
Abstract
Background:
The mandibular condylar fracture is second most frequent maxillofacial fracture but still the management remains controversial.
Aim:
The purpose of the present study is to evaluate the clinical as well as radiographic outcomes of different types of management modalities in various mandibular condyle fractures during 6 months of follow-up.
Material and Method:
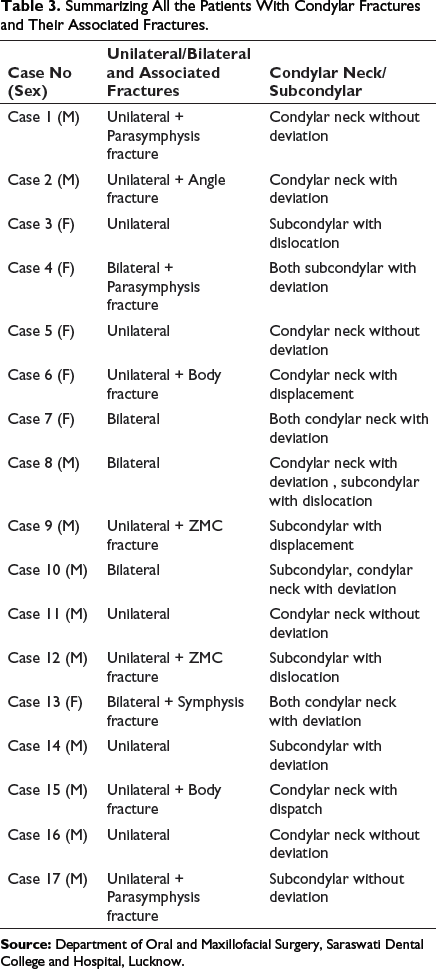
This retrospective study consisted of 17 patients of which 11 were male (65%) and 6 female (35%). These included 12 unilateral condylar fractures (70%) and 5 bilateral fractures (30%). Anatomically, these fractures were 13 condylar neck fractures (59%) while 9 were subcondylar fractures (41%). Depending on the anatomic position, type, displacement/dislocation/deviation of condyle, and associated fractures, 5 closed reduction (23%) and 17 open reduction and internal fixations (77%) were performed. Fixation was done with lag screw in 1 patient, 3-D strut plate in 2 patients, and single miniplate fixations in 14 patients. Orthopantomograms were taken preoperatively, immediate postoperatively, and at 1, 3, and 6 months postoperatively to evaluate the radiographic changes.
Results:
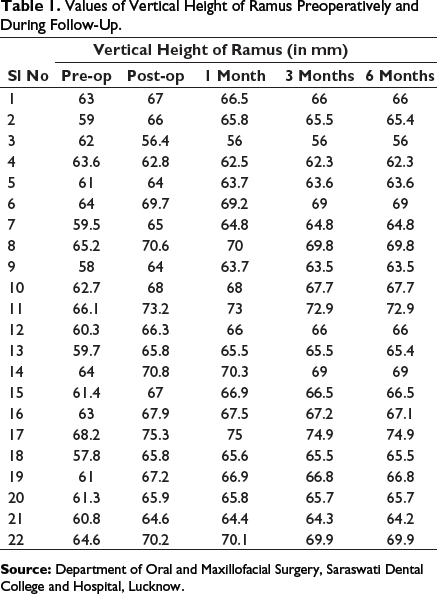
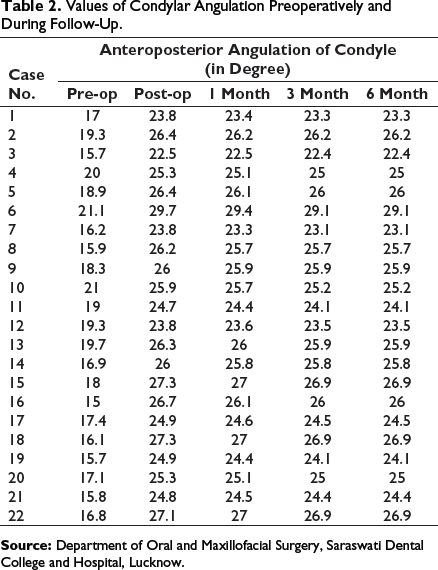
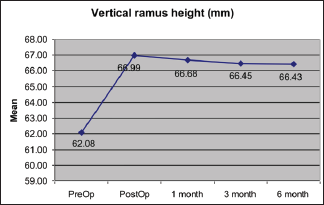
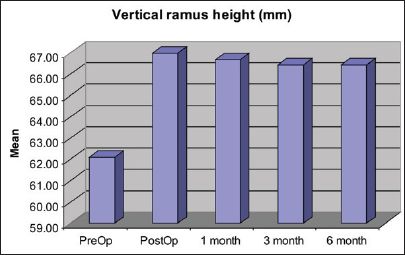
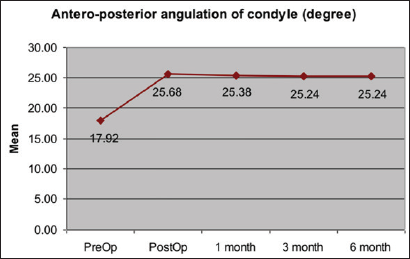
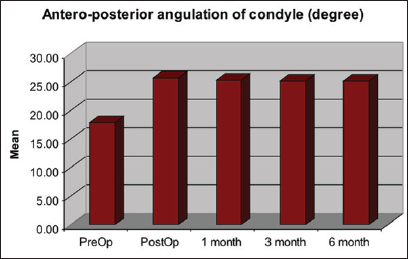
Preoperatively, the average ramus height was 62.07 ± 4.13 (in mm) while condylar angulation was 18.23 ± 4.38 (in degree) while immediate postoperatively these were 66.98 ± 5.03 (in mm) and 25.67 ± 4.07 (in degree), respectively. After 6 months, the value was 66.43 ± 4.97 (in mm) and 25.24 ± 3.94 (in degree) which is statistically significant (P < .5).
Conclusion:
Open reduction and internal fixation allows better maintenance in function and anatomical repositioning of condyle as compared to closed reduction.
Keywords
Introduction
