
Abstract
The temporomandibular joint is the joint formed by the glenoid fossa of the temporal bone and the condylar process of the mandible. It is covered by dense fibrocartilage called the capsule. Each mandibular condyle has a wide motion range, consisting of both rotation and translation. Temporomandibular joint arthroscopy is a technique for direct visual inspection of internal joint structures, including biopsy and other surgical procedures performed under visual control with the help of an arthroscope. In this review article, the authors try to address the techniques of arthroscopy and its recent advances.
Introduction
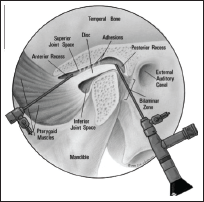
The temporomandibular joint (TMJ) is the joint formed by the glenoid fossa of the temporal bone and the condylar process of the mandible. It is covered by dense fibrocartilage called capsule. Each mandibular condyle has a wide motion range, consisting of both rotation and translation. The fibro-cartilaginous disc cushions mechanical stresses that exist between the temporal and mandibular articular surfaces. The high collagen content of this disc provides great rigidity and durability. The TMJ disc has no direct vascularization or innervation by itself. However, its posterior attachment, known as retrodiscal tissue, features many vessels and nerves which are crucial during physio-pathological processes. The TMJ has a more complicated anatomy and function than any other human joint.
TMJ Arthroscopy
TMJ arthroscopy is a technique for direct visual inspection of internal joint structures, including biopsy and other surgical procedures performed under visual control with the help of an arthroscope. Arthroscopy of the TMJ has been established as a reliable and predictable, noninvasive technique for the treatment of internal derangement (ID) of the TMJ, mainly for Wilkes 1 stages II, III, and IV. 2
Kondoh et al 3 in a cadaver study of 30 joints, found that morphologic changes in the inferior surface of the TMJ disk were more prevalent than those in the upper surface, although no relationship between irregularities of the inferior surface and the position of the disk was found.
Milam and Schmitz 4 reviewed the rationale and role of molecular pathological sequences in the synovial fluid of diseased TMJ, and hypothesized and proposed several pathways.
Some studies5–14 demonstrated that various cytokines, pain mediators, and substances detected were higher in diseased TMJ compared with the control and were closely linked to the pain and/or osteoarthritic changes.
Montgomery et al 15 reported the clinical and radiographic results of arthroscopy in 52 joints. Patients were studied at 1, 2, 4, 8, 24, and 52 weeks postoperatively. The authors found that pain, mandibular movement, function, and diet were significantly improved. The incidence of joint sounds did not significantly improve beyond the week’s evaluation. Arthroscopy is a reliable and safe procedure for decreasing pain and increasing mouth opening in patients with ID, independently of the grade of involvement of the joint surface and the synovial lining. 16
TMJ arthroscopy is of 2 types.
Historical Background
Arthroscopy of the human TMJ was first described by Ohnishi in 1975. 16 A major breakthrough for small joint endoscopic access occurred in 1970 with the development of the Watanabe no. 24 Selfoc arthroscope with a 1.7-mm diameter. 17 This was introduced into the TMJ by Masatoshi Ohnishi using a fiberoptic light source and arthroscopic device manufactured by Olympus in the early 1970s. Ohnishi published both the puncture technique and the anatomic findings, and later went on to describe the usefulness of this technique for clinical applications in the treatment of TMJ disease in 1980, including photographic documentation of normal anatomy, as well as providing early information on traumatic pathology and joint fibrosis.18-21 In 1978, an animal study on rabbits by Hilsabech and Laskin demonstrated that TMJ arthroscopy was a safe technique that revealed the appearance of intra-articular structures. 22
In 1982, Ken-Ischiro Murakami and Kazumasa Hoshino reported their procedural terminology and arthroscopic anatomy, excellently illustrating the human TMJ with color photography. 23 The first international hands-on course using fresh cadaveric specimens for technique development was initiated by J. J. Moses in late 1985.
In 1985, with references to the arthroscopic observations, Murakami and Hoshino described histologic cellular characteristics of the inner surfaces of the TMJ. 24 Holmlund and Hellsing in 1985 published their landmark paper on the concept of reproducible puncture sites correlating measurements along the tragal-canthal line. 25
A pivotal work was published in 1987 by Sanders in the treatment of closed lock condition with the surgical application of arthroscopic lysis and lavage over a 2-year period. 26
General Principles
In any arthroscopic surgical procedure involving small joints, it is important to adhere to some basic technical points:
The joint should remain fully distended, allowing for easier trocar puncture and minimizing the risk of iatrogenic intracapsular damage. The skin should be punctured with a sharp trocar. All intra-articular procedures should be done with care to prevent articular surface damage. Attention should be given to preserve as much healthy synovium as possible in order to enhance its physiologic effects on the joint in any arthroscopic surgical procedure. The joint space should be kept expanded during instrumentation by a slow infusion irrigation system.
