
Abstract
Background
Silicone bands offer a non-invasive method for measuring environmental chemicals; however, their feasibility with young children is uncertain. This mixed-methods study examines toddler compliance with silicone bands, identifies predictors of compliance, and offers recommendations for research.
Methods
Children wore silicone wrist and ankle bands for 1 week; parents completed daily diaries capturing wear time of each band (hours) to indicate compliance (focal outcome). Mothers completed questionnaires capturing family characteristics and child cognitive and behavioral characteristics. Compliance and its associations with family and child characteristics were examined using descriptive, comparative, and associative statistics, and predictive modeling. Comments provided by parents in diaries and research assistants’ feedback were summarized to inform recommendations for future studies.
Results
Children (n = 115, 28–39 months) tended to be highly compliant with wearing both bands (56%) or the ankle band only (23%), as reflected by a median of 11–12 hours/day of wear time over the week. Compliance was higher for ankle than wrist bands (p-value <0.001). Wear time was not associated with child age, sex, associated clothing when wearing the band, or socioeconomic status (p-values >0.05). Child language and anxiety were positively associated with wristband compliance (p-values ≤0.038), whereas higher behavioral inhibition and lower effortful control were associated with higher ankle band compliance (p-values ≤0.016). Qualitative data suggest improving band appeal and resolving sizing issues could improve compliance.
Conclusions
Results support the feasibility of deploying silicone bands with toddler-aged children. Studies using child-worn bands should account for hourly wear time, as compliance may predict both chemical exposure levels and child characteristics.
Introduction
Young children are often disproportionately at risk for, and vulnerable to, environmental chemical (EC) exposures.1,2 Due to a combination of increased hand-to-mouth behavior and oral exploration, closer proximity to the floor, and needs for more food, water, and air by weight compared to adults, young children encounter a larger variety and higher body burden of ECs than older children and adults.1,3–6 Moreover, with early life representing a sensitive and rapid period of organ development, young children often experience enhanced vulnerability to the toxic effects of ECs.6,7 Characterizing the landscape of exposures that young children experience remains challenging, though this information is critical towards informing inferential study designs and remediation approaches.
Methods to evaluate EC exposures in young children span biomonitoring efforts using human biospecimens (e.g., blood, urine), samples of the environment (e.g., dust wipes, air monitoring) or computationally-driven approaches (e.g., exposure pathway modeling).8,9 Recent studies have also incorporated silicone band technologies as an innovative method to ascertain personal-level exposure information.10,11 Silicone bands are worn for multiple days, absorbing a wide range of chemicals that participants come into physical contact with. Bands can then be analyzed post hoc for chemical composition using analytic chemistry approaches,12,13 including gas chromatography and/or liquid chromatography mass spectrometry methods. Relevant to the researcher, advantages to silicone bands include the acquisition of proximal chemical exposure data across multiple physical environments, low up-front costs, and the ability to be deployed by data collectors with minimal training and/or in remote data collection settings.9,14,15 Of importance to the participant, these technologies are uncomplicated and non-invasive.9,15 Due to these advantages, silicone bands are being incorporated into the design of a rapidly increasing number of environmental health studies.
ECs measured in silicone bands include those of high relevance to childhood health and development. For example, exposure to phthalates, flame retardants, parabens, pesticides, polycyclic aromatic hydrocarbons (PAHs), and per- and polyfluoroalkyl substances (PFAS), which have all been adversely associated with concurrent and prospective indices of child health and development,4,16–22 can be measured using silicone bands.23–28 Insofar, studies enrolling preschool-aged (3-5 years old) children specifically demonstrate that silicone wristbands can capture individual-level exposure to phthalates, 29 flame retardants,29,30 and pesticides. 31 Comparisons to house dust, hand wipes, and child urine samples corroborate the validity of the child-worn silicone band for assessing many phthalates and flame retardants.12,29 ECs captured by child-worn silicone bands have also been associated with child outcomes as expected. In a sample of preschool children (N = 69), exposure to organophosphorus flame retardants (OPFRs) measured via child-worn silicone bands was associated with higher externalizing behaviors and lower responsibility scores. 32
Despite their benefits, silicone bands have notable limitations as exposure assessment tools for young children, as they require several days to capture chemical exposure, must remain securely worn without being lost, and may be cumbersome or bothersome. To our knowledge, no study has evaluated the feasibility of deploying silicone wrist and ankle bands with young children (ages 2–3 years old). Given that very young children are especially susceptible to ECs, it is crucial to ensure their compliance in wearing silicone bands to enable accurate measurement of exposure levels.
Prior studies have examined crude wear-time (in days) of silicone bands in preschool-aged children as a function of sociodemographic characteristics like child race, age, and an aggregate measure capturing family context. 30 Still, other child characteristics, such as behavioral inhibition, anxiety, temperament, and inhibitory control, may be differentially associated with children’s tolerance of the band, and thereby the extent to which the silicone bands collect ECs. Parental characteristics, for example, their own social and psychological demands or their participation in wearing a silicone wristband, might also influence the extent to which they chaperone their child’s band wear. If not properly accounted for, these child and parent characteristics could confound associations between EC levels captured via silicone bands and child cognitive and behavioral outcomes. For example, if children with poorer inhibitory control have higher wear time (due to increased chaperoning), failing to adequately adjust for band wear time could bias associations between chemical exposure and child inhibitory control away from the null. To our knowledge, no study has thoroughly investigated the child and parent characteristics that may predict a child’s compliance with wearing the silicone band.
The objectives of our study are guided by three research questions (RQs). First, how compliant are toddlers with wearing the silicone wrist and ankle band? To answer this, we examine the number of hours that young children (ages 2–3 years) wear a silicone wrist and ankle band over a 7-day period. We hypothesized that children would fall into two categories: those highly compliant with at least one band and those highly uncompliant with both bands. Second, to what extent do child and family characteristics predict child band compliance? To answer this, we test whether various a priori-selected child and family characteristics are associated with children’s wear time of the wrist or ankle band. We hypothesized that higher child negative affectivity and lower effortful control would be independently associated with lower band wear time. Third, how can studies improve compliance and participant experiences for future studies? To answer this, we summarize the experiences of participating parents and researchers, thereby inferring recommendations for future studies interested in using silicone bands to quantify ECs in the young child’s environment. Given the current momentum surrounding silicone band technologies, this study design guidance will facilitate the effective integration of silicone bands into investigations that focus on early childhood ECs.
Method
Participants
This mixed-methods study was embedded in the Brain and Early Experience (BEE) Study—a longitudinal cohort study following up to 208 mother-child dyads. The overarching goal of the BEE Study is to examine how aspects of the social (e.g., caregiving, language) and physical (e.g., chemical, home, sleep) environments in the first 3 years of life influence child cognitive and socio-emotional development. Among other measures, the longitudinal study administers robust parent-reported surveys capturing early child experience and functioning. The current study focuses on mother-child dyads who participated in the toddler visit (N = 130). Although any parent or guardian was eligible to participate in the 30-months visit, all adult participants were the child’s mother. A full description of the protocol, including recruitment strategies and enrollment criteria, are reported elsewhere. 33 Procedures for the toddler visit, which covered parent-reported surveys among other activities were approved by the University of North Carolina at Chapel Hill Institutional Review Board (#17-1914). Procedures for the silicone band activity were approved by the same Institutional Review Board (#21-1223). Adult participants provided written informed consent prior to enrollment and at every follow-up visit. Adult participants also provided written parental permission for their child to participate in study activities. Specifically, for the 30-months visit, written consent was obtained electronically prior to the visit through Research Electronic Data Capture (REDCap).34,35 A research assistant then reviewed the consent form with the participating family at the start of the remote visit on Zoom.
Demographic characteristics of the analytic sample (n = 115 dyads).