The mandible is the only mobile bone of the maxillofacial region. It forms the lower third of the face. Fractures of the mandible are the most common fractures that a maxillofacial surgeon comes across. Fractures of mandibular condyles account for 25% to 45% of all the mandibular fractures1, 2 and 72% times it is associated with fractures of other facial bones. 3 Isolated condylar fractures are rare, and occurrence of malocclusion is more dependent on the site of fracture. Incidence of condylar head fracture is the least with the majority fractures at the condylar base. Frequency of unilateral fractures is higher than the bilateral fractures.4-6 Although the incidence is high, till date the management remains an ongoing matter of controversy in maxillofacial surgery which is well reflected in the variety of opinions and treatment modalities proposed. Both conservative and surgical managements can be done according to the patients age, site of fracture, and other associated fractures. Conservative method is less invasive, safe, easy, and low cost with no surgical complications. Although closed management gives a satisfactory outcome, it is related to certain chronic problems like pain, arthritis, malocclusion, deviation in mandible on opening and closing, temporomandibular joint (TMJ) dysfunction, especially in bilateral condylar fractures. 7 If condyle is displaced by 10 to 45 degree or shortening of ramus height is by 2 mm, surgical management is preferable. Surgical treatment also has disadvantages such as its high cost, scar formation, intraoperative hemorrhage, and facial nerve injury. The main goal is to achieve (a) no pain with minimum interincisal distance of 40 mm, (b) smooth movements on excursions, (c) restore preinjury occlusion, (d) good stable TMJs, and (e) good symmetry of face and jaw. 8
Aim and Objectives
The aim of the study is to evaluate the outcomes of different types of management modalities in various condylar fractures treated at Saraswati Dental College and Hospital in last 3 years (January 2018-December 2020). The objective of the study is to evaluate the changes in the vertical height of ramus and anteroposterior angulation of condyle radiographically in OPG.