Indications of TMJ Arthroscopy
Patients with pain and jaw dysfunction not responsive to nonsurgical dental/medical management.
Frequent mandibular dislocation
Persistent preauricular atypical facial pain.
Osteoarthritis
Post-traumatic complaints
Pseudotumors
Biopsy of suspected lesions or disease.
Confirmation of other diagnostic findings that could warrant surgical intervention.
Unexplained persistent TMJ pain that is nonresponsive to medical therapy.
Contraindications
Bony and advanced fibrous ankyloses
Ankylosing osteoarthritis
Malignant tumors
Advanced resorption of the glenoid fossa
Increased risk for hemorrhage: May cause hemearthrosis.
Overlying skin infection: Puncturing through an infected skin can cause septic joint postoperatively.
Armamentarium
Arthroscope
An arthroscope is a rigid cylinder with internally mounted lenses, which permits a view with a wider and brighter field.
It should be less than 2 mm in diameter with an angle of view of 30.
A 1.9-mm arthroscope with (a) C-mount attachment, (b) focusing ring, and (c) light source attachment. Following are the parts of an Arthroscope:
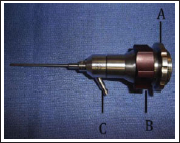
The devices inserted in the cannula, including the scope, should have a diameter at least 0.1 mm smaller than the inner diameter of the cannula.
Markings on the cannulas allows the surgeon to monitor depth of penetration
Technique for TMJ Arthroscopy
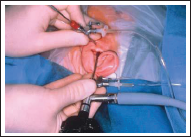
General anesthesia-nasotracheal TMJ is approached through 2 trocars. The arthroscope is introduced through 1 port, which also acts as the irrigation port. The second one is for drainage and instrument passage.
TMJ is inspected and palpated, and the position of condylar head is determined by passive movement of the joint.
Planning of Trocar Sites
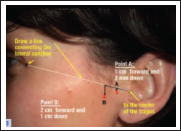
Draw a straight line between the center of the tragus and the lateral canthus. Mark a point on the line 10 mm from the tragus and 2 mm below it. Point A is the first trocar site. For the second trocar site, mark a point on the line 20 mm from the tragus and draw a perpendicular 10 mm down. This is Point B.
For distension of the superior compartment and in order to avoid iatrogenic damage to the cartilaginous surfaces during introduction of the trocar, 1% lidocain solution 2.0 mL is inserted.
The needle is aimed in a medial and slightly anteriosuperior direction until contact with the glenoid fossa is achieved.


Joint Puncture
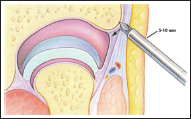
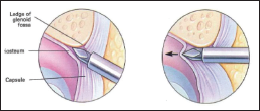
Through the small skin incision at the injection site, the lateral capsule is punctured with a sharp trocar in an arthroscopic sheath inserted in the same direction as the previous injection needle. The instrument is never to be passed straight through the capsule without locating the bone.
The cannula and trocar are advanced to the inferolateral aspect of the zygoma, then inferiorly stepped off the osseous ledge. The sharp trocar is exchanged for a blunt one, and the arthroscopic sheath is advanced further into the upper joint space. Correct placement can be checked by infusing saline-fluid level in the cannula that will move with the movement of jaw. Then the arthroscope is introduced with attached camera.
A second cannula is introduced in a similar fashion at point B. A second puncture into the joint space allows the clinician to establish an outflow of irrigation fluid to insert a probe to assist in the examination or to insert a cutting instrument to perform surgery. The second cannula should be placed at the anterior and lateral corner of the superior joint space to ensure maximum flexibility of the operative cannula.
The examination begins with the identification of landmarks—the boundary between the disk and posterior disk attachment, the medial capsule, and the inferior part of eminence and anterior capsule. The posterior disk attachment is the predominant location for inflammation like the increased vascularity capillary hyperemia, synovial hyperplasia.
Loss of well-defined boundary between posterior part of the disk and posterior disk attachment indicates degenerative changes usually found in joints with chronic locking and osteoarthritis. During alternate opening and closing movements, any elongation of the posterior disk attachment is revealed. The arthroscope should be moved more medially to visualize the medial capsule.
Arthroscopically, a clinician can evaluate and describe pathologies such as perforation, adhesion (fibrous connective tissue bands between disk and fossa), foreign bodies, hyperemia, corrugations (foldings), depression, fibrillations, and folds.
