
Abstract
Background:
Parents of children with life-limiting illnesses experience considerable burden and distress, yet few interventions have targeted their well-being.
Objectives:
Evaluate the use and feasibility of the Paediatric Carer Support Needs Assessment Tool (pCSNAT) in assessing and addressing parents’ needs caring for cancer and non-cancer conditions. Carer well-being outcomes were also tested.
Methods:
A non-randomised prospective intervention pilot study. Twenty-eight parents (out of 42 approached) and 5 health professionals working in paediatric palliative care services in Western Australia (2018–2019) completed the pilot study.
Results:
Two-thirds of eligible parents completed the study. The highest support needs included having time for yourself; practical help in the home; knowing what to expect in the future; financial, legal or work issues; and knowing who to contact if you are concerned. Almost all needs were considerably more pronounced for the non-cancer group. The pCSNAT seemed feasible and outcomes demonstrated a tendency to improve.
Conclusion:
Using the pCSNAT provided a concise and comprehensive ‘one stop shop’ for health professionals to evaluate difficulties encountered by parents. The disadvantages reported by the non-cancer group warrant increased attention. Paediatric palliative care should adopt routine assessment of parents’ support needs to anticipate early and tailored supports including partnerships with the community.
Keywords
Introduction
Paediatric palliative care (PPC) focuses on providing holistic and integrated care to enhance the quality of life of children and young people with life-limiting illnesses while also supporting their families. 1 A key principle of family-centred care is for professionals to work with families to ensure the best interests of the child and family are addressed.2–4 In Australia, the health department policy identifies children and their family caregivers to be central in the care model, with their physical, spiritual, psychosocial and cultural needs determining appropriate care. 5
However, in clinical practice, a gap remains between this optimal approach of family-centred care and reality. 6 Families with seriously ill children face complex challenges including stress on siblings, physical and mental health issues, financial and work problems, relationship issues, social isolation and high distress. 6 Parents report high levels of distress and burden, low quality of life and unmet emotional and practical support needs. 7 Parents place their personal needs aside to focus on their child’s needs. This may be feasible in the short term when a child is suffering from an acute illness; however, when a child has a life-limiting illness, placing personal needs aside for months and years can have detrimental effects on the parents’ health and well-being.8,9 However, when involved in the planning of their child’s care, they feel empowered in being able to anticipate the child’s needs as the illness progresses. 10 The long, debilitating trajectory of some non-cancer diseases can also lead to negative effects on the parents’ mental health 11 and to high levels of stress around feelings of burdening other family members and of financial strain. 12
Despite the known unmet needs of parents of PPC patients, there is no formal systematic assessment approach embedded in practice to identify and address these needs in a paediatric setting. The Carer Support Needs Assessment Tool (CSNAT) is a validated adult palliative care tool designed to identify and address the individual support needs of carers of adults with life-limiting conditions. 13 The CSNAT approach also involves creation of an action plan in response to the needs assessment and further reviews and follow-ups (more details in the ‘Methods’ section). The effectiveness of the CSNAT approach has already been demonstrated in the adult setting, with family carers and service providers greatly appreciating the benefits of this approach.14–16 However, the key challenge to improve practice is for practitioners to change from the prevailing ad hoc approach to a person-centred carer-led systematic approach as advocated by the CSNAT.
In an Australian study (undertaken in 2013–2014), Collins and colleagues 7 used the CSNAT to assess the unmet needs of parents in a cross-sectional design; however, the study did not extend to developing and reviewing action plans to address the needs. The sample included both cancer and non-cancer conditions, but the analyses did not distinguish between the two groups. A small American study trialled the paediatric version of the CSNAT (as explained in the ‘Methods’ section) as part of an intervention for advance care plans (ACP). 17 The sample included only non-cancer conditions. The study concluded that an apparently difficult topic to broach was facilitated by the CSNAT process of regular conversations that elicited palliative care needs and a support plan, with all six families completing the ACP.
Objectives
The aim of this pilot study was to evaluate the use of the Paediatric Carer Support Needs Assessment Tool (pCSNAT) in assessing and addressing parents’ needs for support while caring for their ill children, with cancer and non-cancer conditions, in the PPC setting in Western Australia (2018–2019) in order to inform a future larger study. Specific objectives were the following:
Identify and compare the profile and the support needs of parents caring for children requiring palliative care from both cancer and non-cancer groups.
