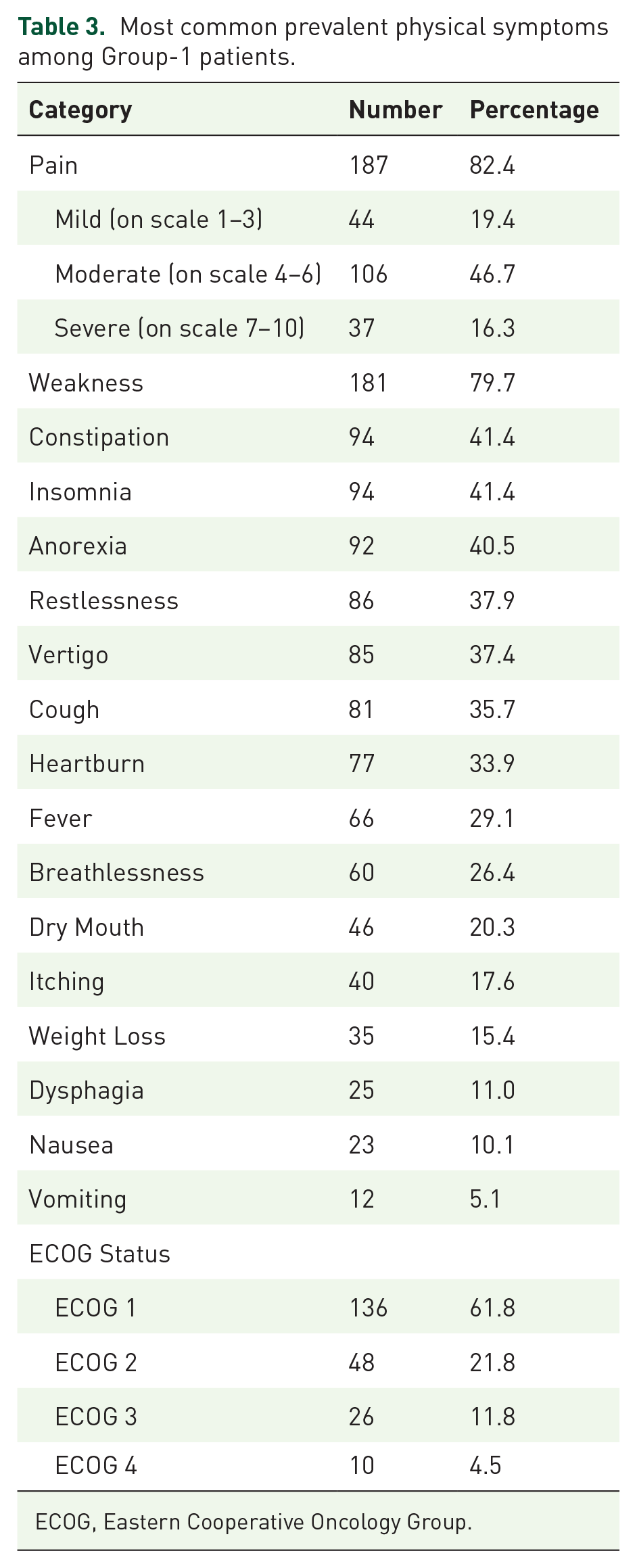
ECOG, Eastern Cooperative Oncology Group.
Levels of disability (N = 95) among Group-1 patients.
Anxiety, sadness, and depression were commonly observed and documented psychological concerns of patients based on interviews. Worries about the family members and lack of income were the cause of significant social distress whereas loneliness contributed to most spiritual concerns. Around 78% patients were counseled regarding their disease prognosis; and most had this revealed to them by doctors (Table 5).
Psychosocial and spiritual concerns among patients with intense palliative care needs.

Evaluation of the care by the patients showed significantly better outcomes statistically in psycho-social and spiritual care, caregiver training, responding to emergencies, reduction of out-of-pocket expenses (OOPE) for health care, and overall rating of care among the intensive intervention group (Group 1) compared to the Group 2 (Table 6).
Comparison of patient evaluations of care based on levels of intervention (Z-test done. *p < 0.05 significant).
