
Abstract
Methods:
A six years retrospective observational study was conducted on 183 patients with Zygomaticomaxillary complex (ZMC) fractures. We analyzed prevalence of age, gender distribution, etiology, location and mode of treatment.
Results:
In our study, the mean age was 33±14.5, gender distribution 68% males and 32% females, etiology of ZMC fractures was 114 road traffic accident (RTA), 44 falls, 12 sports injuries, five interpersonal violence, four animal bites, and four work-related. Results show that the treatment options applied are 37 conservative management and 146 open reduction internal fixation.
Conclusion:
In this study, male predilection to ZMC fractures was seen, RTA being the most common etiology and the most common site of fracture was Zygomaticomaxillary buttress region. There are different treatment protocols for the management of ZMC fractures. In our study, two-point fixation was the most common (35%). Concluding upon our experience and the results derived from our study, various methods are used to stabilize zygomaticomaxillary complex fractures. Relying upon the characteristics of the fracture, open reduction and internal fixation with mini plates is the most reliable modality providing three-dimensional stability.
Keywords
Introduction
Most commonly treated facial injuries by oral and maxillofacial surgeon are zygomatic-orbital fracture. 1 The maxillo-facial region (MFR) consists of hard and soft structures of face which stretch from the forhead above to chin below. Face is most of the visible portion of the body, most vulnerable to injury. 2 Zygomatic fracture is one of common fracture due to its elevation, predisposing it to brace the burden of injury. 3 Trauma to the face, injures the skeletal components, dentition, and soft tissues. Trauma to MFR are becoming more common and severe as a result of the population’s increased socioeconomic activity and reliance on road transportation. 2
Zygomatic bone works as a buttress and contributes greatly to strengthen and stabilize the middle third of face and is considered the basis for attractive presentation since it establishes mid-facial breadth and emphasizes the cheeks. 2
The zygomatic bone articulates with the superior frontal bone, maxilla, temporal bone, and sphenoid bone on the back having five processes known as the zygomaticotemporal (ZT), zygomaticomaxillary (ZM), infra-orbital (IOR), fronto-zygomatic (FZ), and spheno-zygomatic (SZ) or zygomatic-sphenoid (ZS). 3
The ZM complex is a vital and intricate facial component that provides both vertical and horizontal struts to the facial framework. Due to its eminent location, it becomes susceptible to fractures, either alone or in conjunction with other bones.
ZMC fractures are the most frequent form of face fractures, coming in second only to nasal fractures in incidence. 3
Based on the category and seriousness of the damage, patterns of fracture range from uncomplicated to crunched and from slightly to substantially deranged. Zygomatic fracture is commonly called as “tripod fracture,” however it indeed entails interference at four different locations based on the crashing and intensity. 3
Because of changing fracture patterns caused by complicated traumas, it is impossible to apply established classifications for ZM complex fractures in a few situations.
Aesthetics has an crucial role in surgical design of patients with ZMC fractures. Keeping in mind the high aesthetic pertinence of mid-face,treatment of disrupted fragments should not give rise to scars or unaesthetic defects. It is critical to select the appropriate surgical approach, that adequately repairs fractured fragments and maintain the patient’s aesthetics. Because aesthetic restoration is frequently the primary or sole rationale for ZM complex fracture surgery, the method for treating these fractures must adhere to the same standards as aesthetic surgery. ZMC fractures should be treated as esthetic surgeries with minimum incisions and minimal hardware as they form the main esthetic zones of face. 5
The need for this study was to know how ZMC fractures treated at our center behaved in the long term in view of aesthetics and patient satisfaction. Evaluation of whether we were able to give satisfactory functional and esthetic results at our center to know if our present protocols are satisfactory or need further deliberation.