Assess the feasibility and initial implementation outcomes of pCSNAT related to parent strain, distress, positive appraisals, family well-being and preparedness to care in this paediatric setting.
Methods
The project was approved by the Ethics and Governance Committee of the Child and Adolescent Health Service (RGS0000000772) and La Trobe University Research Ethics Committee. Reporting is consistent with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 18 Participants provided their signed written consent prior to the start of data collection. Two health consumers (parents with experience of the PPC service) informed the project.
Setting
PPC services in Western Australia are located at the specialist children’s hospital. They provide care for children with life-limiting diseases and their families in line with recognised definitions of PPC by supporting children and their families from time of diagnosis of a life-limiting condition through their illness including end-of-life and bereavement care. Inpatient and outpatient services are provided in addition to support and delivery of care in the home by close collaboration with local providers across the state. The service usually has about 70 children requiring palliative care.
Eligibility
Parents of children (18 years and younger) receiving palliative care were invited to participate. They needed to be able to speak, read and understand English. Parents of children who were assessed to be within 6–8 weeks of dying were not eligible for inclusion.
Design
This was a non-randomised prospective intervention pilot study to evaluate the parents’ support needs and the likely impact of the intervention on parent outcomes. The researchers delivered a 2-h intervention training session for health professionals. The intervention and all the tools were initially pilot tested with six parents.
Description of the intervention: pCSNAT
The CSNAT is a validated evidence-based tool used to systematically identify family carer support needs during their relative’s end-of-life care and is carer-led but facilitated by the health professional (HP). The CSNAT is structured around 14 broad domains that fall into two distinct groups: those enabling the caregiver to care and those that enable more direct support for the caregiver. It is brief but comprehensive and enables caregivers to identify the domains in which they require further support, which can then be discussed with health professionals and an action plan developed. The tool has demonstrated sensitivity to change over time and has face validity as well as content and criterion validity. 13
The CSNAT has been used in several trials in Western Australian adult populations, including in caregivers of terminally ill patients,14–16 in motor neurone disease 19 and for older people discharged from hospital.20,21 The CSNAT was adapted for use in a paediatric setting in the United States. This adaptation was created through a process of community-based participatory research with parents of children living with rare diseases in Washington, DC. Semi-structured interviews and conference calls with parents led to the addition of items about spouses and siblings, and to changes in wording more appropriate for paediatric patients not in hospice, but medically fragile. 17 Two items were subsequently added to the CSNAT: ‘… taking care of others in the home (e.g. siblings, ageing parents and grandparents?’ and ‘… your relationship with your spouse or partner?’, resulting in the pCSNAT having 16 domains and used in this study.
The pCSNAT approach has five stages:
The pCSNAT is introduced to the parent by the HP during a home visit, clinic encounter or inpatient admission.
The parent is given time to consider in which domains they require additional support.
The HP and parent discuss the domains where more support is needed to clarify and prioritise their specific needs during an assessment conversation.
A shared action plan is developed with the parent involved in identifying the type of input they would find helpful (rather than delivery of ‘standardised’ supportive input).
A shared review is planned.
Recruitment and data collection
Eligible parents with a child known to palliative care and attending a clinical appointment were identified and invited to participate. They were provided with information sheets about the study, given the opportunity to ask questions and completed a signed consent form and the outcome measurement tools (baseline).
The pCSNAT was completed during a scheduled clinical appointment or over the telephone when deemed appropriate by the HP. Parents completed the pCSNAT for a second time within 2–8 weeks of the initial encounter. The shorter time period was necessary to include those with terminal cancers and imminently dying and when the parents are at their most vulnerable time to benefit from the intervention; otherwise, we would have missed on including the cancer group in this study. The longer time period was suitable for the non-cancer group who did not need a review within a short time period. Post-testing of outcome measurement tools (follow-up) took place approximately 2 weeks after the second pCSNAT had been completed.