Materials and Methods
Values of Vertical Height of Ramus Preoperatively and During Follow-Up.
Values of Condylar Angulation Preoperatively and During Follow-Up.
Summarizing All the Patients With Condylar Fractures and Their Associated Fractures.
Preoperatively, detailed case history of the patients was recorded and thorough clinical evaluation of fracture sites was done to detect presence of edema, ecchymosis, hemorrhage, derangement of occlusion, step deformities, and fracture segment mobility. Radiographic evaluation was done through OPG.
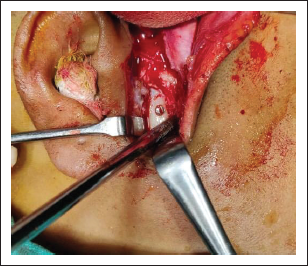
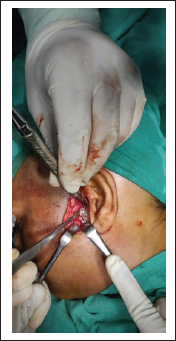
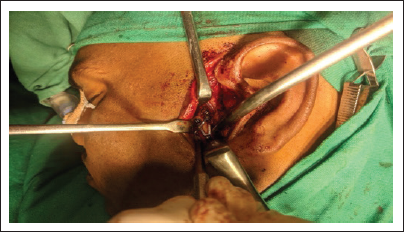
The type of management was chosen based on fracture type, location, position, associated fractures, location of the fracture, amount of vertical reduction in height of the ramus and degree of angulation, relation of condylar head to the glenoid fossa, TMJ and mandibular functions with occlusion status. In 5 patients closed reduction (23%) and in 17 patients open reduction internal fixations (ORIFs) (77%) was performed.10-12 In closed reduction, intermaxillary fixation (IMF) was done for 2 to 6 weeks with functional treatment and functional exercises. 13 The surgeries were performed under general anesthesia with nasal intubation. In ORIFs prior to the surgery, IMF was done to provide proper occlusion before the fracture reduction and fixation. In order to expose the fracture site, submandibular approach14, 15/retromandibular approach16, 17/preauricular approach 18 /Alkayat Bramley approach 19 was taken. Lag screw was used in 1 fracture reduction (Figures 1 and 6), 3-D strut plate in 2 patients (Figure 3), and single miniplate fixations in 14 fractures (Figures 2 and 7). After proper reduction and stability of internal fixation, IMF was removed. Wound closure was done in layers.
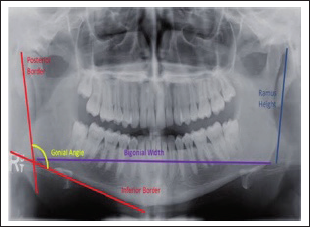

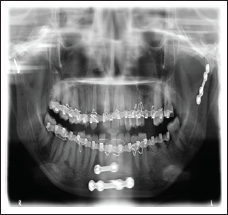
Clinical follow-up was carried out in all patients. OPGs analyzed preoperatively, immediate post-operatively, after 1, 3, and 6 months postoperatively. Mandibular ramus height and condylar angulation were investigated by the condylar morphology scale (CMS) method for observation of condylar remodeling or resorption. Condyle process shortening was measured, and the fractured side of the condylar process was compared with the healthy side. Ramus height was also compared before and after the time the fracture was surgically reduced. In cases of bilateral fracture, the overlay of fragments was measured on X-ray. 22 All measurements were taken by the same investigator (Figures 4 and 5). This was also helpful to detect any cases of nonunion, plate fracture, loosening of plate and screws, and for measuring the bone density in fracture line.
Result
Preoperatively, the average ramus height is 62.07 ± 4.13 (in mm) and condylar angulation is 17.92 ± 3.38 (in degree). Statistical analysis showed that immediate postoperatively the ramus height is 66.98 ± 5.03 (in mm) and the condylar angulation is 25.67 ± 4.07 (in degree) while after 6 months the value is 66.43 ± 4.97 (in mm) and 25.24 ± 3.94 (in degree) respectively (Figures 8 to 11).