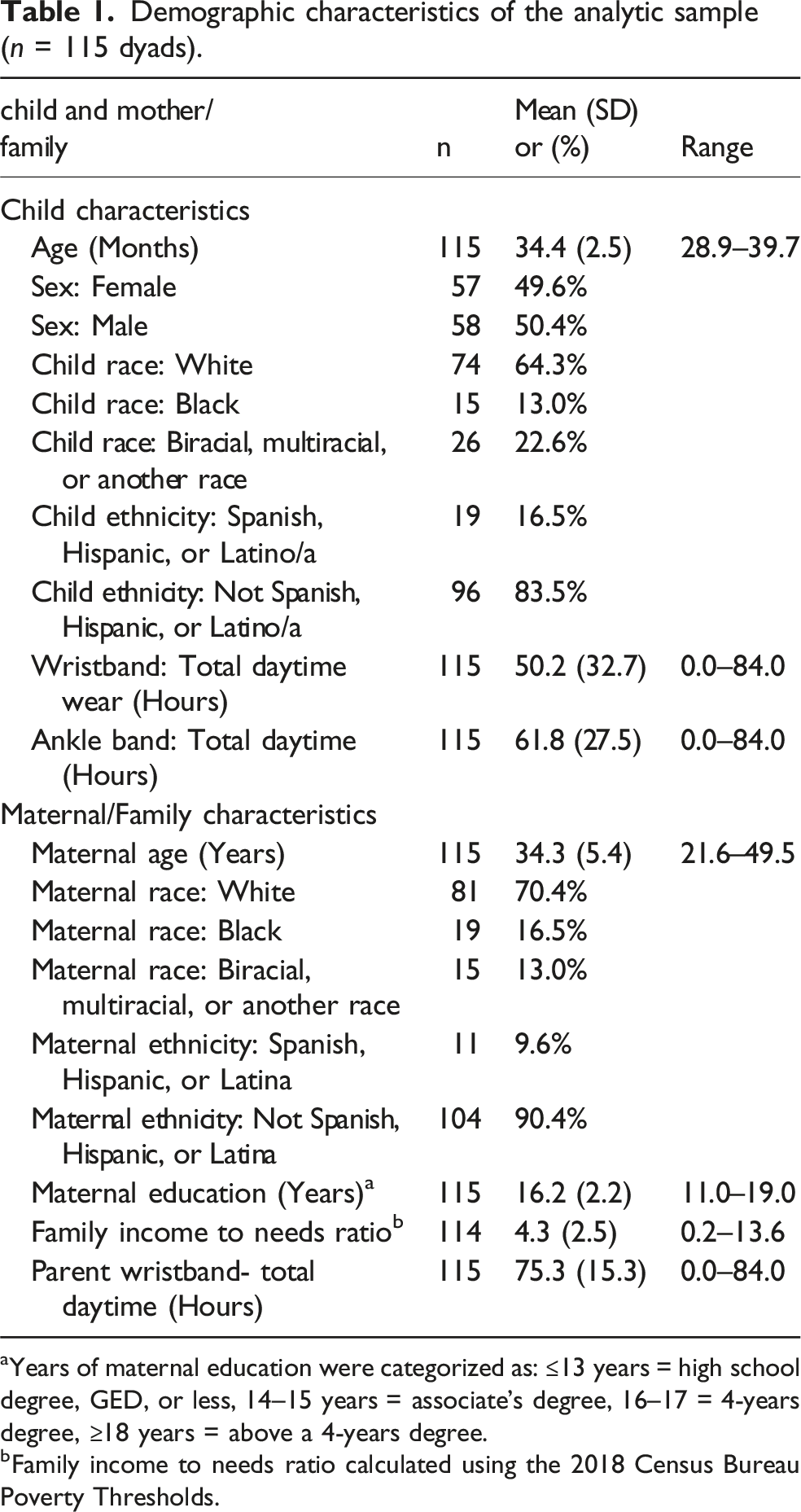
aYears of maternal education were categorized as: ≤13 years = high school degree, GED, or less, 14–15 years = associate’s degree, 16–17 = 4-years degree, ≥18 years = above a 4-years degree.
bFamily income to needs ratio calculated using the 2018 Census Bureau Poverty Thresholds.
Mothers were asked to self-identify their ethnicity and race and their child’s ethnicity and race. Those with Hispanic ethnicity descend from a Spanish-speaking populations, and those with Latino ethnicity have Latin American descent; either may be any race. Hispanic or Latino ethnicity for this study was determined by the mothers’ response to the question: “Are you [do you consider your child] Spanish, Hispanic, or Latino?” Only 11 (9.5%) mothers identified themselves and 19 (16.5%) identified their child as Spanish, Hispanic, or Latino. Race was determined by mother’s response to the question “How would you describe your [your child’s] primary race?” Most mothers identified as White (n = 81; 70.4 %), whereas 16.5% (n = 19) of mothers identified as Black or African American, and 13.0% (n = 15) identified as Biracial, Multiracial, or another race. Most children were similarly identified to be White (n = 74, 64.3%), whereas 13.0% (n = 15) were identified as Black or African American, and 22.6% (n = 26) of children were identified as Biracial, Multiracial or another race.
Mothers were also asked “How many years of school have you completed?” Reported years of education were categorized according to standard U.S. educational benchmarks (e.g., ≤13 years = high school degree, GED, or less; 16 years = a 4-year college degree), as detailed in Table 1 (note). This sample was more diverse with respect to education level: 24 (20.9%) completed a high school diploma or its equivalent (General Education Development or GED) or less, 41 (35.7%) completed a 4-year degree, and 43 (37.4%) completed a degree above a 4-year college degree.
Dyads (n = 15) who were removed from the analysis due to active (n = 2) or passive (n = 13) refusal were more likely to identify their maternal race as Black or African American, have lower levels of maternal education, and lower family income to needs ratios on average than dyads included in the analytic dataset (p-values ≤0.041); there were no differences in child age or sex.
Procedure
Mother-child dyads completed the toddler visit—a 90-min, remote home visit by Zoom. Prior to their scheduled visit, mothers were shipped a box of materials and devices that would be used during and following the Zoom visit. Families were provided with sets of wrapped, unused silicone bands prepared for study usage, as previously described. 11 Families were given a prepared adult-sized (202 mm circumference) wristband for the mother to wear during the week. For the child, each box included the following sets of bands (one wrist and one ankle): (1) two toddler-sized bands (152 mm circumference), (2) a toddler-sized band for the wrist and a youth-sized band for the ankle (180 mm circumference), and (3) two youth-sized bands. Band sets were wrapped together in clean aluminum foil and stored in a clean plastic sandwich bag. On the outside of the aluminum foil was a paper label reading “Unused Bands” that was placed so that if someone opened the package, the paper would be damaged, indicating that the bands would be unusable for other participants. Also in the shipment were unwrapped toddler- and youth-sized bands for measurement purposes. Mothers were instructed to have their child try on the toddler- and youth-sized bands on their ankle and wrist to determine the best fitting set and open only the unused set that would best fit their child. The unused bands were returned to the box unopened for mail back to the study office at the completion of the activities. A blue band was designated as the wristband and a yellow band was designated as the ankle band—embossing on the band read “BEE Happy [Thumbs Up Emoji] Child Wristband” or “BEE Happy [Footprint Emoji] Child Ankle Band” (see Supplemental Material 1 for a photograph of the child ankle and wristband). Activity instructions and the daily diary reminded parents of the color assigned to the wrist and ankle band.
Mothers were asked that their child wear the silicone wristband and ankle band for seven consecutive days, including when sleeping, bathing, or swimming, and mothers were asked to wear their silicone wristband for the same duration. The 7 days of wear typically started immediately following the Zoom visit; though, parents could choose another start date within the week to accommodate their schedule. Mothers who elected a later start date were instructed to open the silicone bands when they were ready to begin their 7 days of wear. Children were also asked to wear an ankle band actigraphy monitor for the same seven consecutive days and a language monitor in a vest for 2 days (these data are not presented). Children could wear the ankle band on the same or opposite ankle as the actigraphy monitor. Mothers completed a series of research assistant (RA) administered- and self-administered questionnaires during and following the visit using REDCap.