Outcome measures
Outcome measures were completed before and after the intervention. These tools were chosen because of their performance in other similar studies that used the CSNAT in the adult population.16,21
The Preparedness for Caregiving Scale 22 shows changes over time in caregiving preparedness. It has eight items scoring from 0 = not at all to 4 = very well prepared. Satisfactory internal consistency, reliability and stability, and unidimensionality were reported. 22 The higher the score, the better prepared. A change in the total score of two points was considered to be clinically meaningful, given that this would mean a change such as from ‘not at all prepared’ to ‘somewhat well prepared’ in one item or from ‘pretty well prepared’ to ‘very well prepared’ in two. 22
The Family Appraisal of Caregiving Questionnaire Palliative Care 23 (FACQ-PC) shows changes over time in caregivers’ impacts from caregiving. It has four sub-scales: Strain, Distress, Positive Appraisals and Family Well-being. Scores are from 5 = strongly agree to 1 = strongly disagree. It has good internal consistency reliability and construct validity. 23
Feasibility measures
Feasibility was assessed using the following indicators: the proportion of parents enrolled from those approached, the proportion who completed the intervention from those enrolled, the proportion who had an action plan and the proportion who completed the outcome measurements. In addition, parents were asked to rate their experience completing the pCSNAT on a scale from 1 to 5 (1 being very difficult and 5 being very easy) and to rate how helpful was completing the pCSNAT in getting the support they needed on a scale from 1 to 5 (1 being very unhelpful and 5 being very helpful).
HPs were asked to rate how comfortable they were generally about using the pCSNAT in everyday practice on a scale from 1 to 5 (1 being very comfortable and 5 very uncomfortable), whether the pCSNAT prompted reviews of support put in place (yes, no) and whether they recommended the use of the pCSNAT as a standard/routine practice in their service on a scale from of 1 to 5 (1 being strongly agree to 5 strongly disagree).
Analyses
Descriptive statistics were used to describe the demographic (patients and parent carers) and clinical profile (patients) and the needs as identified by the pCSNAT. Data were analysed using the SPSS statistical software package version 24. A paired t test was used to compare pre-intervention versus post-intervention responses to the two outcome measurement tools. Sample power was not calculated as the primary objective of the study was to test the applicability of the tool in this setting and not to achieve significance.
Results
Participants’ characteristics
Forty-two eligible parents were approached for enrolment; 33 agreed to participate and 28 (8 with cancer and 20 with non-cancer) completed the study consisting of the pCSNAT intervention, pre- and post-intervention outcome measures and the feedback interview. Reasons for declining to participate or not completing the study were due to the child rapidly deteriorating or because of the parent feeling overwhelmed.
Most parents were women (93%) with age ranging from 27 to 55 years (mean = 41.7 years; SD = 8.4). Eighty-two percent of parents were married/de facto and 14% were separated/divorced. Seventy-five percent of the parents had an Australian background. The age of the children ranged from <1 to 18 years with a mean of 9.4 years (SD = 5.5). The median time from diagnosis was 64 months, the median time since the child first became unwell was 94 months, and the median time since referral to palliative care was 23 months (Table 1).
Demographic characteristics of parents (and their children) who completed the study.

SD, standard deviation.
There were differences in the profile of parents in the two groups. The non-cancer group had higher proportions of Australian-born (85% versus 50%), lower proportions of employed (35% versus 75%), higher proportions from rural areas (25% versus 12.5%), a longer median period of child being unwell (140 versus 24 months) and a longer median period since diagnosis (123 versus 34.5 months), compared with the cancer group, although both groups had similar median time since referral to palliative care (24 versus 20 months) (Table 1).
Support needs and actions taken
Time frames and contacts
The median period between the first and second pCSNAT contacts was 34 days (mean = 42 days, SD = 23, range = 14–99 days). Fifty percent of first pCSNAT contacts and 7% of second pCSNAT contacts were face-to-face, and the remainder were conducted by telephone.
Support needs identified by parents
The HPs discussed with the parents their support needs during the two pCSNAT contacts. Figure 1 shows the support needs identified by the parents at the two time points.