Distracted frontozygomatic suture in cases of tripod fracture, had highest percentage of signs or symptoms, while zygomatic arch fractures had the lowest. There occurs flattening of face in 89% of case of tripod fractures with displaced frontal-zygomatic sutures fragment. Trismus is most usually associated with a fracture of the zygomatic arch. Epistaxis and subconjunctival ecchymosis occurred in varying degrees, ranging from 20% in arch fractures of zygoma to 65% in zygomatic-orbital fractures. Functional impairments such as paraesthesia, trismus, diplopia, and anti mongoloid tilt are extremely distressing for the patient and necessitate surgical repair. 2
A computed imaging with reconstruction, Water’s view, and a submental-vertex projection distinctly detects the fracture and its movement. 3
Materials and Method
A retrospective analysis undertaken at Oral & Maxillofacial Surgery Department of KM Shah College from tenure, January 2015 to December 2021. The patients who reported with history of trauma of face were included. Approval was taken from Sumandeep Ethics Committee (SVIEC) with no. SVIEC/ON/DENT/SRP/22006.
Patient’s Informed consent was not required as this is a retrospective study.
Ages group of 18–61 years.
Displaced and non-fracture of the ZMC.
Fractures which have occurred less than 6 weeks before.
Concussion cases with extreme traumatic brain injury.
Orbital fractures, where secondary approach is necessary for restoration of inferior wall of orbit.
Fractures beyond 6 weeks.
Medically compromised cases.
Age and gender distribution.
Etiology of fracture.
Site of fracture and treatment done.
Ethics Approval
Sumandeep Vidyapeeth Institutional Ethics Committee (SVIEC). SVIEC/ON/DENT/SRP/MARCH/23/75.
Methodology
Medical records of all the patients with maxillofacial injuries was analysed. Data for analysis was acquired from the track record of patients given treatment at Dhiraj hospital, Vadodara from January 2015 to December 2021.
Documentation gathered was analysed for age, sex, process of injury, and fracture area of ZMC.
Patient data were diagnosed for fracture based on the documented history, clinical findings and complains, examining and interpreting radiographs.
Patters of fractures was identified taking into consideration fractured ZMC in relation to the different etiological factors. Causes were classified as RTA, falling from height, physical violence and injuries during sport activities.
Soft tissue wounds were not documented as associating injuries. To decide the treatment plan by examining the patient and before treatment 3DCT scans were done in all patients.
Patients were kept on follow up of 6 ± 2 months.
Statistical Analysis
Windows Statistical software SPSS 20 is used for studying data. Quantitative, statistical investigation was carried out by Chi-square and paired sample-t test. P-value of 0.05 was considered significant
Results
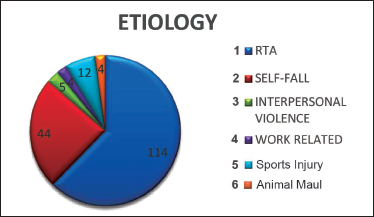
In course of period of six years study from January 2015 to December 2021 which also includes follow up period, 183 cases with ZM complex fracture were given treatment, with the mean age of 33 ± 14.5 years (Figure 1, Table 1) and with gender distribution of 68% (n=124) males and 32% (n=59) females (Figure 2, Table 2). In the community measured, RTA was considered to be a frequent etiology causing zygomatic fracture marked 62.3% (n=114), following which are unintentional self-falling, illustrating 24% (n=44) of instances, sports injury (n=12) 6.6%, physical attack (public violence) 2.7% (n=5), repetitive strain or industrial damage marked 2.2% (n=4) and animal maul damage (n=4) 2.2% (Figure 3, Table 3). Information on clinical demonstration was documented throughout the examination of the injured. Subjects featured with circumorbital ecchymosis, edema around the eye and hyposphagma were the frequent signs trailed by conjunctival swelling, cheek flattening, palpation of step. Investigation manifested that zygoma got fractured at only one protrusion in 53.6% (n=98) and multiple protrusion in 46.4% (n=85). In cases of only one protrusion fracture, maxillary-zygomatic buttress was frequently concerned attributing 27.3% (n=50), trailed by isolated zygomatic arch 15.3% (n=28), infraorbital rim (IOR) 9.3% (n=17) and frontal-zygomatic (FZ) 1.7% (n=3) (Figure 4, Table 4).
