
Abstract
Partial trisomy 22 is a rare condition that is found in live birth. In most cases, diagnosis of partial trisomy 22 was made after birth. Herein, we report a prenatal diagnosis of fetal partial trisomy 22 in a 28-year-old pregnant woman presented with fetal cystic hygroma. Structural abnormalities were detected at 16 weeks of gestation: left cleft lip and ventricular septal defect. The G-banding karyotype analysis and fluorescence in situ hybridization showed partial trisomy 22. It is recommended that pregnant women with fetal anomalies should have prenatal genetic diagnosis to ascertain whether the fetus has partial trisomy 22 or other rare chromosomal abnormalities.
Introduction
Trisomy 22 is the second most common autosomal trisomy found in spontaneous abortion. But it is a rare condition that is found in live birth. It is found in approximately 1 in 30,000 live births. 1 Multiple anomalies can be detected in the second trimester and third trimester by ultrasonogram. Abnormal ultrasonographic findings of trisomy 22 are intrauterine growth restriction, nuchal thickening, hypoplastic femurs, oligohydramnios, and multiple structural anomalies such as cerebellar defects, cardiac malformations, ambiguous genitalia, a multicystic left kidney, and an absent right kidney. 2 However, ultrasonogram may be unremarkable in the first trimester. One study found that increased nuchal translucency during the first trimester was identified in one-third of trisomy 22 and cystic hygroma was identified in 2 of 9 cases with trisomy 22. 3 One study had an abnormal combined first-trimester screening results, cleft palate, and double outlet right ventricle in trisomy 22. 4
In most cases, diagnosis of partial trisomy 22 was made after birth. The clinical features of patients with partial trisomy 22 are mental retardation, congenital heart disease, minor skeletal abnormalities (especially extra ribs), and certain facial characteristics (an antimongoloid slant of the palpebral fissures, preauricular tags and sinuses, and low-set ears). 5 There have been a few reports of prenatal diagnosis of partial trisomy 22.6 –8 Herein, we report a case of fetal cystic hygroma detected in the first trimester that led to the diagnosis of a partial trisomy 22.
Case presentation
A 28-year-old pregnant woman (gravida 1, parity 0) with 10 weeks gestation came to the hospital for a second opinion. Ultrasonogram was performed at a private hospital and fetal cystic hygroma was detected. Her past medical history and family history were unremarkable. Ultrasonogram was repeated and revealed that there was a single viable fetus, with a crown rump length of 40 mm, which was compatible with a 10-week gestation with a posterior cervical cystic hygroma (a cystic lesion diameter 25.6 × 3.7 × 33.2 mm3 in the area of fetal neck) (Figure 1). After extensive counseling, she and her husband agreed to have additional investigation by the amniocentesis for karyotyping at 16 weeks. However, she had a non-invasive prenatal testing at 12 weeks. The result showed that there was a low risk for chromosomal abnormalities. Ultrasonogram was repeated before amniocentesis at 16 weeks of gestation. The fetal biometry was compatible with 16 weeks. Structural abnormalities were detected: left cleft lip (Figure 2(a)) and ventricular septal defect (VSD) (Figure 2(b)). Amniocentesis was performed without complications. The G-banding karyotype analysis showed that there was 46, XX, +22, rob(22;22)(q10;q11.2) karyotype in all the analyzed cells (Figure 3). Another test, fluorescence in situ hybridization (FISH), was performed to confirm this genetic result. The karyotype of the woman revealed that she had a normal female chromosome and her husband had a normal male chromosome.

Ultrasonographic findings at 10 weeks: cystic hygroma in the area of fetal neck.

Ultrasonographic findings at 16 weeks: (a) left cleft lip and (b) ventricular septal defect.