Clean pieces of foil and plastic bags were provided for the return of each band—on the outside of each plastic bag, a paper label indicated whether the contents should include the used parent wristband, child wristband, or child ankle band. After 7 days, mothers wrapped used bands in the provided foil and shipped the materials with other post-visit activities to the laboratory. Parents and RAs worked together to coordinate the shipping of the materials; hence, parents were reminded through the daily diaries and through their interactions with RAs coordinating the shipping when the 7 days of post-visit activities were complete. Mothers were compensated $50 for their family’s participation in the remote Zoom visit and $25 for attempting post-visit activities.
Participant survey measures
Child and family characteristics
Child and family characteristics were reported by the mother to the RA and captured via REDCap during the toddler remote visit. Mothers reported their child’s birthdate (to calculate age), sex, race, and ethnicity as well as their own birthdate (to calculate age), race, ethnicity, and highest level of education. Mothers also reported their household income and number of adults and children living in the household. This information was compared to the 2018 Census Bureau Poverty Thresholds 36 to create a ratio score of the family’s income relative to their needs. Mothers reported the number of places where the target child receives care aside from with the mother and any live-in partner. Mothers reported whether the target child has been suspected or identified to have: (1) speech or language impairment; (2) problems related to blindness or vision; (3) any hearing impairment; (4) problems related to physical or orthopedic impairment; (5) any physical or developmental delay; (6) emotional or behavioral problems. We created a dichotomous indicator capturing whether the mother reported any suspected or identified delay or disability.
Silicone band daily diary
A paper and pencil daily diary was completed by parents during the 7-day period that the child was expected to wear the silicone wrist and ankle band (typically, this immediately followed the toddler remote visit). Parents reported which hours the child wore each band, broken into one-hour increments; there were also options for “All 24 hours” and “None” to reduce burden and confusion. Parents indicated if their child wore long sleeves or long pants that day (aside from coats worn briefly). Each diary page included space to provide written comments (see Supplemental Material 2). Children’s wear time of the silicone bands as indicated in the daily diaries served as our primary variables of interest, reflecting compliance with silicone bands. We additionally categorized written comments to summarize the experiences of parents in the interest of informing recommendations for future research.
The remainder of the questionnaires were completed independently by the parent via an e-mailed REDCap link within approximately 2 weeks of their child’s toddler visit. Additional information about scores generated from questionnaires is available in Supplemental Table 1.
MacArthur-bates communicative development inventory-III (MCDI)
The communicative development inventory was used to evaluate children’s expressive and receptive language. 37 The inventory (124 items) assesses the child’s vocabulary, grammar complexity, and language comprehension. Item responses reflect item endorsement (no vs yes). Construct validity has been established using the McCarthy–General Cognitive Index, McCarthy Verbal Index, and the Peabody Picture Vocabulary Test.37,38 An overall early language skills score represents the proportion of all endorsed items. 39
Early childhood behavior questionnaire (ECBQ)
The ECBQ was employed to evaluate children’s temperament. 40 Mothers were given 107 statements of child behavior and asked to rate how often they observed the behavior from their child in the past 2 weeks on a scale from 0 (never) to 6 (always). We explored the effortful control (mean of 32 items), negative affect (mean of 48 items), and surgency (mean of 25 items) scores as well as the discomfort (mean of 7 items) subscale. An example item for the discomfort subscale, which is included in the negative affect total score is “During quiet activities, such as reading a story, how often did your child fiddle with their hair, clothing, etc.” The ECBQ scales demonstrate moderate longitudinal stability and inter-rater reliability. 40
Behavioral inhibition questionnaire (BIQ)
The BIQ was used to capture children’s behavioral inhibition. 41 Mothers were given 30 statements describing children’s behavior in various situations and asked to rate how often they would expect their child to demonstrate that behavior on a scale from 0 (hardly ever) to 6 (almost always). We focus on the social subscale (mean of 14 items) and the novelty subscale (mean of 16 items), which comprise the total behavioral inhibition score (mean of 30 items). Example items for the social and novelty subscale include “Is shy when first meeting new children” and “Seems nervous or uncomfortable in new situations,” respectively. In a sample of 3–5-year-olds, maternal-reported total BI scores were strongly correlated with the inhibition subscale of the Temperament Assessment Battery for Children. 41
Preschool anxiety scale (PAS)
The PAS was used to assess children’s frequency and severity of anxiety symptoms. 42 Mothers were asked to rate how accurately each of 28 statements described their child on a scale from 0 (not true at all) to 4 (very often true). An example item is “Asks for reassurance when it doesn’t seem necessary.” A total anxiety score was created by taking a mean of all 28 items. Concurrent validity has been demonstrated using the Child Behavior Checklist internalizing scale. 42
Parental stress index (PSI)– short form (PSI-SF)
The PSI-SF is a 36-item questionnaire designed to assess parental stress in the parent-child system, including stress related to child rearing, social support, interactions with their children, and children’s self-regulatory abilities. 43 Mothers report their level of agreement to 33 statements such as “I feel trapped by my responsibilities as a parent” on a scale from 0 (strongly disagree) to 4 (strongly agree). Three additional items are scored on a non-Likert scale but are translated to scores of 0-4. We focus on the total parental stress score (mean of all 36 items) and the difficult child subscale (mean of 12 items).
Data analysis
All analyses were performed using R studio with R version 4.3.1. 44 Input files and R code are publicly available online via the Ragerlab Github repository. 45 Packages used throughout the analysis include tidyverse, 46 openxlsx, 47 table1, 48 ggpubr, 49 rstatix, 50 ltm, 51 FSA 52 and randomForest. 53 Results were visualized using ggplot2, 54 patchwork 55 and Adobe Illustrator. 56
We summarize analyses and results as they correspond to three RQs: (1) To what degree are toddlers compliant with wearing the silicone wristband and ankle band? (2) Are there child and family characteristics that are associated with child wrist and ankle band wear time? and (3) Can we summarize the experiences of our participants and researchers in ways that will inform recommendations for future studies?
For all quantitative analyses, we examined band wear time separately by placement (ankle vs wrist). Though children were requested to wear the bands 24/7, we limited analyses to daytime wear only (7 AM – 7 PM), as we were interested in children’s conscious time wearing the bands. Nighttime wear data (7 PM–7 AM) are available in the Ragerlab GitHub repository. 45 We considered results to be statistically significant at alpha (ɑ) = 0.05. To answer RQ1, we relied on descriptive statistics and Cronach’s alpha (α) as a measure of internal consistency.
To answer RQ2, we a priori selected child and family characteristics as potentially associated with child compliance with silicone bands. We considered that children may be more compliant with wearing the bands if they were older, they did not have a disability, the bands were covered by pants or long sleeves, parents were nearby to chaperone compliance, or the mother was wearing her own band (by modeling behavior or being reminded of the activity). We also considered that compliance could differ by child sex. Hence, we examined whether child’s age, disability status, clothing, use of childcare outside of the home, sex, and mother’s daytime wear of her own silicone wristband predicted child’s compliance with the band activity using Wilcoxon signed-rank tests, Wilcoxon rank sum tests, and analysis of variance (ANOVAs).
Next, we considered that children may be more compliant with wearing the bands if they had higher reported effortful control or surgency or if they had lower behavioral inhibition, anxiety, or were less affected by discomfort. We considered that children with more advanced language skills may be better able to negotiate band wear or comprehend the activity. We considered that parents with higher socioeconomic status, older mothers, or mothers with lower parenting stress may be better able to chaperone children’s band wear (promoting higher compliance). Hence, using Spearman’s rank correlation coefficients and linear regression, we examined whether children’s total daytime wear of the wristband or ankle band was associated with child temperament indicators (effortful control, surgency, negative affect, and discomfort), language, behavioral inhibition (total, to social situations, and to novelty), and anxiety, as well as maternal demographic characteristics (income to needs ratio, education, age) and parenting stress. We additionally tested for differences in these child and family characteristics by categories of wear time using Wilcoxon rank sum tests.
