
Abstract
“Cystic hygroma” is defined as a fluid-filled sac, resulting from a blockage in the lymphatic system. This large, deep, diffuse swelling commonly occurs in the neck as a result of the congenital malformation of lymphatic system having an equal distribution between males and females. It results as a failure of development of the communications between lymphatics which is mostly found in the posterior triangle of neck. Its recurrence rate may be up to 10%–15%. Different treatment modalities for treating cystic hygroma are surgical excision, sclerotherapy, laser and radiofrequency. Here we report a rare case of cystic hygroma present in a 20-year-old male on left side of his neck treated by total surgical excision of the lesion. The patient is on regular follow up for 12 months and he has been asymptomatic till now.
Introduction
“Hygroma” is a Greek word means water-containing tumor. Cystic hygroma or cystic lymphangioma is a subtype of lymphangioma. It forms due to an aberrant proliferation of lymphatic vessels, resulting from abnormal development of the lymphatic system. 1 Patients with cervical cystic hygroma have an obstruction between venous and lymphatic drainage leading to accumulation of lymph in the jugulo-lymphatic sacs of the nuchal region. 2
Cystic hygroma occurs more frequently as compared to other types of lymphangioma, composing of single or multiple macrocystic lesions and having scarce communication with normal lymphatic channels. There are multiple proposed mechanisms to explain the pathophysiology of a cystic hygroma. Embryologically these lesions are thought to originate from sequestration of lymphatic tissues during the development of lymphatico-venous sacs. These sequestered tissues fail to communicate with remainder of the lymphatic or venous system. Later on, dilatation of the sequestered lymphatic tissues ensues, resulting in the cystic morphology of these lesions. 3 Cystic hygromas can also be associated with chromosomal abnormalities such as Down syndrome, Turner syndrome and trisomy of chromosome number 13 & 18. 4
Children below the age of two years are usually affected with cystic hygroma and it is quite rare in adults. It can be manifested anywhere in the body and the clinical presentation depends on its size, anatomic location and rate of growth of malformation. 5 The common locations are cervicofacial regions (especially posterior cervical triangle), mediastinum, axilla, groin and floor of the mouth. 1 Although the cause of cystic hygroma in adults is uncertain, its onset is thought to be triggered by both trauma and upper respiratory tract infection. 5
On clinical examination, these lesions appear soft, non-tender, compressible, trans-luminant and without any bruit. 6 However, cystic hygroma does not cause significant morbidity except for facial disfigurement, restricted neck movement, sudden increase in size due to infection, hoarseness, dysphagia and rarely respiratory difficulties. 5
Diagnosis of cystic hygroma in adults is more challenging than in children and the final diagnosis is usually made based upon histopathological examination. These cysts may produce a milky, serous, serosanguinous, yellowish or straw-colored fluid, on aspiration with a wide-bore needle during a Fine Needle Aspiration Cytology (FNAC). 6 Cystic hygroma can be confused with a branchial cleft cyst, ranula, teratomas, thyroglossal cyst and thyroid goiter based on its presentation. Ultrasonography (USG) of the lesions usually features a multicystic appearance with internal septations without any blood flow and it can be detected on color Doppler ultrasonography. 7 Other modalities like Computed Tomography (CT) scans and Magnetic Resonance Imaging (MRI) can be employed to delineate the lesion. 8
The most preferred modality for the treatment of cystic hygroma remains complete surgical excision of the lesion; however, many recent studies in the literature have increasingly documented remarkable results for management of such lesions with sclerosing agents. Although, suitable treatment options should be selected based upon case-to-case variation. Optimum treatment can be given by surgery alone, sclerotherapy alone or a combination of both. Recently invented treatment modalities such as laser and radiofrequency can also be used in selected patients. 9
Here we report a case of cystic hygroma in left side of the neck of a 20-year-old male treated with total surgical excision.
Case Report
A 20-year-old male reported to the out patient department of our Institution with complain of a swelling present on left side of the neck for five years. The swelling gradually increased in size to attain the present size. Patient had no other compressive neck symptoms like difficulty in breathing and swallowing. He gave no history of previous neck trauma or upper respiratory tract infection.