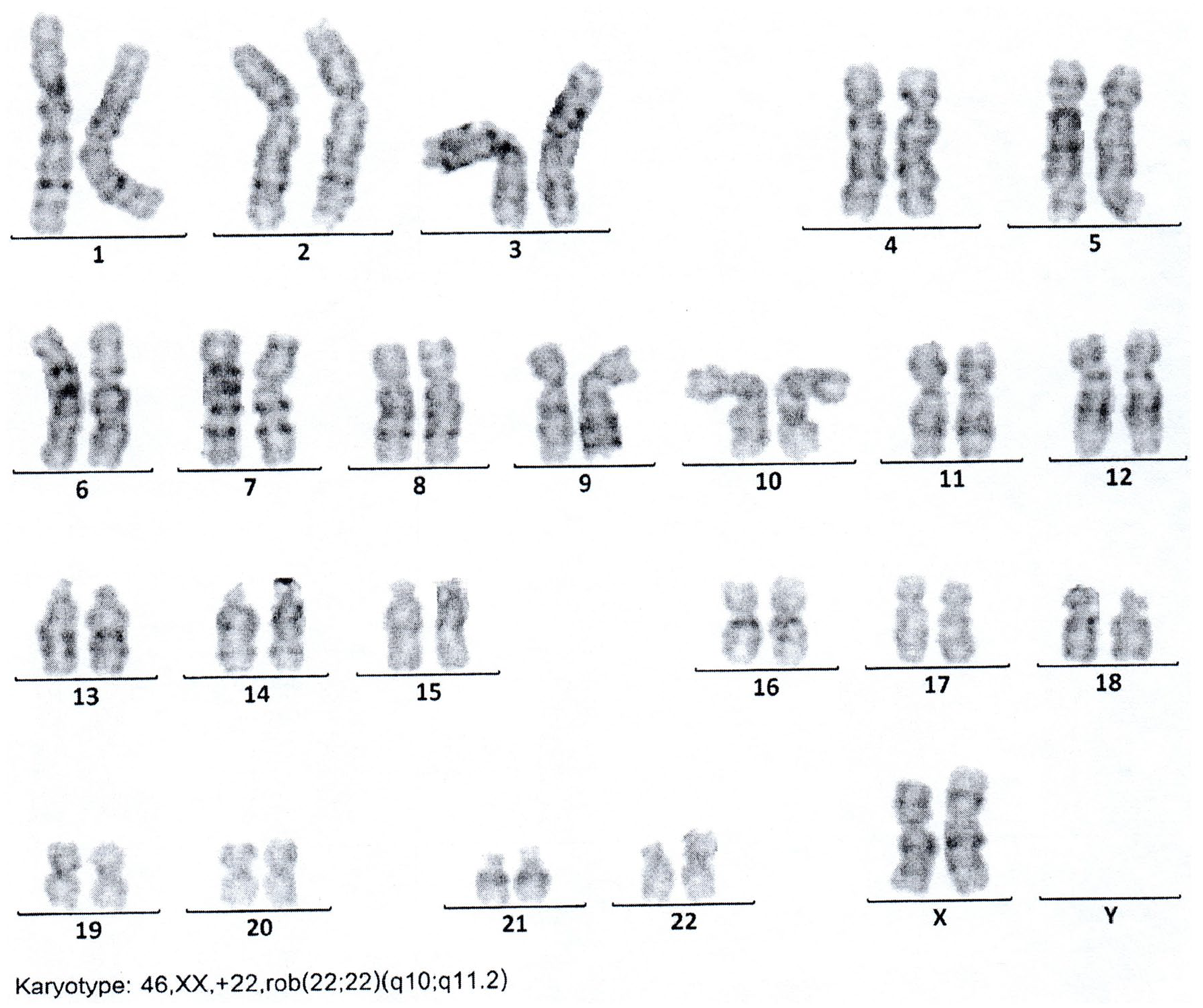
The G-banding karyotype analysis showed that there was 46, XX, +22, rob(22;22)(q10;q11.2) karyotype.