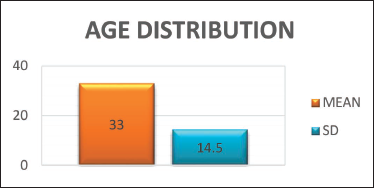
Results shows Mean Age is 33 ± 14.5.

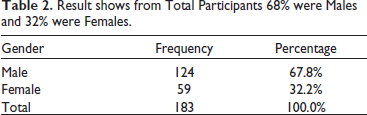
Result shows from Total Participants 68% were Males and 32% were Females.
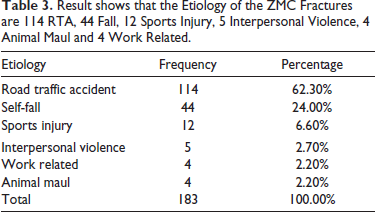
Result shows that the Etiology of the ZMC Fractures are 114 RTA, 44 Fall, 12 Sports Injury, 5 Interpersonal Violence, 4 Animal Maul and 4 Work Related.
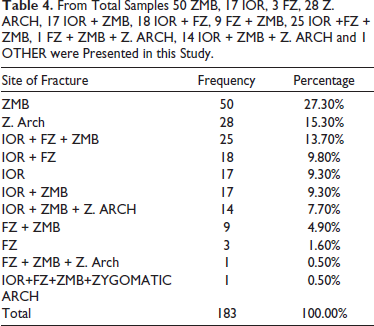
From Total Samples 50 ZMB, 17 IOR, 3 FZ, 28 Z. ARCH, 17 IOR + ZMB, 18 IOR + FZ, 9 FZ + ZMB, 25 IOR +FZ + ZMB, 1 FZ + ZMB + Z. ARCH, 14 IOR + ZMB + Z. ARCH and 1 OTHER were Presented in this Study.
Results shows Mean Age is 33±14.5.
Result Shows from Total Participants 68% were Males and 32% were Females.
Result Shows that the Etiology of the ZMC Fractures are 114 RTA, 44 Fall, 12 Sports Injury, 5 Interpersonal Violence, 4 Animal maul and 4 Work Related.
From Total Samples 50 ZMB, 17 IOR, 3 FZ, 28 Z. ARCH, 17 IOR + ZMB, 18 IOR + FZ, 9 FZ + ZMB, 25 IOR +FZ + ZMB, 1 FZ + ZMB + Z. ARCH, 14 IOR + ZMB + Z. ARCH and 1 OTHER were Presented in this Study.
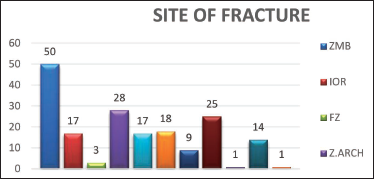
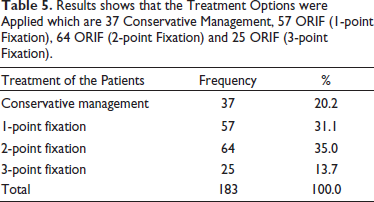
Fracture at two processes was found in 24% (n=44) where bone was fractured at multiple points. In patients with two process fracture IOR + FZ accounting for 9.7% (n=18), IOR + ZMB 9.3% (n=17) and FZ + ZMB 5% (n=9) respectively. Three process fractures (tripod) were reported in 21.9% (n = 40) of cases out of which most commonly involved was IOR + FZ + ZMB accounting for 13.7% (n = 25), followed by IOR + ZMB + Z. ARCH 7.7% (n = 14) and FZ + ZMB + Z. ARCH 0.5% (n = 1). 0.5% (n=1) cases associated buttress, rim of orbit, frontal-zygomatic suture and arch of zygoma. 20.2% of 183 patients were detected with undisplaced fracture were kept on follow up and treated conservatively. ORIF was carried in 79.8% (n=146) of patients. Incision like trans conjunctival, subcilliary, lateral brow, oro-mucosal, coronal and along existent tearing wound were used for exposing fracture site. Based on the intensity of the damage, degree of movement of fragments, compensation needed after reduction ,fragments were stabilized and fixed at single , double , triple point.. Fixing at single point was completed in 31.1% (n=57) of the instances; fixation at 2 point in 35% (n=64) of instances fixation at 3 points in 13.7% (n=25) of the instances (Figure 5, Table 5). During tenure of follow up, no patients were found with incidence of movable segments of fracture. Postoperative follow up evaluation such as edema and trismus were seen in few cases which settled a while later.