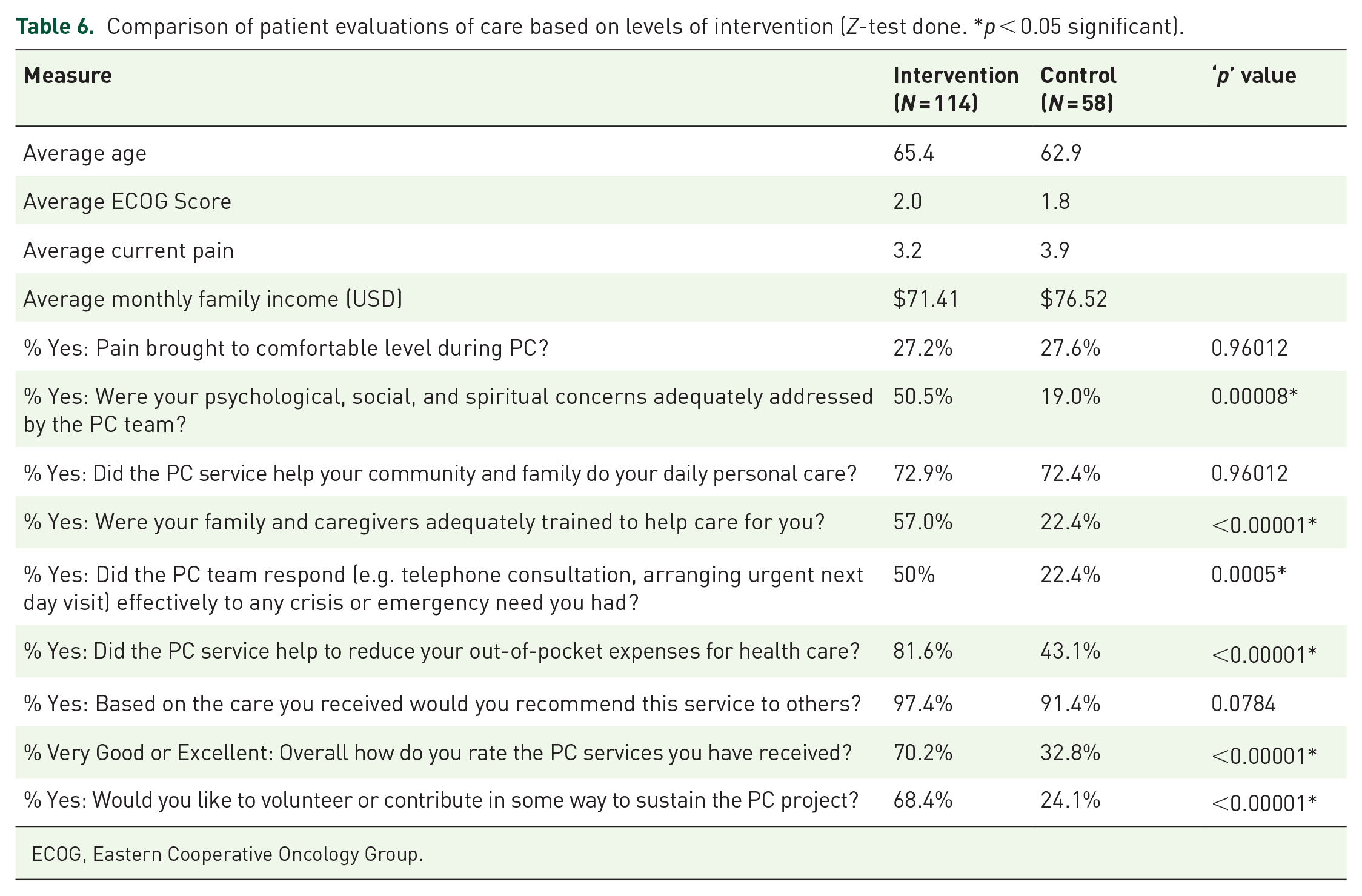
ECOG, Eastern Cooperative Oncology Group.
Discussion
At the outset of the study, it was apparent that the people of the community did not have access to even basic primary health care and that specialized medical services like palliative care were a luxury for them. The Korail community was concerned about and had a history of NGOs entering their lives and then leaving, either bringing very little actual support or leaving rapidly without any enduring beneficial impact. With involvement and support from the local community along with flexibility to change and adapt, a good relationship was built and trust was gained over time. The aim was to increase access to compassionate health care and support in Korail for those with serious illness, frailty, and unmet care needs. So, family and neighbors were encouraged to become involved in the care of their own community members (in particular, the elderly). This approach was relevant for Korail as it built on cultural norms in the community of caring for one another.
In the impecunious and poverty-stricken area of a developing country like Bangladesh, women and girls remain neglected and uncared for by the family as well as by the society. This likely explains the predominance of female enrollees. As the project was specially aimed at the elderly, mean age was 64.6 years similar to the population of home-based palliative care patients served in Malappuram, Kerala of India served over the past 20 years. 19
The average monthly individual income in Korail destitute society was found to be only $40 ($480 annually), whereas average salary in Bangladesh in 2020 was $325 per month ($3900 annually) 20 which indicates the very low-income level of these dwellers.