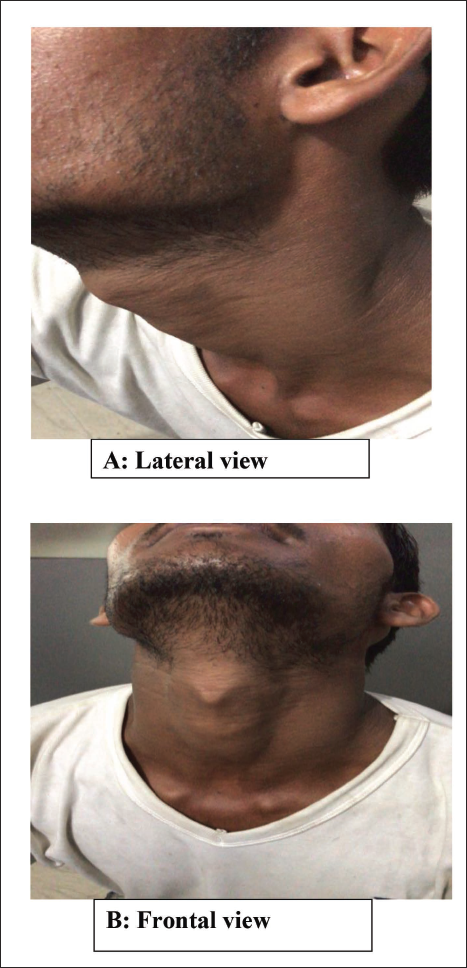
On clinical examination, there was a soft, painless, solitary, freely movable swelling with well-defined margins present in anterior triangle of the neck on left side having size 5×3 cm (Figure 1A and B). The swelling was immobile with deglutition. Overlying skin illustrated no signs of erythema or tenderness. No cervical lymphadenopathy was found.
Pre-operative Extraoral.
Ultrasonography of the neck showed a septated, well-defined, cystic fluid collection of size 4.29×2.24×4.35 cm and volume 21.92 ml in the left anterior triangle.
MRI findings showed a well-defined cystic lesion measuring 4.5×1.2×6.4 cm in the left side of neck located deep to the sternocleidomastoid muscle. It was located posterior to left carotid and internal jugular vessels. Superiorly it was seen to be extending up to the inferior margin of the mastoid bone and inferiorly up to the C4-C5 level. No obvious evidence of vascular encasement or any internal solid component was seen.
FNAC was performed to draw a final diagnosis. Thick, viscous fluid was aspirated from the cyst and the cytological analysis was found to contain numerous lymphocytes with no malignant cells, making cystic hygroma a probable diagnosis.
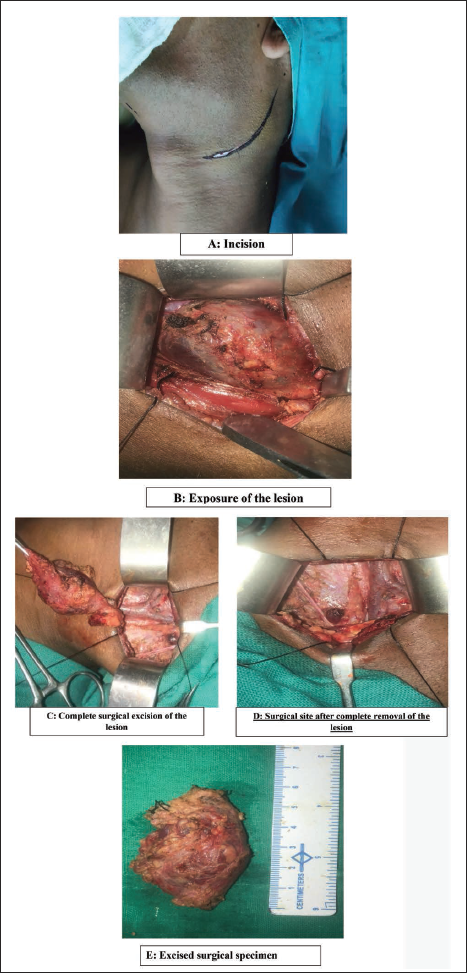
Surgical excision of the lesion was performed under general anesthesia. A curvilinear incision of approximately 6 cm in length was given over the maximum prominence of the swelling (Figure 2A) following which the overlying skin, subcutaneous tissue and platysma flap were raised exposing the cystic mass (Figure 2B). Internal jugular vein and carotid artery were carefully dissected; all important nerves and arteries encountered during dissection were identified and preserved. The lesion was completely excised along with the entire capsule (Figure 2C and D). The size of the cyst was found to be 6×4 cm (Figure 2E). Layerwise closure was performed using 3-0 vicryl for deeper layer and 4-0 prolene for the superficial skin layer. The surgical specimen was sent for histopathological evaluation.