Random forest modeling was used to assess the predictive value of different variables on ankle and wristband wear time. Random forest modeling is a supervised machine learning algorithm that utilizes multiple decision trees, each trained on a subset of data from the dataset. Decision trees are hierarchical models built using a random select subset of variables as nodes, which split into subsequent nodes and ultimately, a decision. 57 The Gini importance index of each variable within these models can be determined as the average increase in node purity expressed as the change in the probability of a correct decision if a sample was classified using that variable. In this analysis, this was achieved using the “randomForest” R package. 53 Complete case analysis was performed for the prediction variables of interest using five hundred trees in each model. Note, childcare and the mean use of long sleeves/pants were excluded in the random forest model only because of high missingness.
To answer RQ3, we relied on comments made by mothers on the silicone band daily diary and feedback from RAs. Daily diaries were reviewed and coded by two authors (JF and AW). First, all comments were exported into two master spreadsheets. Both authors independently reviewed comments and generated a series of qualitative codes. The authors then reviewed and compared their respective codes and through conferencing, produced one coding scheme of 10 codes (one code indicates ‘no comment’). One author (AW) then categorized all comments into one or more codes, which was reviewed by the other (JF). All disagreements were resolved through conferencing.
Finally, we asked the lead RA (NS), who led most of the toddler visits, to gather feedback from RAs who facilitated the wristband activity about issues they encountered; feedback was gathered in an online working document. Authors NS and AW reviewed this feedback together and organized the document into a narrative of current practices and associated problems. They then brainstormed ideas for proposed solutions.
Results
As described, 11.5% of the total sample (of N = 130) of child participants were removed from analyses due to lack of returned diary (n = 13) or active refusal (n = 2). The following results focus on the sample of participants who returned a silicone band diary with any portion of the diary completed (n = 115).
Toddlers’ silicone wristband and ankle band wear time
Considering a maximum of 84 hours of daytime wear over the course of the week (12 hours per day over 7 days), children’s median wear time was 66 hours for the wristband (mean = 49.8 hours) and 73 hours for the ankle band (mean = 61.2 hours), with more variability in wear time for the wristband (SD = 33.2) than the ankle band (SD = 28.4) (see Figure 1). Overall, children wore the ankle band on average 11.6 more hours than the wristband (paired Wilcoxon signed rank test p < 0.001). Reliability of daily wear time over the 7 days was high for the wristband (Cronbach’s α = 0.94) and the ankle band (Cronbach’s α = 0.91). The first day of the 7-day week showed varied levels of wear time, as children often began their week-long silicone band activity at the end of the toddler remote visit (part way through the day). Wear time for the remaining 6 days showed an even more consistent pattern of wear time (Cronbach’s α = 0.96 for wrist and Cronbach’s α = 0.93 for ankle). Total daytime (left) and nighttime (right) wear of the silicone wrist and ankle bands by child participants (n = 115) over the 7-day wear period.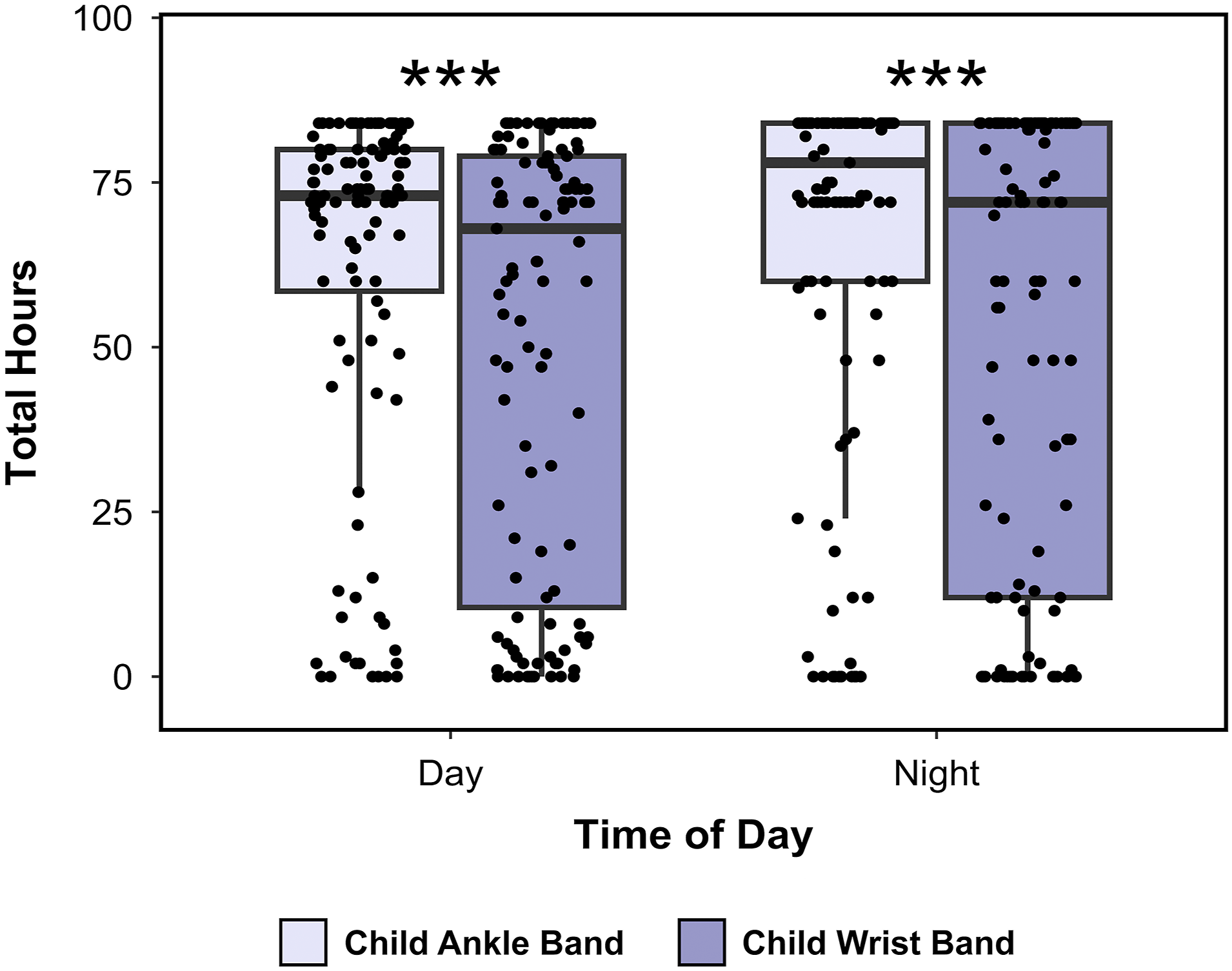
Groupings of total daytime wear time (Panel A) and median daily wear time hours (Panel B) of silicone wrist and ankle bands across a 7-day period among a sample of n = 115 children.