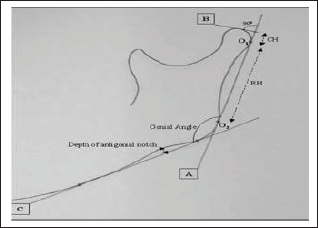
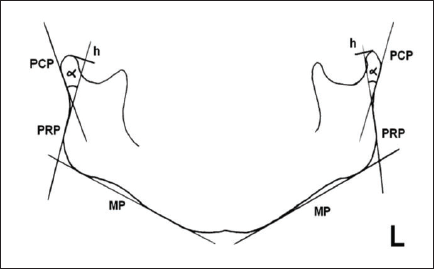
OPG tracing after surgical treatment of a simple condylar fracture and symphyseal fracture. Bilateral measurement of ramus height and anteroposterior condylar angulation. h right = 83 mm, h left = 83 mm; α right = 23 degree, α left = 25 degree; MP: mandibular plane; PRP: posterior ramus plane; PCP: posterior condyle plane; a: angle between PCP in PRP, that is, between the condyle and ramus; h: total ramus height e measured from the intersection between PRP with MP to top of condylar head.
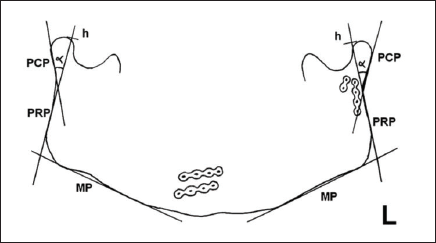
OPG tracing after conservative treatment of a simple condylar fracture. Bilateral measurement of ramus height and antero-posterior condylar angulation. h right = 59 mm, h left = 65 mm; α right = 34 degree, α left = 28 degree; MP: mandibular plane; PRP: posterior ramus plane; PCP: posterior condyle plane; a: angle between PCP in PRP, that is, between the condyle and ramus; h: total ramus height e measured from the intersection between PRP with MP to top of condylar head.
Discussion
In this study, gender distribution shows clear predominance of males. Again the ratio of additional fractures is more as compared to isolated condylar fracture. 23
All 22 fractures were managed with 4 different treatment modalities to manage the mandibular condylar fractures.
In conservative management, IMF was done for 2 to 6 weeks. IMF was obtained by using arch bars, Ivy loops, and IMF screws used depending on the use of elastics or wires, and on the level of fracture. During this, functional treatment was followed with guiding elastics and active movements. Elastics are given to achieve repeatable occlusion. Initially, heavy elastics are placed and then slowly shifted to light elastics. In ORIFs, early intervention gave better improvements. In case of associated fractures, the duration was longer till traumatic swelling subsided. 24 Fixation with titanium plates and screws allowed good osteosynthesis and has given optimal results with adequate bone, proper site selection, and proper techniques. 25
Patients were followed up to 6 months postoperatively. All showed good results in mandibular functional parameters and fracture alignment with significant increase in bone density. No patient reported with nonunion, plate fracture, or loosening of plate or deviation in condyle. Better mandibular movement and better subjective outcomes, such as regarding pain and malocclusion, can be expected with open treatment.
Increase in ramus height after reduction was radiographically observed and statistically analyzed with the student t test; also, a significant difference was found between the preoperative and postoperative positions of the condyle (P < .05). The fact that height was constant at the control OPGs shows that no resorption occurred during the study period. Remodeling of the condyle (CMS score, 1) was observed in patients, but this fact was not clinically or statistically significant because remodeling of the condyle was minimal and did not affect ramus height. 26
Conclusion
Both treatment options for condylar fractures of the mandible yielded acceptable results. However, operative treatment was superior in all objective and subjective functional parameters except occlusion. Open reduction and internal fixation with ORIFs allows better maintenance in anatomical repositioning and condylar function as compared to closed reduction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.