
Abstract
Hemangiomas are benign tumors of endothelial cells and most common tumors of the childhood but rarely found in adults. They appear a few weeks after birth and grow rapidly, and in most cases undergo involution. Hemangiomas occur more common in females than males. The treatment depends upon patient’s age, lesion location, size, and evolution stage. Here, we report a rare case of cavernous hemangioma in a 44-year-old male present on right lateral border of anterior two-thirds of tongue.
Introduction
Vascular anomalies are a group of conditions characterized by the abnormal development of blood or lymphatic vessels. Mulliken and Glowacki (1982) divided the anomalies into 2 main categories, hemangioma and vascular malformation, based on the clinical presentation, biological behavior, and histology of the lesion. The International Society for the Study of Vascular Anomalies approved the scheme in 1996, and it was later revised in 1997. It is now universally accepted as the official classification system for vascular anomalies worldwide.1, 2
Hemangiomas are benign neoplasms made up of rapidly proliferating endothelial cells. These cells are surrounded by hyperplastic cells, and the blood vessel structure is not complete. In contrast, vascular malformations do not have hyperplastic cells but are characterized by abnormal and dilated vessels that enlarge progressively. The vessels are composed of a specific vascular architecture such as veins, lymphatic vessels, venules, capillaries, arteries, or a combination of these types. 2
Hemangiomas are the most common tumors in childhood and are rarely found in adults. Typically, these growths become apparent a few weeks after birth and exhibit rapid growth, but in most cases, they eventually undergo regression or involution.2, 3 Histologically, they can be classified into “capillary,” “cavernous,” and “mixed” types.1-9 Different treatment modalities are available such as intralesional and systemic corticosteroids, sclerosing agents, embolization, excision, electrolysis, thermocautery, and laser photocoagulation. 2
This case report presents a rare case of cavernous hemangioma located on the right lateral border of the anterior two-thirds of the tongue in an adult male patient.
Case Report
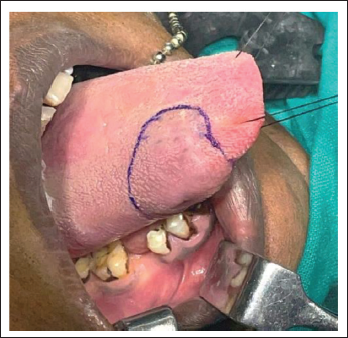
A 44-year-old male came in with a swelling in his mouth involving the right lateral border of the anterior two-thirds of the tongue (Figures 1a and 1b) that had been present for the past 10 years. History of the present illness revealed that the swelling was initially small in size but gradually increased over time to reach its current size. Throughout this period, there were no associated symptoms such as pain, difficulty in speech, swallowing, and mastication. There was no significant medical, dental, or family history to report. On general examination, the patient was normally built and all the vital signs were under the normal limit.
Lesion on the Right Lateral Border of Anterior Two-Third of the Tongue.

On intraoral examination, there was a dome-shaped, bluish-purple swelling on the right lateral surface of the anterior two-thirds of the tongue with normal surrounding mucosa, measuring about 3cm×3cm in its greatest dimension. The borders were well-defined with central scarring of the lesion. Upon palpation, the lesion was found to be soft and non-pulsatile, exhibiting emptying and refilling phenomena, and it demonstrated blanching when pressure was applied. A provisional diagnosis of hemangioma of the tongue was made based on the clinical findings.
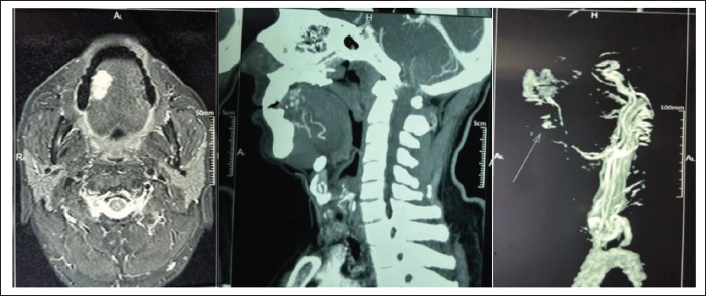
Contrast-Enhanced Magnetic Resonance Imaging (CE-MRI) angiography was done which revealed a well-defined lobulated avidly enhancing soft tissue lesion (measuring 22×15×25 mm) epicenter in the dorsum of anterior two-thirds of the right lateral border of the tongue supplied by right lingual artery (Figures 2a, 2b, 2c). Wide surgical excision of the lesion with primary closure of the defect under general anesthesia was planned.
CE-MRI of face and neck revealed a well-defined lobulated avidly enhancing soft tissue lesion (measuring 22×15×25 mm) epicentered in dorsum of anterior 2/3rd of right lateral border of tongue supplied by the right sublingual artery (axial view and sagittal view).
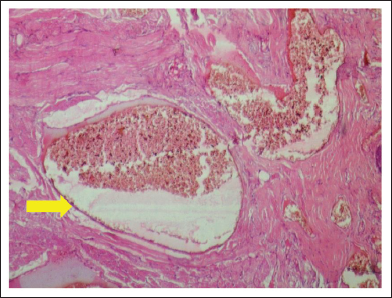
Written consent was obtained from the patient. A routine blood examination was done which was found to be within normal limits. After completion of the pre-anesthetic check-up patient was posted for general anesthesia. Initially, 2 sutures were tied at the tip of the tongue to retract and prevent fallback during the procedure. The incision site was marked using a surgical marker (Figure 3). Surgical excision of the lesion was carried out using electrocautery (Figure 4). Before the complete surgical excision, the feeder’s vessel was identified and ligated followed by suturing of the tongue (Figure 5). After the specimen was removed, it was sent for histopathological examination, which confirmed the diagnosis of cavernous hemangioma (Figure 6). Postoperatively, tongue movements were normal. On initial follow-up days, the patient’s phonetics were affected which improved later on further follow-up days. There were no complications during the healing process, and complete recovery was observed after 1 month, with no recurrence of a similar lesion (Figure 7). The patient is under regular follow-up.
Marking of the Incision Site.
Excision of the Lesion.