After another extensive counseling, the woman and her husband finally decided to terminate the pregnancy. Termination of pregnancy was performed at 20 weeks of gestation. Postmortem autopsy was permitted. Upon the physical examination, the fetus was found to be female with microcephaly and had the following features: low-set ears, up slant eyes, right preauricular nodule, left cleft lip and palate, and micrognathia (Figure 4). From the autopsy, a VSD, pulmonary hypoplasia, absent ductus arteriosus and gall bladder agenesis as well as bicornuate uterus were found.

Fetal gross findings: microcephaly, low-set ears, up slant eyes, right preauricular nodule, left cleft lip and palate, and micrognathia.
Discussion
This case presented with cystic hygroma in the first trimester that led to the diagnosis of partial trisomy 22. The finding from this case was similar to a previous report that found cystic hygroma in the first trimester of trisomy 22. 3 Fetal anomalies (cleft lip and congenital heart defect) were found in this individual. However, unlike other previous reports, this case did not have many structural anomalies.2,5 This discrepancy may be due to the early diagnosis in our patient.
Cystic hygroma in present case was associated with partial trisomy 22. Cystic hygroma is a congenital malformation of the lymphatic system that appears as fluid-filled cavities, most commonly found in the posterior cervical area.9,10 Cystic hygroma is associated with chromosomal abnormalities. 10 The most common chromosomal abnormalities include trisomy 21, trisomy 18, trisomy 13, or monosomy X. It may be associated with the sex chromosomal abnormalities and fetal syndrome such as Noonan syndrome, achondroplasia, lethal multiple pterygium syndrome, Fryns syndrome, Apert syndrome, Pena-Shokeir syndrome, Cornelia de Lange syndrome, and fetal alcohol syndrome.9,10
VSD was found as cardiac abnormalities in present case. VSD is a common cardiac abnormality. The prevalence is 0.9–6.0 per 1000 live births. VSD can be found as isolated defects or associated with extracardiac, genetic, or syndromic abnormalities. 11 In present case, VSD was associated with partial trisomy 22.
From this patient, cell-free DNA testing could not help to diagnosis due to partial trisomy 22. This case highlights the importance of pre-test counseling for patients who are considering having cell-free DNA testing after having an abnormal ultrasonographic finding. 12 The detection rate of cell-free DNA is 99% and 72% for trisomy 21 and all aneuploidies, respectively. 13 A low risk result of cell-free DNA result indicates that there is a decreased risk, but it cannot definitively rule out trisomy 21 or other chromosome abnormalities as seen in our patient. All pregnant women who undergo a cell-free DNA test should understand the screening nature of the test that it only detects common aneuploidies, has the potential to give unexpected results or fails to obtain test results, and has the possibility to yield false-positive results, and hence the obstetricians should provide their patients with the options for diagnostic testing. 14 This case report confirmed the use of prenatal genetic diagnosis when fetal structural abnormalities were found. 15
Literature review in MEDLINE (1966–2019) search with the term “partial trisomy 22” and “prenatal diagnosis” was performed. We found only 3 publications, a total of 4 cases, including this present case, of prenatal diagnosis of partial trisomy 22 (Table 1). All cases were primigravida. Indication for prenatal diagnosis was a maternal balanced translocation (1 case), a diaphragmatic hernia with intrauterine growth restriction (1 case), a VSD with intrauterine growth restriction (1 case), and a cystic hygroma (1 case). All cases ended with termination of pregnancy. Multiple anomalies were found from autopsy in all cases.
Literature review: 4 cases of prenatal diagnosis of partial trisomy 22.

GA: gestational age; PND: prenatal diagnosis; TOP: termination of pregnancy; IUGR: intrauterine growth restriction; VSD: ventricular septal defect.
Conclusion
It is recommended that all pregnant women with fetal anomalies should have prenatal genetic diagnosis to ascertain whether the fetus has partial trisomy 22 or other rare chromosomal abnormalities as seen in our patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant for International Research Integration: Research Pyramid; Ratchadaphiseksomphot Endowment Fund, Chulalongkorn University; and Placental Related Diseases Research Unit, Chulalongkorn University.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article. Written informed consent was also obtained for publication of the images.