Arthroscopic Approaches
There are various approaches described for TMJ arthroscopy.
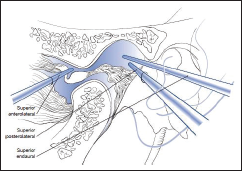
Superior posterolateral approach
Inferior posterolateral approach
Superior anterolateral approach
Inferior anterolateral approach
Endaural approach
Superior Posterolateral Approach
In this technique, the mandible is distracted downward and forward, producing a triangular depression in the front of the tragus. 27 This depression represents an area bordered superiorly by the glenoid fossa, anteroinferiorly by the dorsal aspect of the condylar head, and posteriorly by the external auditory canal. It is at the roof of this depression, above the gloved fingernail of the surgeon’s digit outlining the inferior aspect of the glenoid fossa, that the trocar is inserted.
The trocar is directed anterosuperiorly toward the posterior slope of the eminentia. This provides access to the posterosuperior joint space and allows visualization of the superior joint space. The areas that are difficult to visualize are the superoanterior synovial pouch and the medial paradiskal synovial groove.
Inferior Posterolateral Approach
This is a variation of the inferolateral approach, in that the trocar is directed against the lateral posterior surface of the mandibular head. The inferoposterior synovial pouch and posterior condylar surface can then be examined.
Superior Anterolateral Approach
In this technique, the trocar is directed superiorly, posteriorly, and medially along the inferior slope of the articular eminence after first locating the prominence of the lateral articular tubercle as a landmark.
The mandibular condyle is distracted inferiorly and positioned posteriorly by the surgical assistant. This approach allows anterosuperior joint compartment instrumentation or visualization.

Inferior Anterolateral Approach
This is a technically more difficult approach than those described earlier, and it allows observation of the lower anterior synovial pouch.
In this technique, the condylar head and articular tubercle are palpated. The trocar is then inserted at a point anterior to the lateral pole of the condylar head and immediately below the articular tubercle. This places the trocar in the lower anterior synovial pouch, adjacent to the anterior aspect of the condylar head. The technique allows observation of the lower anterior synovial pouch.
Endaural Approach
Steps of Endaural Approach
Injection of Heparinized Ringer’s Lactate to distend joint.
Placement of outflow needle in anterolateral aspect of the joint.
Arthroscopic examination of the joint via inferolateral approach.
This access is initiated by a trocar entering the posterosuperior joint space from a point 1- to 1.5-cm medial to the lateral edge of the tragus through the anterior wall of the external auditory meatus.
The trocar is directed in an anterosuperior and a slightly medial direction toward the posterior slope of the eminentia. This approach provides access and visualization of the posterior superior joint space as well as the medial and lateral paradiskal troughs.
Complications
Infection
Vascular injury
Discussion
Arthroscopy has become a common treatment modality for a variety of TMJ abnormalities. Patients for who conservative measures of treating temporomandibular disorders (TMDs) are not effective arthroscopy is a minimally invasive surgical procedure that has been shown to result in a satisfactory outcome, with no need to resort to open joint surgery. Pathologies of the TMJ and its associated muscles of mastication are termed as TMDs. TMDs present with a variety of symptoms that include pain in the joint and the surrounding musculature, jaw clicking, limited mouth opening, and headaches. TMDs form the most common noninfective, painful conditions of the orofacial region. If there is clear evidence of advanced degenerative joint disease, it is expected that arthroscopy will be less successful
Over the past decade, numerous researchers have shown the effectiveness of TMJ arthroscopy, both in the diagnosis and the surgical management of TMJ articulopathies.28-33
TMJ arthroscopy is effective in reducing pain and increasing motion in patients with ID.
It is a procedure that provides knowledge of how to treat dysfunction of the TMJ, and its complexity lies in the technique because the TMJ has a volume of just 0.9 mL in the inferior joint space and 1.2 mL in the superior.
Since 1975, arthroscopy of TMJ has been applied to clinical use primarily as a diagnostic procedure followed by minimally invasive surgical intervention. Basic investigations of TMJ arthroscopy and related surgery significantly inspire the progression of the diagnostic science through the findings of intra-articular pathology and by the cumulated data of synovial fluid analysis. Both arthroscopic surgery and arthrocentesis with lavage are now established as minimum invasive interventions for TMJ diseases.
Successful management of patients with TMJ pathology requires greater emphasis on the reduction of joint loading, inflammation, and pain, thus enabling maximizing joint mobility, and less emphasis on the restoration of anatomic relationships.