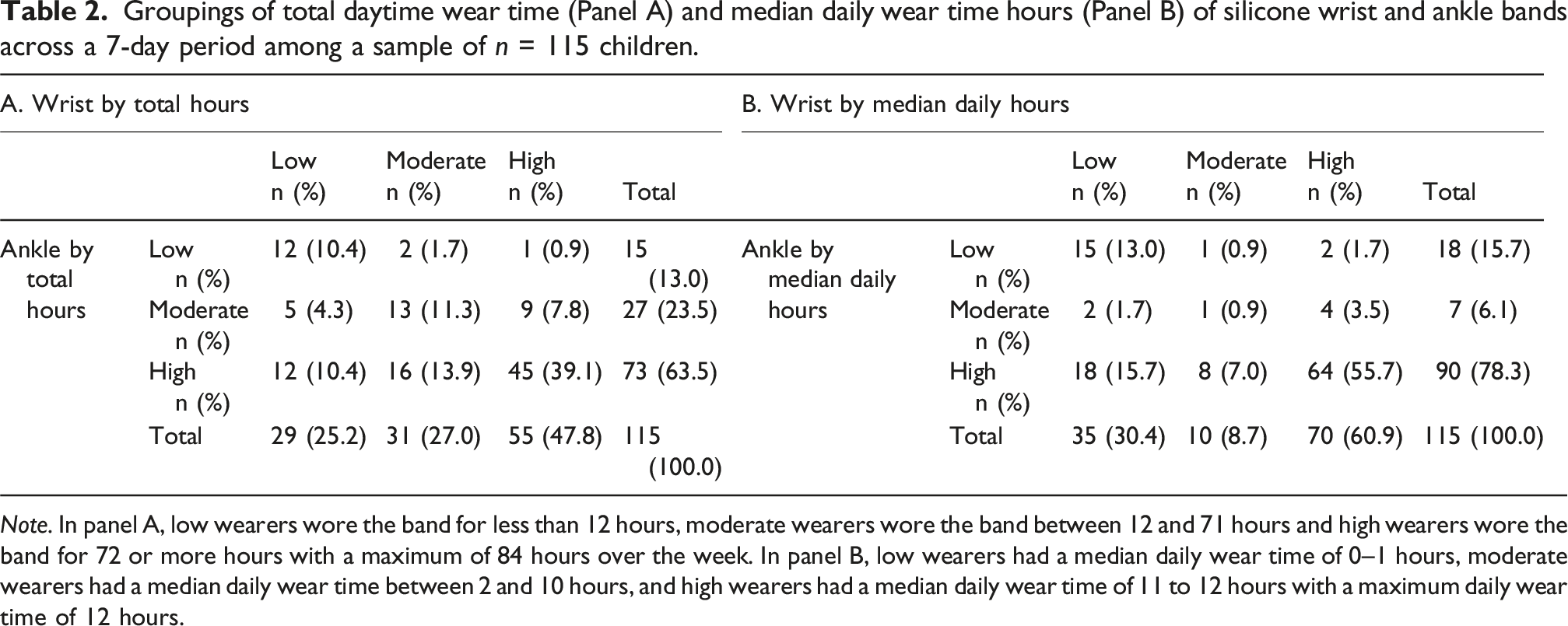
Note. In panel A, low wearers wore the band for less than 12 hours, moderate wearers wore the band between 12 and 71 hours and high wearers wore the band for 72 or more hours with a maximum of 84 hours over the week. In panel B, low wearers had a median daily wear time of 0–1 hours, moderate wearers had a median daily wear time between 2 and 10 hours, and high wearers had a median daily wear time of 11 to 12 hours with a maximum daily wear time of 12 hours.
When considering the median daily wear time, 56% of children (64/115) had a median of 11–12 hours of daily wear time for both the wrist and ankle band over the week and were considered “high daily wearers,” whereas 13% of children (15/115) had a median of 0–1 hours of daily wear time for both the wrist and ankle band over the week and were considered “low daily wearers.” Another 23% of children (26/115) had a median of 11–12 hours of daily wear time for the ankle but 0–1 hours (16%) or 2–10 hours (7%) of daily wear time for the wristband and were considered “high daily ankle wearers only.”
Range of actual daytime hours reported for the wristband and ankle band as it relates to expected total days of reported wear.
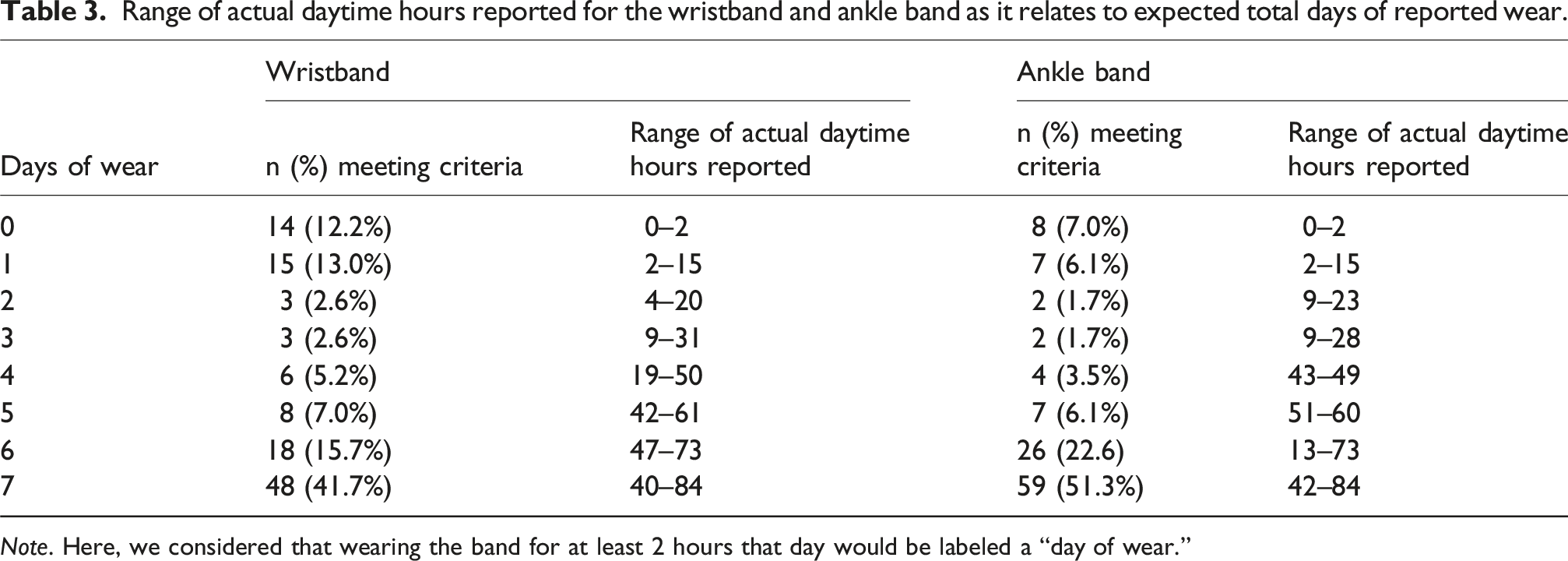
Note. Here, we considered that wearing the band for at least 2 hours that day would be labeled a “day of wear.”