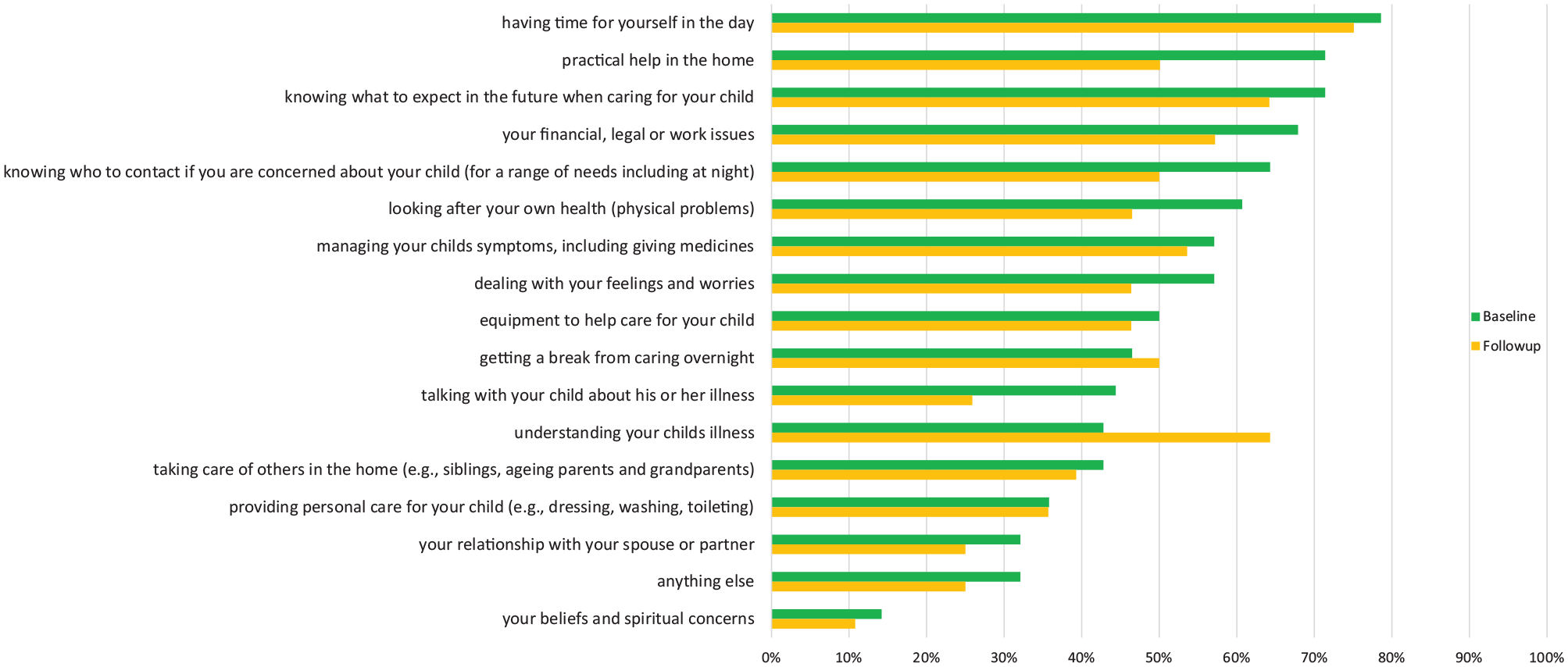
Support needs identified by parents at baseline and follow-up, n = 28.
The top five needs, with proportions of parents needing support ranging from 65% to 78% at baseline, were the following: having time for yourself in the day (direct support); practical help in the home (direct support); knowing what to expect in the future when caring for your child (enabling support); financial, legal or work issues (direct support); and knowing who to contact if you are concerned about your child (enabling support).
Three of the five needs related to direct support needs for the parents. The need to understand the child’s illness was high at follow-up, and that was mainly for the non-cancer group. The two specific paediatric items for the pCSNAT 17 identified that approximately 40% of parents had needs in ‘taking care of others in the home’ and about 30% had ‘needs in managing relationship with spouse/partner’.
The item ‘anything else’ consisted mainly of needs related to children transitioning to adult services, navigating the National Disability Insurance Scheme (NDIS) system and disability services, and psychosocial support for family members such as siblings and grandparents who helped care for the ill child.
Actions taken by HPs for the top five needs
The action plans discussed by the parents and HPs and suggested solutions to address the top five unmet needs are presented in Table 2. The conversations were about what the parents could do for themselves and what could the service do for parents in terms of the internal capacity to help or reaching out and referring to external health and community services. Action plans also explored the families’ own social and informal networks to provide support and peer support from other families in similar situations.
Examples of action plans discussed between parents and HPs.