The allocation for family welfare in Bangladesh in FY 2019–20 was only 1.02% of gross domestic product (GDP) and 5.63% of total budget allocations. 21 The estimated total health expenditure per capita increased from US$27 in 2012 to US$ 37 in 2015. It was estimated that 67% of total health expenditure was met by households OOPE in Bangladesh, which is the highest in South-East Asia Region, followed by India (62%) and far away from Maldives (18%). 22 So, average OOPE for treatment ($952) in this poor marginalized settlement was likely to have devastating impact and considerable financial risk. Twenty two percent of patients were unable to assess or did not know their diagnosis whereas 10% guessed by themselves rather than having it explained by anyone or health professionals. Still almost 65% were told by their doctors. During this program, almost 23% of the patients died but among the surviving group, most preferred to continue receiving care. The death rate reflects that palliative care still has an important role to play especially for the elderly with pain relief and other supports toward the end of their lives. However, the reported death rate was much lower than for the similar palliative care program in Kerala (56%). 18
Hypertension, stroke and cerebrovascular diseases and other chronic illnesses were the most commonly addressed diagnoses rather than cancer. Most patients were mobile and ambulatory, only about 16% were significantly disabled and needed extensive medical and nursing care, though over 89% had some degree of disability. Moderate to severe pain was found in almost half of patients. Weakness was also commonly found, as nutritional support was lacking and many barely had enough food every day.
In addition to experiencing a very hard life in a marginalized group with uncertainties, the burden of chronic diseases exacerbates psycho-social and spiritual concerns in daily life. Anxiety, depression, and sadness were common, and the majority had concerns about care of the family and lack of income or loss of job due to illness.
Both Groups 1 and 2 were similar in terms of age, monthly income, average ECOG score, and current pain. Pain was brought to a comfortable level in 27% of each group, which indicates a need for improved pain control. Palliative care advocates a holistic, comprehensive, and patient-centered approach to address patients’ total experience in the physical, psychological, social, and spiritual dimensions. 23 Psychological, social, and spiritual concerns were adequately addressed by the palliative care team among Group-1 patients. The project always attempted to encourage the family, community, and neighbors to take care of neglected patients and managed to do so among both groups. Group-1 patients’ families and caregivers received extensive training in care giving which resulted in improved quality of life (QOL).
The team responded with 24-hour telephone service, urgent next day visits whenever any emergency arose, and the response was significantly better among Group-1 patients. The project had a significant impact on reduction of OOPE for health care in Group-1 patients by reducing medicine cost and fewer hospital visits and admissions. Regular home visits, outpatient visits, and a variety of medical specialty clinics enriched the support. Similar results were found in other home-based palliative care approaches in New York metropolitan area, 24 Hawaii and Colorado. 25
A similar percentage of both groups would recommend this service to others reflecting some leniency bias, but a significantly higher percentage of Group-1 patients rated the service as very good or excellent. Many of them urged that similar programs be developed. Some of other notable suggestions were launching emergency services, more frequent and specialized physician services, financial aid, and medicines free of charge. Willingness to volunteer or contribute in some way to sustain this project was significantly higher in the intervention group. Their earnest wish for sustainability of the project may be the result of the positive impact of the services on reducing their suffering. Overall, the results of the comparison of evaluation of care between the two groups demonstrated the significant and positive impact of comprehensive palliative care services.
Limitations
There were several limitations to this study. First, QOL of patients was not specifically measured at enrollment and thereafter impact of the program on their QOL could not be quantified though aspects of QOL, such as pain control were assessed. Second, the intervention group study sample, could not be randomized. Other differences (e.g. less health care needs, can walk to OPD service at hub, better ECOG performance, and solvency than Group 1) could account for variation in evaluation of services. Third, the reasons behind rejecting the service were not explored. Fourth, more structured monitoring and evaluation from the beginning of the project would have yielded more versatile data on the impact of palliative care on study subjects.
Conclusion
This study has shown the significant impact of community palliative care on the lives of impoverished older people and indicates the strength of this care model. In Bangladesh, where palliative care is scarcely practiced, a community-based approach following this model may play an important role in expanding the availability of palliative care. Future studies with larger cohorts and qualitative research are required to further explore the strengths and weaknesses of this home and community-based approach and the experiences and barriers faced by the providers, patients, and caregivers. Learning from this project has been taken forward in a new project in Narayanganj, Bangladesh.
Footnotes
Acknowledgements
The authors are grateful to all the program coordinators, palliative care assistants, doctors and nurses from BSMMU who contributed and made this project successful. They acknowledge with gratitude the cordial support of their patients and families of Korail community. Finally but not the least, they thank WHPCA for funding this project and facilitating improvement of quality of life of older people in the indigent community and the Palliative Care Society of Bangladesh (PCSB) for extending their help with financial support at a later part of the journey.
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Worldwide Hospice Palliative Care Alliance (WHPCA).