Child and family characteristics associated with child band compliance
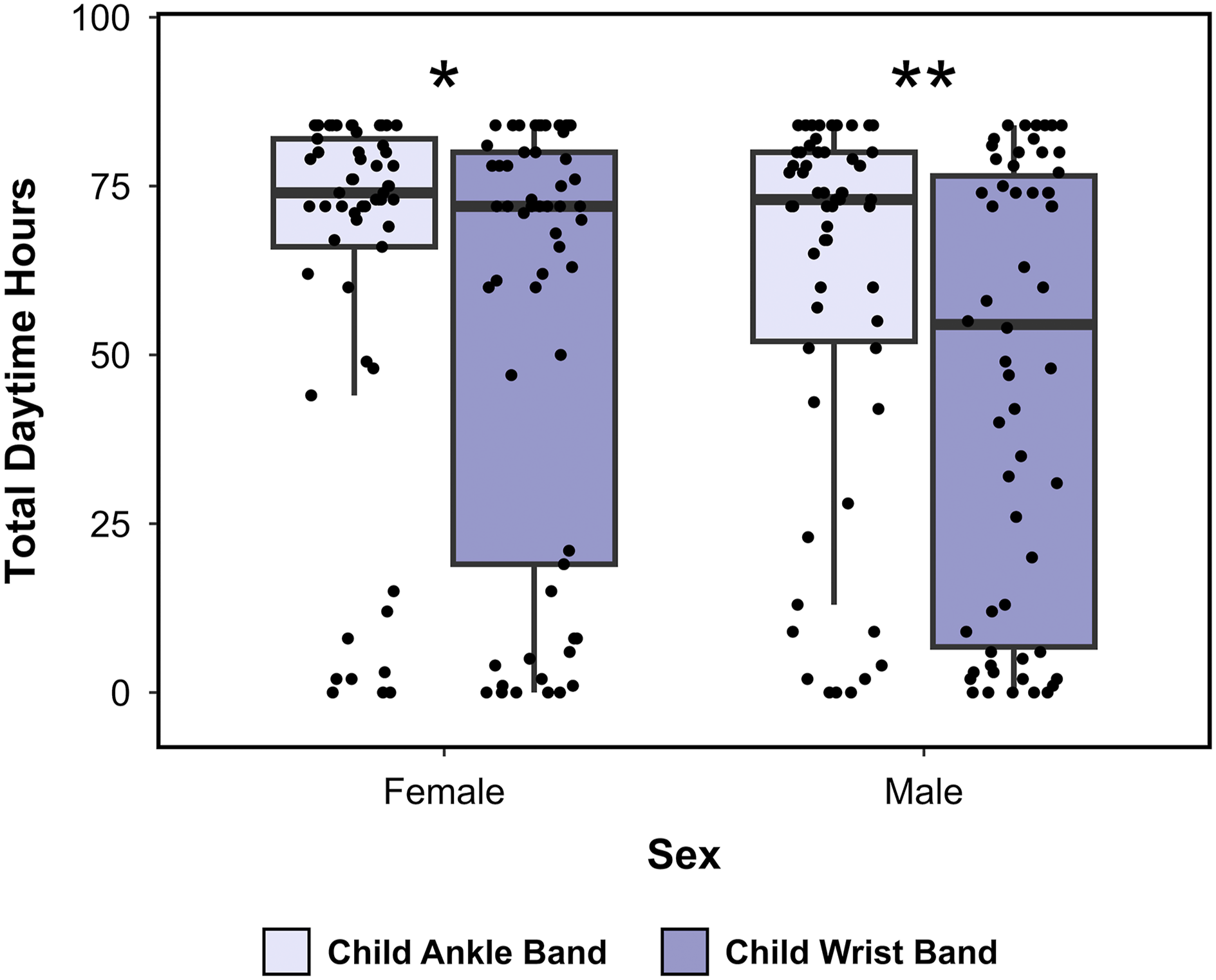
We tested whether total daytime wear of the wrist or ankle band over the week varied as a function of child age, disability, sex, mother’s daytime wear of her own silicone wristband, and child clothing worn while wearing the band (long-sleeve shirt for wristband; long pants for ankle band). We also examined whether categories of wear time, grouped into low/moderate wear (<72 hours) or high wear (≥72 hours), were associated with child and family characteristics (see Figure 2/Supplemental Tables 2 and 3). In comparison to male children, female children had longer total daytime wear hours for the wristband (Female mean = 55.1 total hours; Male mean = 46.3 total hours) and ankle band (Female mean = 63.9 total hours; Male mean = 60.6 total hours), though these were not statistically significant differences (wristband Wilcoxon p = 0.163; ankle band Wilcoxon p = 0.372). The bivariate correlation between wrist and ankle band total wear time was stronger in female children (rho = 0.76, p < 0.001) than in male children (rho = 0.27, p = 0.034). The preference for the ankle band over the wristband (as indicated by total wear time) was apparent in both male (Wilcoxon p = 0.004) and female (Wilcoxon p = 0.002) children (see Figure 3). Both child ankle band total wear time and child wristband total wear time were positively correlated with parent wristband wear time (rho = 0.34, p < 0.001 and rho = 0.17, p = 0.072, respectively). Child, maternal, and family characteristics by daytime wear categorizations where darker colors indicate higher values of the child, maternal, and family characteristics in question (e.g., sex: proportion female, child age, use of childcare). Total daytime hours of wear of the silicone wrist and ankle bands by sex over the 7-day wear period.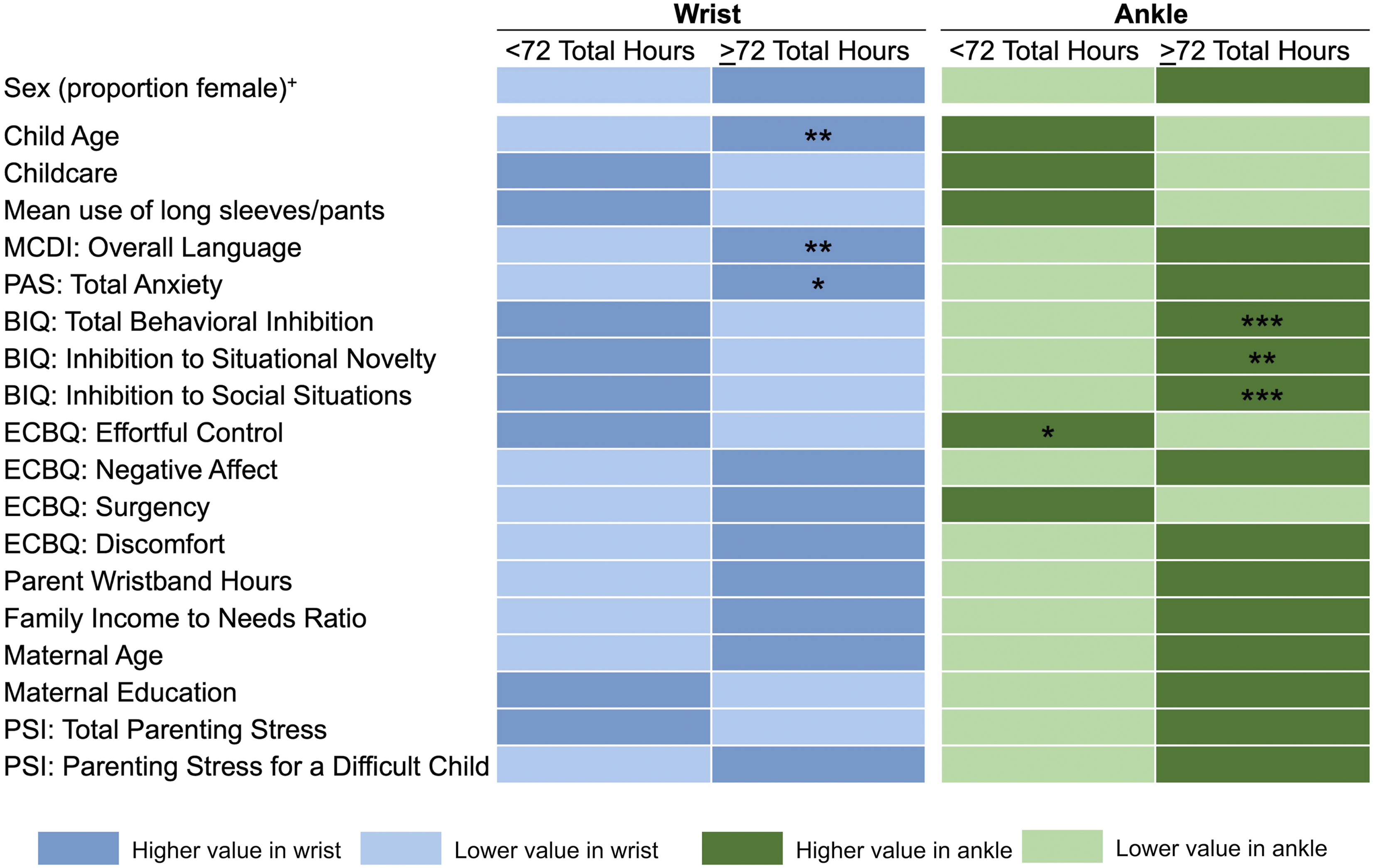
Child’s age was not associated with total daytime wear for the wrist (Spearman p = 0.098) or ankle band (Spearman p = 0.966) when considering daytime wear continuously. Stratification by sex also showed no significant associations between age and wear time (data not shown). However, categorizing participants into low/moderate vs. high levels of weekly daytime wear revealed that children who were “high total wristband wearers” were on average older (mean age = 35.1 months) than children who were “moderate-low total wristband wearers” (mean age = 33.8 months, p = 0.011) (see Supplemental Figure 1).