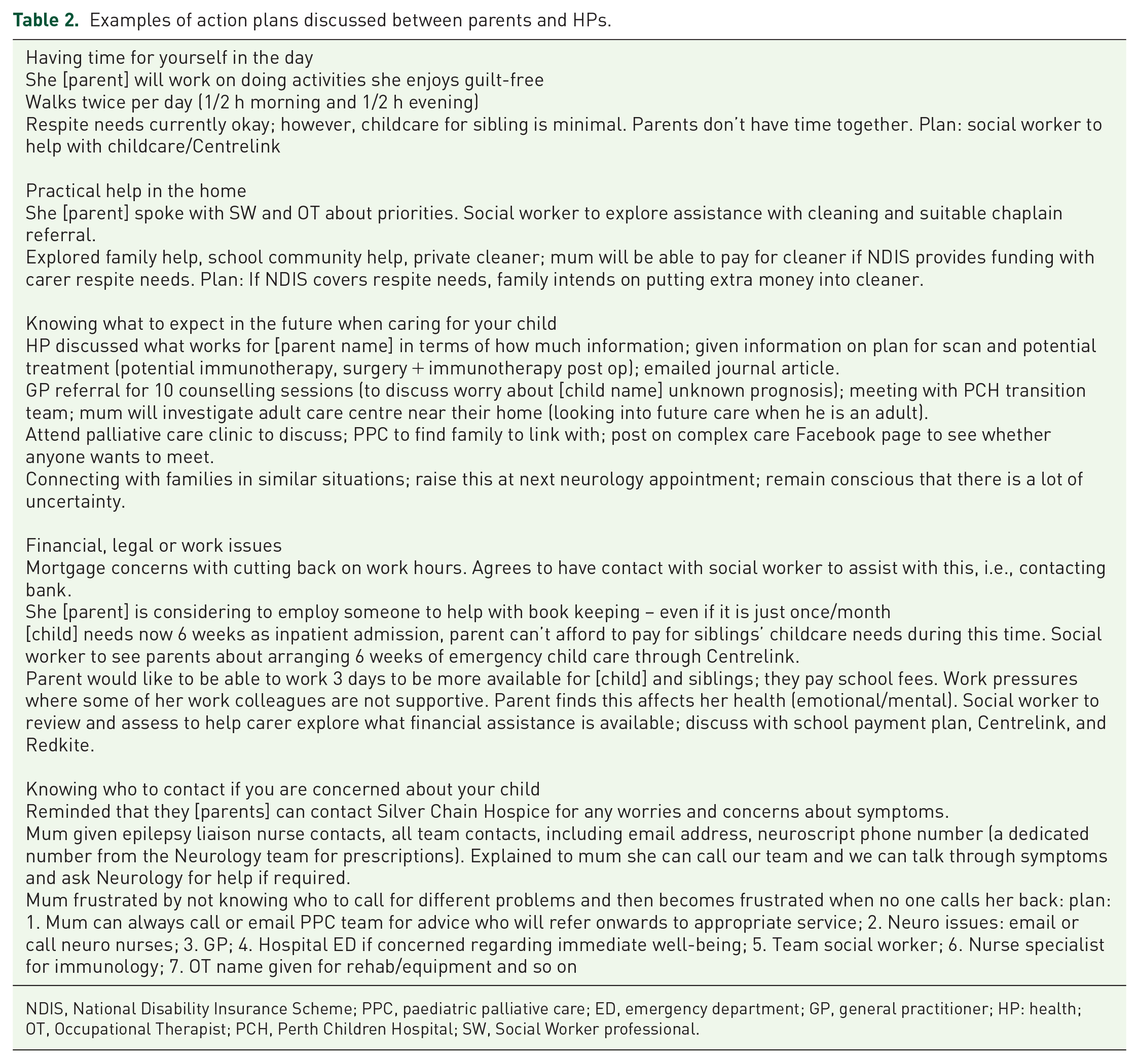
NDIS, National Disability Insurance Scheme; PPC, paediatric palliative care; ED, emergency department; GP, general practitioner; HP: health; OT, Occupational Therapist; PCH, Perth Children Hospital; SW, Social Worker professional.
Differences in support needs between the cancer and non-cancer groups
The support needs of the non-cancer group parents were considerably greater at baseline (Figure 2): practical help in the home (85%); having time for yourself in the day (85%); knowing who to contact (80%); looking after own health (70%); equipment to help care (65%); getting a break from caring overnight (60%); and providing personal care (50%).

Differences in support needs between the cancer and non-cancer groups at baseline.
The cancer group parents had greater unmet needs at baseline in the following domains: talking with the child about the illness (63%); taking care of others in the home (63%); and relationship with partner (50%)
At follow-up (Figure 3), almost all needs were considerably greater for the non-cancer group parents.