The basic principles of TMJ arthroscopic surgery require preservation of (a) synovial membrane for providing joint lubrication, (b) articular cartilage to maintain the properties of resiliency and compressibility, (c) the disc for giving a biomechanical advantage and hydrostatic/weeping lubrication, (d) intra-articular biopsy for histologic review, and (e) removal of adhesions and impediments to joint motion.
In 1995, Trumpy and Lyberg 34 stated the importance of functioning disc in the TMJ. They observed that the development of osteoarthrosis was significantly higher in the group with discectomy with or without disc substitute than in the discoplasty group.
It has been reported that most of the disruptions of the synovial lining have been reported to occur in the upper compartment, as was suggested by Holmund et al.
Arthroscopy of the inferior joint space requires only minor modification of the technique used for the superior joint space. The mandible is protruded as far anteriorly as possible, with the teeth only slightly apart. The needle and cannula are inserted at the same points, but are directed inferiorly and posteriorly at 45° rather than anterosuperiorly.
Uriell et al (1989) 35 reported that arthroscopic lysis and lavage of the TMJ demonstrated better surgical outcomes for the early intervention group than for the late intervention group. Patients with a shorter duration of symptoms benefited more than those with a longer duration.
Murakami et al 36 reported that TMJ arthroscopic lysis and lavage has been shown to be specifically successful in intermediate and intermediate/late progression of ID (Wilkes stages III and IV), and showed an average 90% success rate with arthroscopic lysis and lavage in a 5-year follow-up study.
White, 37 in a 3-year follow-up study on 100 joints and 66 patients undergoing arthroscopic lysis and lavage, showed that 88% of patients had increased range of mouth opening (ROM), 93% were eating a regular diet, 63% reported no further treatment for pain management, and all patients were satisfied with the outcome and would undergo another arthroscopic procedure.
Holmlund et al, 38 while comparing with discectomy, found that the arthroscopic lysis and lavage procedure was almost equal to that of the open procedure in treating patients with chronic closed lock, with the patients’ choice being arthroscopic lysis and lavage because of its minimally invasive nature.
Recent Advances in Arthroscopy
Over the years there have been many advances in the field of TMJ arthroscopy. following discussion highlights few important points.
Laser Arthroscopy
The difficulty of treating some TMJ disorders has been evident since Annadale’s first surgical attempts in 1887. 39 The addition of lasers in the treatment of TMJ disorders with arthroscopy has offered a less invasive means of management then the traditional open TMJ surgery.
As seen with many other uses of the laser previously mentioned in this article, the laser offers many advantages over conventional arthroscopic instrumentation, including improved coagulation, allowing for better visualization and much greater precision. CO2 and Er:YAG lasers were not very effective in TMJ arthroscopy because of the synovial fluid environment. 40
McCain’s contributions to arthroscopy have advanced the field significantly, and techniques by Hendler and Koslin have been described as sculpting fibrocartilaginous and retrodiscal tissue safely and easily with the Hol:YAG laser.41-43
These techniques developed out of the knee arthroscopy experience pioneered by Fanton and Dillingham. 44 Previous techniques using the Nd:YAG laser were attempted, but they caused significant damage to the adjacent tissue owing to the depth of penetration of this laser.
As previously mentioned, Trauner showed that the Hol:YAG laser was less damaging to the surrounding tissues when sculpting fibrocartilage.
The Hol:YAG laser is a pulsed, mid-infrared laser at 2100 nm that works well in a saline environment and can be used with a fiberoptic quartz fiber. This allows for easy manipulation within the joint using standard triangulation techniques described by McCain with a quartz fiber. Generally, a power setting of 0.8 J and a pulse rate of 10 Hz can be used to ablate and sculpt tissue effectively.
The Hol:YAG laser can be used for discectomy, synovectomy, hemostasis, treatment of anterior disc displacement, dissection of fibrous adhesions, and scarring of retrodiscal tissue in the treatment of hypermobility. 45
Mazzonetto and Spagnoli describe meniscectomies through an arthroscope using a Hol:YAG laser to remove the disc and then using more traditional rotary instruments to recontour the condyle and glenoid fossa. 46 As with most TMJ procedures, the adjunctive physical therapy and use of an occlusal splint is still extremely important in the management of patients with TMJ disorders.
Some clinicians have augmented open arthroplasty techniques by using either the contact Nd:YAG or the carbon dioxide lasers for the dissection. 47 Techniques with and without the use of an operating microscope have been described and may significantly aid in the avoidance of nerve injury. The operating microscope can incorporate a coaxial laser with joystick control to aim the laser within the microscopic field. Comparative studies are needed to evaluate these techniques.
Footnotes
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.