Child’s average days of wearing of long sleeves and long pants across the week were not associated with their total daily wear time for the wristband (r = −0.13, p = 0.172) and ankle band (r = 0.02, p = 0.804), respectively. Children with missing clothing data for all 7 days (n = 7 for wrist, n = 6 for ankle) were excluded from these correlations. Though the median daytime wear time for the wristband decreased with increasing sources of outside childcare, there were no significant differences between the number of childcare sources and total wear time for the wristband (Kruskal-Wallis p = 0.592) or ankle band (Kruskal-Wallis p = 0.609). There were also no differences in total wristband (Wilcoxon rank sum = 870, p = 0.482) or ankle band wear time (Wilcoxon rank sum = 770, p = 0.876) between children who were reported by their mother to have a suspected or identified delay or disability (n = 19) and children who did not have any suspected or identified delay or disability (n = 83).
Children’s total daytime wear of the wristband was significantly correlated with MCDI total language scores (rho = 0.26, p = 0.015). Children who had 72 or more hours of wristband wear time had on average higher MCDI language scores (Wilcoxon rank sum = 835.5; p = 0.015) as well as higher PAS anxiety scores (Wilcoxon rank sum = 583.5, p = 0.038) than children who had fewer than 72 hours of wristband wear time across the week (see Figure 4). However, language and anxiety were not significantly associated with total wristband wear time in regression models when adjusting for child age and sex (language p = 0.077; anxiety p = 0.229). Box and whisker plots of child language (a) and anxiety (b) between children who wore the silicone wristband for <72 total hours or ≥72 total hours. Correlations between total wrist wear time and child language (c) and anxiety (d).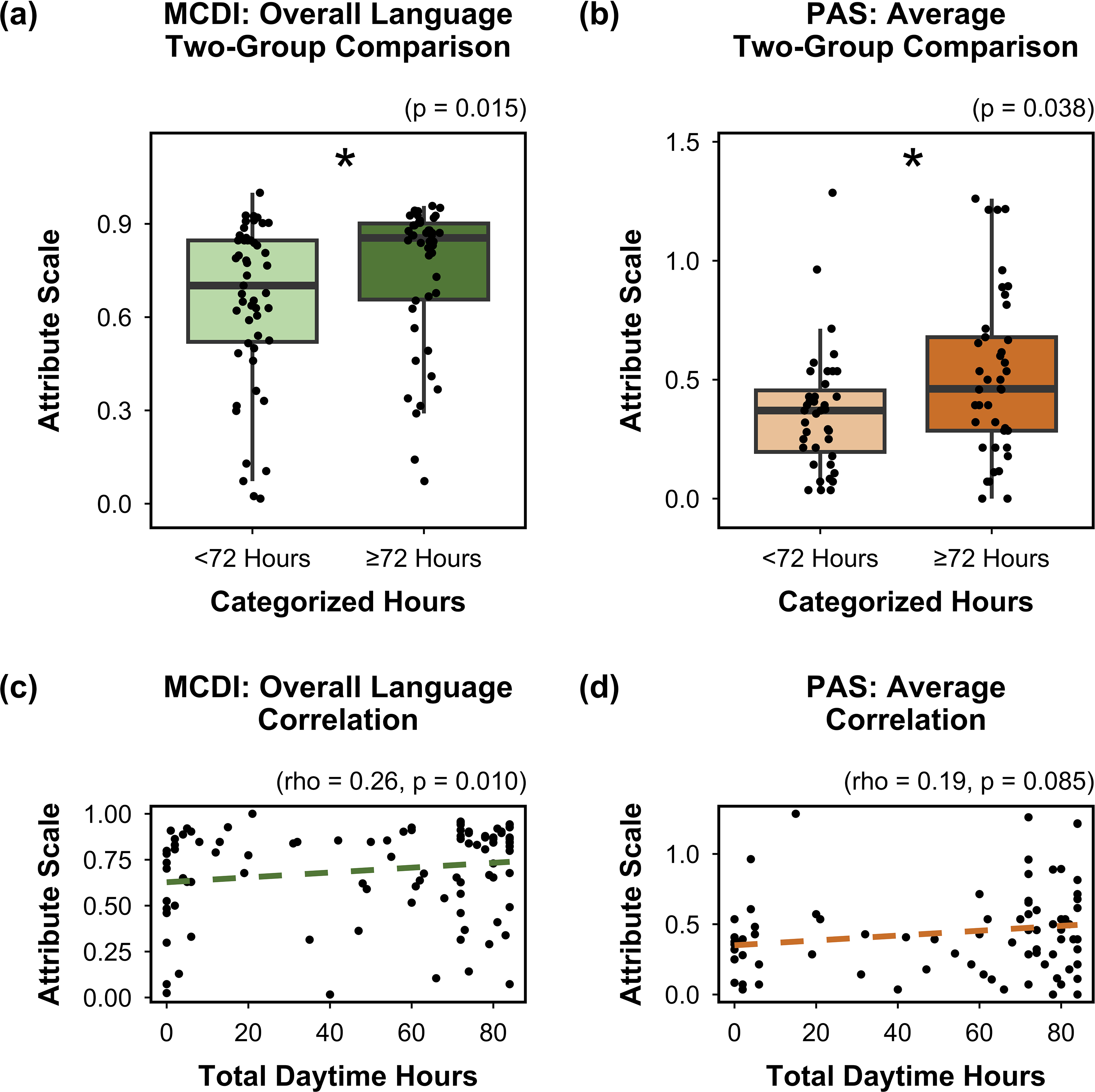
Children’s total daytime wear of the ankle band was positively correlated with BIQ total behavioral inhibition (rho = 0.34, p < 0.001); both components of the behavioral inhibition total score (social and novelty) were positively correlated with the ankle band wear time (rhos = 0.31–0.35, social p < 0.001, novelty p = 0.002). Similarly, children who had 72 or more hours of ankle band wear time had on average higher social behavioral inhibition (Wilcoxon rank sum = 605.5, p = 0.001), behavioral inhibition to novelty (Wilcoxon rank sum = 665.5, p = 0.003), and total behavioral inhibition scores (Wilcoxon rank sum = 644, p = 0.001) as well as lower effortful control scores (Wilcoxon rank sum = 1536.5; p = 0.016) than children who had fewer than 72 hours of ankle band wear time (see Figure 5). Child effortful