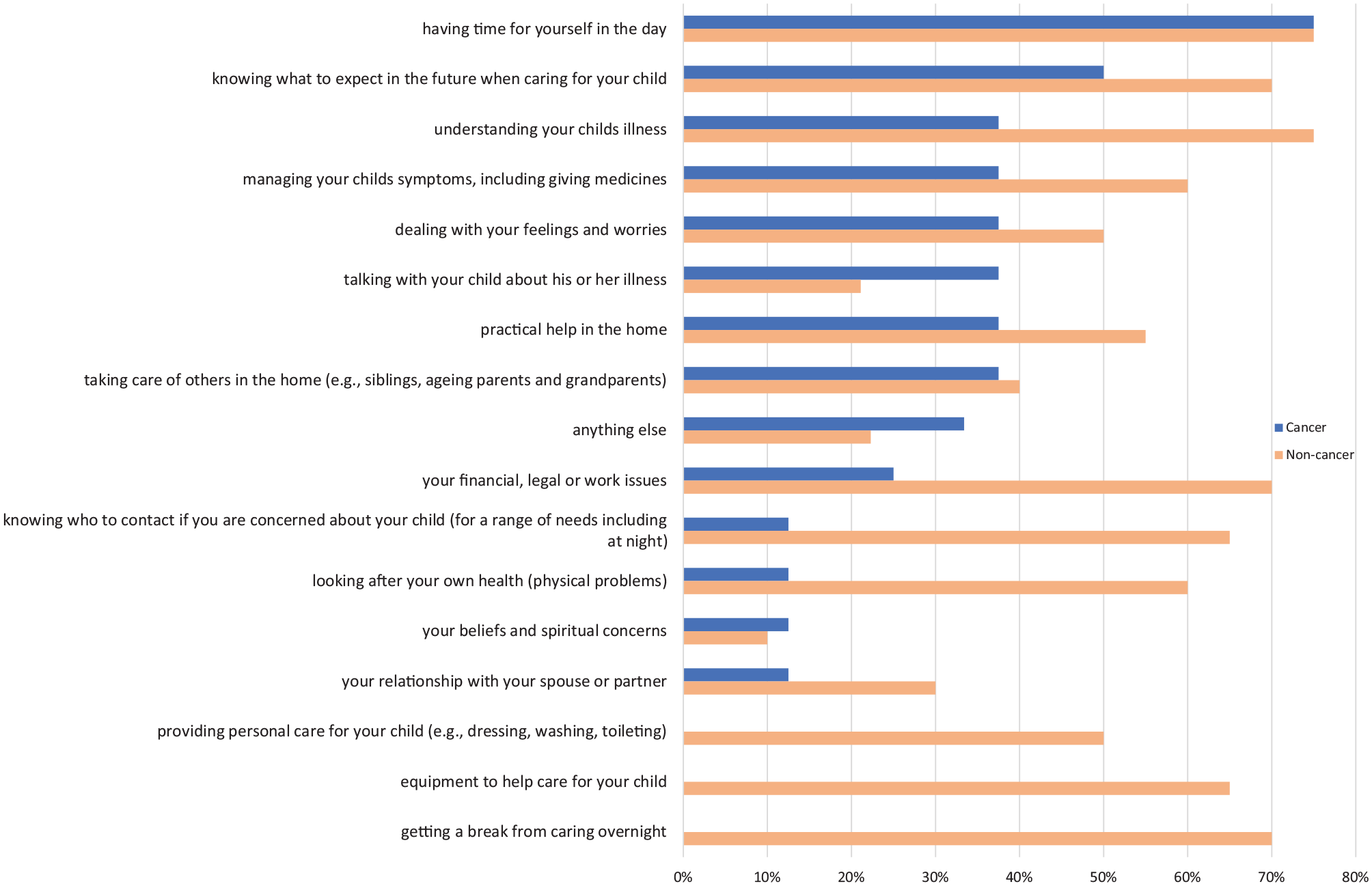
Differences in support needs between the cancer and non-cancer groups at follow-up.
Outcome measures
Parent strain and distress scores (FACQ-PC) decreased between the two time periods. Although not statistically significant, the p-value was 0.09 for distress. Improvement in the family well-being subscale was significant (p = 0.05), but positive appraisals stayed the same between the two time periods (Table 3). The mean preparedness to care score improved, though not significantly.
FACQ-PC scales at baseline and follow-up.

SD, standard deviation; FACQ-PC, Family Appraisal of Caregiving Questionnaire for Palliative Care.
Means tested using paired t-tests.