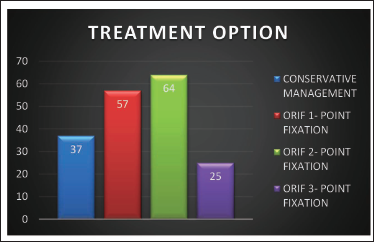
Results shows that the Treatment Options were Applied which are 37 Conservative Management, 57 ORIF (1-point Fixation), 64 ORIF (2-point Fixation) and 25 ORIF (3-point Fixation).
Results shows that the Treatment Options were Applied which are 37 Conservative Management, 57 ORIF (1-point Fixation), 64 ORIF (2-point Fixation) and 25 ORIF (3-point Fixation).
Discussion
The integrity of the zygoma is widely recognized as being crucial in maintaining normal width of face and cheek prominence. In mid-face fractures, three major buttresses must be considered. The medial buttress, also known as the naso-maxillary buttress, extends from the anterior alveolar bone of maxilla to the attachment of frontal bone of cranium. The posterior buttress, joins maxilla to sphenoidal bone antero-posteriorly. The next buttress is the zygomatico-maxillary, joining the lateral maxillary alveolar bone to the temporal bone of the zygomatic extension. Mihai Juncar et al in his cohort analysis of 2021 discussed evidence of more incidences of fracture in young age group due to fact that these groups often participate in social gatherings, leading to alcohol and drugs consumption scenario causing aggression and conflicts. 6
Dikhit PS et al. found a disparity in the population based on age and gender, with considerably more patients in the 19-39 year of age, than that of older population, being consistent with several different analysis. This demonstrated that younger age groups, particularly men, are substantially distinctly possible to sustain injuries resulting from their proclivity for high-velocity vehicles and interpersonal conflicts. 7
Mijiti et al in 2014 reported that monetary status, density of population and differences in culture have influence on causes of trauma. 8 Jingjing Mao et al in 2023 revealed that older patients are more likely to suffer to midfacial fracture as a fact of more developed and mature maxilla making it vulnerable to external blows. 9
In present study mean age was 33 ± 14.5 and of the total participants 68% were males and 32% were females.
According to a study by Rohit et al. (2.6:1), and other investigators like Ozemen et al. (3.2:1) and Chowdhury et al. (5.2:1) also reported comparable results. More men than women suffered zygomatic bone fractures. The third decade was the age range most frequently included in our investigation, which may be due to young adult males’ higher levels of social activity. Maximum source of malar bone fracture in the current investigation was a traffic collision, particularly two-wheeler motorbike accidents. 3
According to Ellis et al.’s study, motor vehicle accidents accounted for just 13.3% of the zygomatico-orbital fractures, which accounted for 46.6% of the sample overall. The Ellis et al. study found a low rate of motor vehicle accidents, which may be due to the law requiring the use of seat belts and other safety equipment. The current study’s high prevalence of zygoma fractures may be due to rise in count of vehicles and a lack of safety precautions. 1
In present study, the etiology of the ZMC fractures were 114 RTA, 44 falls, 12 sports injuries, 5 interpersonal violence, 4 animal maul, and 4 work-related. Sandeep Pandey et al explained positive outcomes in reducing accident rates on sensitizing general population regarding protective restraints and rules enforcing safe driving 10 In 2012 Rajay Kamath et al analyzed pattern of ZM complex fractures briefing about associated ophthalmic injuries like subconjunctival hemorrhage, optic neuropathy, diplopia, hyphema. 11
According to Rohit et al.’s study, lone zygomatic arch fractures occurred in 8.2% of instances and single process fractures occurred in 28.6% of patients. 5.1% of instances with lone and inwardly override zygomatic arch fractures had limited oral opening treated by raising the arch intraorally. 10.21% was found to be isolated fracture of IOR and 14.3% of buttress. In 63.2% of cases, there was more than one process fracture, of which 34.6% had two process fractures and 24.5% had three process fractures. 2 In study of Kathia Dubron et al described ION injury due to compression of bony fragments, oedema, hematoma and more severe nerve injury leading to paresthesia. 12