Intraoperative.
The patient recovered well without any sign of neurological dysfunction post-operatively and he was discharged from hospital after three days of surgery.
After a follow-up period of 12 months by means of clinical examination and ultrasonography, the patient remains free of further recurrence.
Discussion
“Cystic hygroma” is actually a misnomer for macrocystic lymphatic malformation and most commonly seen in utero or in infancy below the age of two years. It is rarely found in adults. 10 Cystic hygromas are most commonly located in head and neck region (75%–80%) and typically in the posterior triangle of the neck. 11 Although in this case, the lesion is present in the left anterior triangle of neck. Both men and women are equally affected by this malformation. The etiology of cystic hygroma in adults is controversial, however, infection, trauma and lymphatic obstruction are thought to be the associated factors due to stimulation of the cell rest proliferation resulting in a delayed proliferation of lymphoid cell rest in adults. 12
Several classification systems have been proposed for proper diagnosis and management of cystic hygromas.
13
Three subtypes of cystic hygromas have been described in various literature. The first one is the capillary or simplex lymphangioma. The channels of this type are characteristically thin-walled and small. The second subtype is the cavernous lymphangioma containing a fibrous, adventitial coat and larger, thinner-walled channels than the capillary lymphangioma. The third subtype is called cystic lymphangioma, that is, hygroma containing flattened endothelium along with large cystic spaces. All the subtypes can be present in the same lesion as well.6, 14 de Serres
15
proposed a staging system according to the location and extent of lesions which is as follows:
Stage 1 - Unilateral infrahyoid Stage 2 - Unilateral suprahyoid Stage 3 - Unilateral infrahyoid and suprahyoid Stage 4 - Bilateral infrahyoid Stage 5 - Bilateral infrahyoid and suprahyoid
On clinical examination, a smooth, soft, mobile, trans-illuminable and non-tender lesion was found. Different investigative modalities have been mentioned in the literature and imaging methods like MRI, CT scan and USG can be performed along with FNAC prior to the treatment. 6 In this case also, we have performed MRI, USG and FNAC preoperatively.
Cystic hygroma can be easily misdiagnosed with other cystic neck swellings such as branchial cleft cyst, dermoid cyst, hemangiomas, thyroid mass and other congenital tumors. Generally, this encapsulated lesion is homogenous and non-invasive. The characteristic feature of cystic hygroma is the presence of clear fluid with histiocytes, lymphocytes and proteinaceous debris in the cytology. Microscopic and immunohistochemical analysis via fine-needle aspiration can contribute to getting the final diagnosis. 14
Many treatment options are present for cystic hygroma including sclerotherapy, laser, cryotherapy, embolization, electrocautery, steroid administration and radiation therapy. However, since cystic hygroma is benign in nature, surgical excision of the entire mass is the treatment of choice. 1 Although if residual tumor is left behind during surgical excision, the recurrence rate of cystic hygroma can be found to be 10%–15%. 6
The different other post-operative complications observed following surgical excision of cystic hygroma are mainly hemorrhage, wound infection, hypertrophied scar and lymphatic discharge from the wound. 16 In our case, following one year of regular follow-up, the patient did not complain of any of these post-operative complications and there is no sign of recurrence till date.
Conclusion
The cystic hygromas should be clinically assessed and diagnosed properly, because although they are benign lesions, sometimes complications such as infection, spontaneous or traumatic rupture, nerve compression causing pain and paresthesia, respiratory difficulties, dysphagia and facial disfigurement can arise. The primary goal of treatment of cystic hygromas must be to relieve obstruction upon vital tissues and to obtain a good cosmetic result.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Ethical clearance was obtained from the Institutional Ethical Committee and a written informed consent was obtained from the patient.