Regarding the individual items of the Preparedness to Care scale (Table 4), the item measuring ‘parents’ ability to respond to and handle emergencies’ involving their sick child improved significantly (p = 0.043). Parents’ ability to ‘take care of physical needs’ marginally improved between the two time periods (p = 0.09). There were no significant differences in mean outcome measures between the two groups.
Preparedness for Caregiving Scale at baseline and follow-up.

SD, standard deviation.
Nonparametric methods used – Wilcoxon Signed Ranks test.
Feasibility measures
Seventy-eight percent of approached eligible parents were enrolled and 85% of those enrolled completed the study (or 67% of approached eligible parents completed the study). All 28 parents completed the first and second CSNAT contacts and had action plans developed. Between 25 and 28 parents completed the outcome measures, with three parents missing four data points in their caregiver strain subscale of the FACQ-PC at baseline.
Ninety-six percent (n = 27) found the CSNAT ‘very easy to easy’ to complete, 68% (n = 19) found it ‘very helpful to helpful’ to obtain timely support, 29% (n = 8) found it moderately helpful and only one found it unhelpful. The parents who gave lower ratings clarified that their scores reflected their frustrations about the complexities they faced in getting support from government agencies rather than any internal service support.
Three HPs were ‘very comfortable’ using the CSNAT and one was ‘somewhat comfortable’ but only initially. However, there were mixed responses as to whether the CSNAT prompted timely reviews of action plans due to resources and time constraints. Review time periods ranged from 14 to 99 days, aided by reminders from the research team. All four HPs agreed that the CSNAT should be included in routine practice.
Discussion
The goal of this pilot study was to test the methods and procedures that would be used in a large-scale test of the intervention. It tested the pCSNAT approach in a paediatric setting, with comparative analyses between cancer and non-cancer groups of parents. It demonstrated that it is suitable to use the pCSNAT in this paediatric setting, as evidenced by two-thirds of eligible parents concluding the study and completing the pCSNAT during a scheduled clinical appointment or by telephone. The outcome measures were readily completed by parents before and after the intervention. Despite the limitations posed by the small sample, all outcomes demonstrated a tendency to improve, with strain and distress demonstrating a tendency to decrease, while the positive appraisals, family well-being and preparedness to care showed a tendency to increase. Such directionality of effects in a pilot study is a promising result 24 and especially that carer strain of parents has been found to strongly correlate with their quality of life. 7
The need to understand their child’s illness increased after the pCSNAT intervention likely for the following reasons: The intervention gave parents time out of the daily demands of caregiving to reflect on their understanding of their child’s illness; the questions may have increased their realisation that their understanding of their child’s illness was not complete; and this in turn may have increased their confidence and motivation to seek more information about their child’s illness.
Psychosocial support for siblings and grandparents who help care for the ill child has emerged as a distinct issue that could not fit within the existing item of ‘taking care of others in the home’, and this is an item worth including and testing in a larger trial.
One HP explained the difference: Supporting siblings/grandparents in dealing with the grief and stress in having a very ill sibling/grandchild is very different to the practical issues of siblings/grandparents (after school activities, meals etc) …. this needs to be a different question. It is a distinct issue for paediatric palliative care.
Financial, legal or work issues featured highly in the needs of parents of children with terminal illnesses in contrast to settings with adult populations where it was rated much lower.16,20 Parents in this study were of working age and raising families; however, only 35% and 75% of the non-cancer and cancer groups, respectively, were employed. The Australian NDIS added another layer of complexity to navigate the system and funding allowances for respite and other needed support.
At both baseline and follow-up, almost all needs were considerably more pronounced for the non-cancer group. This could be due to the considerable differences in the lengths of illnesses between the two groups, the heterogeneity of illnesses within each group and the extent and nature of formal and informal support available for the two groups. One HP commented, Many illnesses in the non-cancer group are ill-defined with very uncertain trajectories that span many years accompanied by severe disability requiring constant support and equipment such as for physical moving, and by consequence years of disturbed sleep and other adverse carer outcomes.