In present study from total samples, 27.4% zygomaticomaxillary buttress, 9.3% infraorbital rim, 1.6% frontozygomatic, 15.3% zygomatic arch, 24.1% two process fracture, 21.8% three process fracture and 0.5% more than three process are involved. Addressing ZM complex fracture is majorly significant as this bone affects contour of face, shielding globe of eye and for sensory perceptivity of cheek 11 Paul tent in his study on Romanian public related complexity of fracture with etiology, kinetic energy of harming agent, speed changes and collision effect on receiver. 13
Displaced zygomatic fractures must be properly reduced and fixed in order to promote appropriate healing and avoid complications after surgery. While only one, two or three of the four articulations must be treated intraoperatively in order to correctly decrease these fractured segments, it is not necessary to address all of them in order to achieve an acceptable reduction.
The writings describes multifarious treating approaches for managing zygomatic fractures, including advancement with hook, external pin fixation, antral dressing, and intra-osseous wiring. 3
Procedures like frontolateral wire suspension, transpalatal wiring and gillies temporal approach are to be performed whenever required. 11
All of the methods have benefits and drawbacks. Issues with the original osteosynthesis treatment of ZMC fractures included a deficit of directional control, aspects such as inadequate proximity area, excessive bone tightness, and secondary intent healing. The issue with wire osteosynthesis was solved by the development of miniature, pliable plates and screws for maxillofacial fracture fixation. 3
In the study conducted by Rohit et al., 83.7% of cases were given treatment of ORIF by utilizing micro plates. 3 Single-point fixation was performed in 22.9% of instances, with 14 requiring fixation at ZMB, 3 at IOR margin, and 5 at FZ. 2-point fixation was performed in 42.4% of instances, with 24 in the frontal-zygoma and buttress region, 8 in orbital rim and zygomatic-frontal region and 10 in the IOR and ZMB region. Fixation at triple point was performed on 15 individuals (18.4 %). The intensity of displacement determined the different points of fixation in this investigation. 3
Ellis et al. documented that 23% of 2067 ZM complex fractures did not go under any surgical procedure. 1
In the present study, results show that the treatment options applied are 37 conservative management (20.2%), 57 ORIF (1- point fixation) (31.1%), 64 ORIF (2-point fixation) (35 %) and 25 ORIF (3- point fixation) (13.7%). 14
Conclusion
Different therapeutic strategies for managing ZM complex fractures start with precise and prompt diagnosing taking into account the correct reduction of fractured fragments to attain equilibrium of face. In this study, male predilection to ZMC fractures was seen, RTA being the most common etiology and repeated site of fracture being buttress of ZMC. In perspective of treatment, fixation at two point was found to be 35% which is most common. We have experienced that a number of techniques can be performed favourably to fix ZM complex fractures, which are based on the features of fracture but the most reliable method for achieving three-dimensional stability is ORIF with miniplates.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Retrospective Analysis of Trends of Zygomaticomaxillary Complex Fractures in Patients Reporting to a Tertiary Health Center—Our Experience by Dharang Soni, Amit Mahajan, Pratesh Dholabhai and Krishna Panchal, in The Traumaxilla
Footnotes
Acknowledgement
Authors would thank Dr. Gulam Naviwala for valuable insights on the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.