Primary Closure of the Defect.

Photomicrograph (H and E×40) revealing cavernous hemangioma. Note the dilated blood vessels with hyperplastic cells at the periphery of the endothelial lining.
Complete healing of the lesion with no recurrence.

Discussion
Hemangiomas are classified as benign tumors and are characterized by 3 stages: endothelial cell proliferation, rapid growth, and spontaneous involution. The appearance of hemangiomas is attributed to both genetic and cellular factors, with monocytes being considered potential ancestors of hemangioma endothelial cells. These lesions are a result of an imbalance in angiogenesis, causing uncontrolled proliferation of vascular elements. This proliferation is associated with substances such as vascular endothelial growth factor, basic fibroblast growth factor, and indole-amine 2,3-dioxygenase, which are found in large amounts during the proliferative stages, but reduce throughout the involution stage.5, 9
Hemangiomas are the most common soft tissue tumors of the head and neck in childhood. These tumors completely resolve in 50% of children by 5 years of age, 70% by 7 years, and 90% by 9 years. However, the occurrence of hemangiomas in adults is rare. 2 In adults, hemangiomas are commonly of the cavernous type and show no spontaneous regression while infantile hemangiomas are usually capillary. According to Chaung et al, more than 90% of cases present before the fourth decade of life 6 , and hemangiomas occur more frequently in females than in males, with a ratio of 3:1.2, 7 However, in contrast to this, the present case shows a different pattern.
As the present case involves an adult male in the fourth decade of life, which is atypical for the typical presentation of hemangiomas, it warrants further consideration.
Clinically, hemangiomas are characterized as soft, smooth, or lobulated tumors that may be sessile or pedunculated and can vary in size from a few millimeters to several centimeters. The color of the lesion typically ranges from pink to red-purple and the tumor blanches on the application of pressure. Hemorrhage may occur either spontaneously or after minor trauma.2, 3 Regarding the location and number of lesions, similarities with cases reported in the literature were observed, as 80% of patients present a single lesion and the head and neck region is the most commonly affected. 8
Depending upon the size and location, significant impairment can result from the growth of problematic hemangioma. In the present case, where the lesion was present on the tongue, special consideration is required due to the tongue being a mobile and inquisitive organ, which increases the susceptibility to minor trauma and consequent bleeding and ulceration. While cosmetic concerns are the major concern in most cases, 3 if the lesion is large, it may also cause difficulties in swallowing, and breathing problems, and interfere with mastication.
To diagnose hemangiomas, bidigital palpation of the affected region to detect the disappearance of blood flow due to finger pressure, followed by observation of revascularization after removal of finger pressure, are important diagnostic signs. Furthermore, if the lesion has an arterial origin, a pulse can be obtained by finger pressure. 3
Radiological investigations are mainly done if the tumor is compressing a vital anatomical structure like a nerve or a vessel. Computed tomography (CT) and magnetic resonance imaging (MRI) are commonly used for assessing the volume of hemangiomas and vascular malformations. These imaging modalities can also help to differentiate the tumor from other possible conditions and assist in determining the size, extension, and location of the lesion. Furthermore, CT and MRI are useful for follow-up assessments after treatment. Color doppler test can help in differentiating between vascular and nonvascular lesions and can help to localize the feeding vessel, further helping in concluding the treatment plan. 5
Histologically, the cavernous variant of hemangiomas, as seen in this case, is composed of dilated, thin-walled capillaries that have one layer of endothelial lining and a variable layer of fibrous adventitia. The walls of these vascular caverns do not contain elastic fibers. On pathological examination, there is typically evidence of previous hemorrhage. Thrombosis may also be present within some of the lumens. 8
Conservative observation has traditionally been used to allow most lesions, especially those in inconspicuous locations, to resolve on their own. Nowadays, it is recommended to intervene early for aesthetic reasons, especially if they are in visible areas. In some instances, medical or surgical interventions may be required if the hemangioma results in functional difficulties, ulceration, bleeding, or if it is exceptionally large. There are rare cases where hemangiomas can lead to congestive heart failure. The treatment options include intralesional and systemic corticosteroids, beta-blockers, instillation of sclerosing agents, irradiation, embolization, laser therapy, cryotherapy, and surgery. The most effective treatment is a wide surgical excision. 2 Close follow-up is necessary regardless of the treatment chosen.
Conclusion
The case presented here is that of an adult male patient with a cavernous hemangioma located on the right lateral surface of the anterior two-thirds of the tongue, which is a rare occurrence. While most hemangiomas typically undergo spontaneous involution, their growth can result in significant impairment depending on their size and location. Early intervention should be considered to avoid sequelae. Based on our findings and available literature, we suggest that surgical excision is the preferred treatment option for vascular lesions affecting the tongue.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Before commencing the study, ethical clearances were obtained and informed consent was obtained from all participants as deemed necessary.