In this study, parents in the non-cancer group had children who had been unwell since diagnosis for a median period that was four times longer than the cancer group (123 compared with 35 months). The non-cancer group parents reported higher unmet needs in knowing who to contact if they were concerned, and this could be a reflection of care being provided by multiple teams rather than the single team approach for families of children with cancer. This was apparent in Table 2 where HPs were assisting frustrated parents to know who to call for the different problems they were encountering. Parents and HPs reported that informal support networks and non-government organisations were not available to the non-cancer group to the same extent they were for the cancer group. For a cancer diagnosis, there were established informal and social networks. By contrast, the non-cancer group of parents were more likely to become socially isolated if their child was unwell needing chronic long-term and complex care, which reduced their opportunities to connect with social networks. One HP reflected, Parents from our cohort [non-cancer] often describe feeling like the poor cousins to the cancer group- they are aware if their child had a cancer diagnosis they would have access to additional supports (sibling camps, help with utilities for example).
It is interesting that most of the challenges reported in this study, particularly for the non-cancer group, were the same as those reported 13 years ago in a study undertaken in this paediatric tertiary hospital. 25 The same differences in the profile, care burden, complexity and long-term duration of care, social and physical isolation, information needs and coordination of care between the two groups were highlighted. More recently, Collins and colleagues 7 reported that the higher proportion of non-cancer conditions in their study could have contributed to the demonstrated high levels of distress, burden and unmet needs.
While access and availability of clinical support have improved for both groups since the 2007 study, what remains of significance are the differences in support that these two groups receive from the not-for-profit and community-based organisations and the partnerships between formal and informal networks which are better established for cancer.
Implications for practice
Despite the clear benefits for family carers in many previous studies of adult populations, introducing comprehensive assessment of carer needs into routine practice is still a challenge or an aspiration as highlighted by the CSNAT developers: ‘While there is clear research evidence and positive policy ambitions to achieve comprehensive, person-centred assessment and support for carers, so far these remain as aspirations in practice delivery’. 26 They reported 10 organisational barriers that can be overcome by a number of strategies that include consistent identification of carers, a protocol for needs assessment, a recording system separate to patients, time and workload capacity of staff, and support from senior managers. 26
As in previous Australian CSNAT studies undertaken in different settings,16,19,27 time and workload capacity of staff, particularly in undertaking regular reviews of carer needs, was a challenge that was encountered in this study. One suggestion, that could have assisted prompting for reviews, is the tool having a scoring system to alert to severity of needs. This could have elicited more timely reviews by HPs who could prioritise their follow-ups according to severity of these needs. One such evidence-based tool with a scoring system is the Carers’ Alert Thermometer. 28 However whichever assessment approach is used in routine clinical practice, service providers would need to make the judgement when to introduce it and how often.
The issues identified by the non-cancer group in all domains of needs warrant more attention for development of more tailored and coordinated models of care, including the support from the non-government sector. This may also involve partnerships with the community to boost the support of the informal networks for example, through a Compassionate Communities Model of end-of-life care, 29 which harnesses the informal resources inherent in communities. 30
Limitations
The difference in number of participating parents of non-cancer versus cancer patients is compatible with proportions reported in the literature. Fraser and colleagues 31 reported that the distribution of life-limiting diagnoses comprised only 13.7% oncology, with the majority being congenital anomalies and neurologic diagnoses. A study undertaken in the same hospital in Perth 13 years ago 25 had 15% cancer and 85% non-cancer, and Collins and colleagues 7 had 85% of their sample consisting of non-cancer conditions. Our study had a higher proportion of cancer diagnoses compared with the literature (29% cancer and 71% non-cancer).
It is to be expected that outcomes would not be significant considering the small sample size and the relatively short follow-up period for changes to take place. These findings will inform a larger study regarding suitability of design and outcome measures. Further details on other acceptability matters captured in interviews with parents and HPs will be covered in a forthcoming article. The results of this study may not be generalizable to parents who are not receiving palliative care from this tertiary service or not at all, and therefore their unmet needs and well-being outcomes will differ and possibly these may be worse.
Conclusion
This project has shown that there is a benefit to using a systematic and evidence-based approach to assessing and addressing the support needs of parents in a timely manner. Using such a short form provided a concise and comprehensive ‘one stop shop’ for HPs to identify and address problems encountered by parents. Such problems have been usually reported in a piecemeal manner using lengthier questionnaires to assess the same aspects of needs but stopped short of implementing the necessary strategies. This pilot study has demonstrated that this intervention is appropriate for further testing in larger studies using a longer follow-up period.
Footnotes
Acknowledgements
We gratefully acknowledge the participants (parents and health professionals) for contributing to this research project, the consumer representatives for their advice and Taryn Vose for her assistance.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from Health Department of Western Australia through the WA Cancer and Palliative Care Network and supported by La Trobe University and Perth Children’s Hospital.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.