control and behavioral inhibition were not significantly associated with total daytime wear of the ankle band after adjusting for age and sex in linear regression models (effortful control p = 0.093; social behavioral inhibition p = 0.086; behavioral inhibition to novelty p = 0.246; total behavioral inhibition p = 0.112). Box and whisker plots of child behavioral inhibition to novelty (a), social behavioral inhibition (b), total behavioral inhibition (c), and effortful control (d) between children who wore the silicone ankle band for <72 total hours or ≥72 total hours over the 7-day period. Correlations between total ankle wear time and behavioral inhibition to novelty (e), social behavioral inhibition (f), total behavioral inhibition (g), and effortful control (h).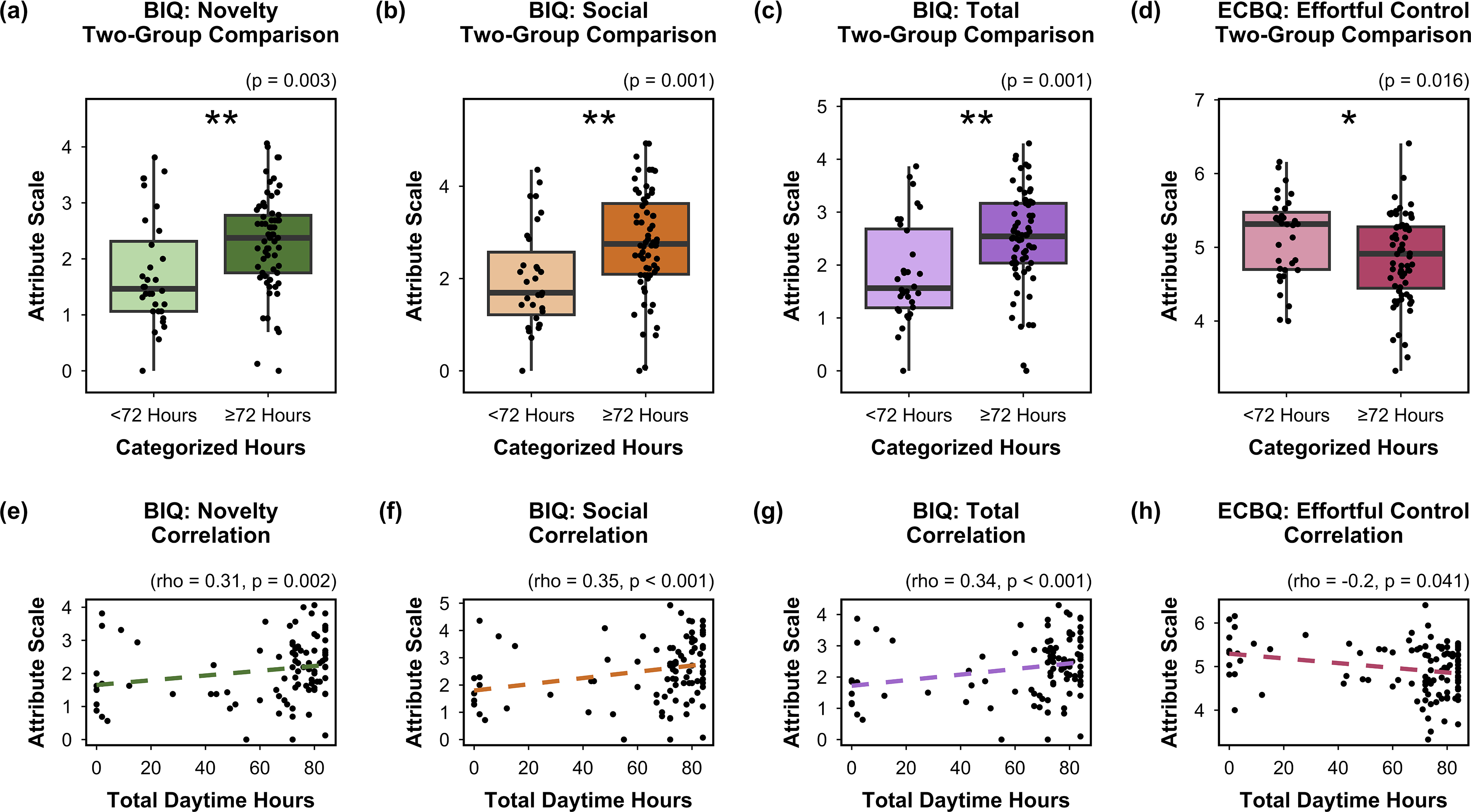
Children’s total daytime wear of the wristband or ankle band were not significantly correlated with family income to needs ratio (wrist rho = 0.04, p = 0.698; ankle rho = 0.14, p = 0.131), maternal education (wrist rho = −0.11, p = 0.229; ankle rho = 0.03, p = 0.764), maternal age (wrist rho = −0.10, p = 0.278; ankle rho = −0.02, p = 0.812), mean parenting stress (wrist rho = 0.05, p = 0.643; ankle rho = 0.06, p = 0.532), or parenting stress over a difficult child (wrist rho = 0.09, p = 0.360; ankle rho = 0.06, p = 0.517) (see Figure 2/Supplemental Table 3). Categories of children’s wear time (<72 hours vs ≥ 72 hours) were similarly not associated with socioeconomic status or parenting stress measures (data not shown).
Random forest modeling was used to assess the predictive value of child and parent characteristics on ankle and wristband wear time. Predicted performance characteristics of resulting models are in Supplemental Table 4. The ranked importance of input variables in the random forest models showed that children’s total daytime wrist wear was most strongly predicted by MCDI total language scores, the only variable which had a statistically significant association in regression methods (see Supplemental Figure 2). Moreover, for ankle wear time, the ECBQ effortful control score, shown to be negatively correlated with wear time, had the highest ranked importance in the random forest model (see Supplemental Figure 2).
Summarizing participant and researchers’ experiences
Finally, we summarized comments provided at-will by parents into the wristband diary, and the experiences of RAs “on the ground” facilitating the wristband activity, who offered a narrative summary of encountered issues.
Qualitative coding of silicone band diary comment section.
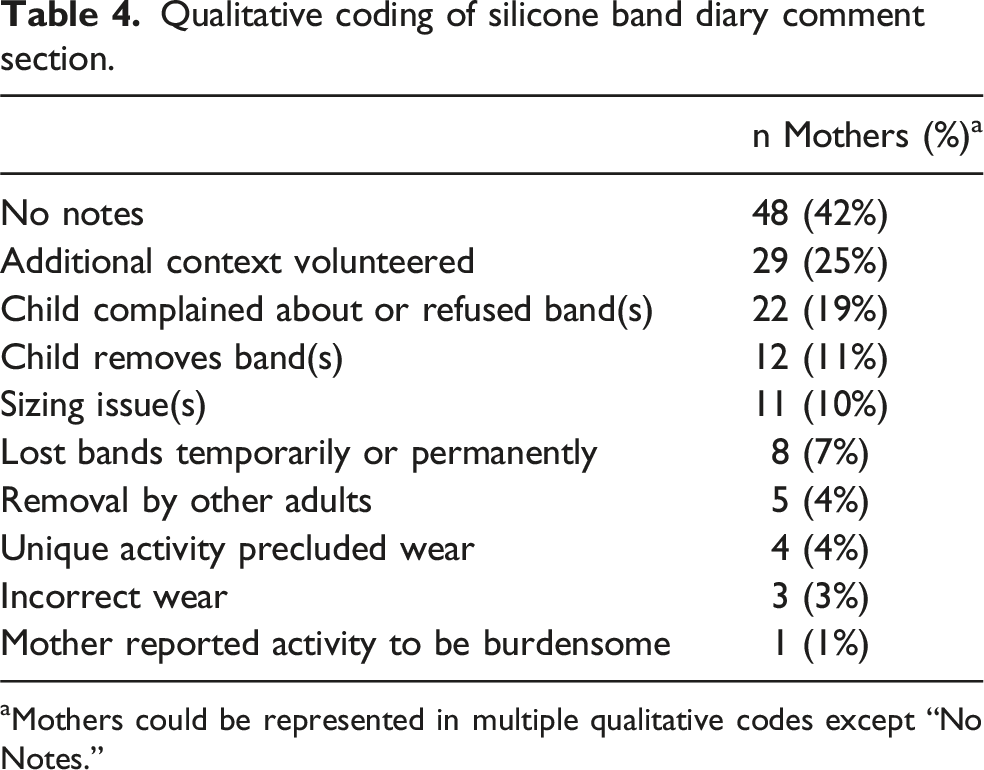
aMothers could be represented in multiple qualitative codes except “No Notes.”
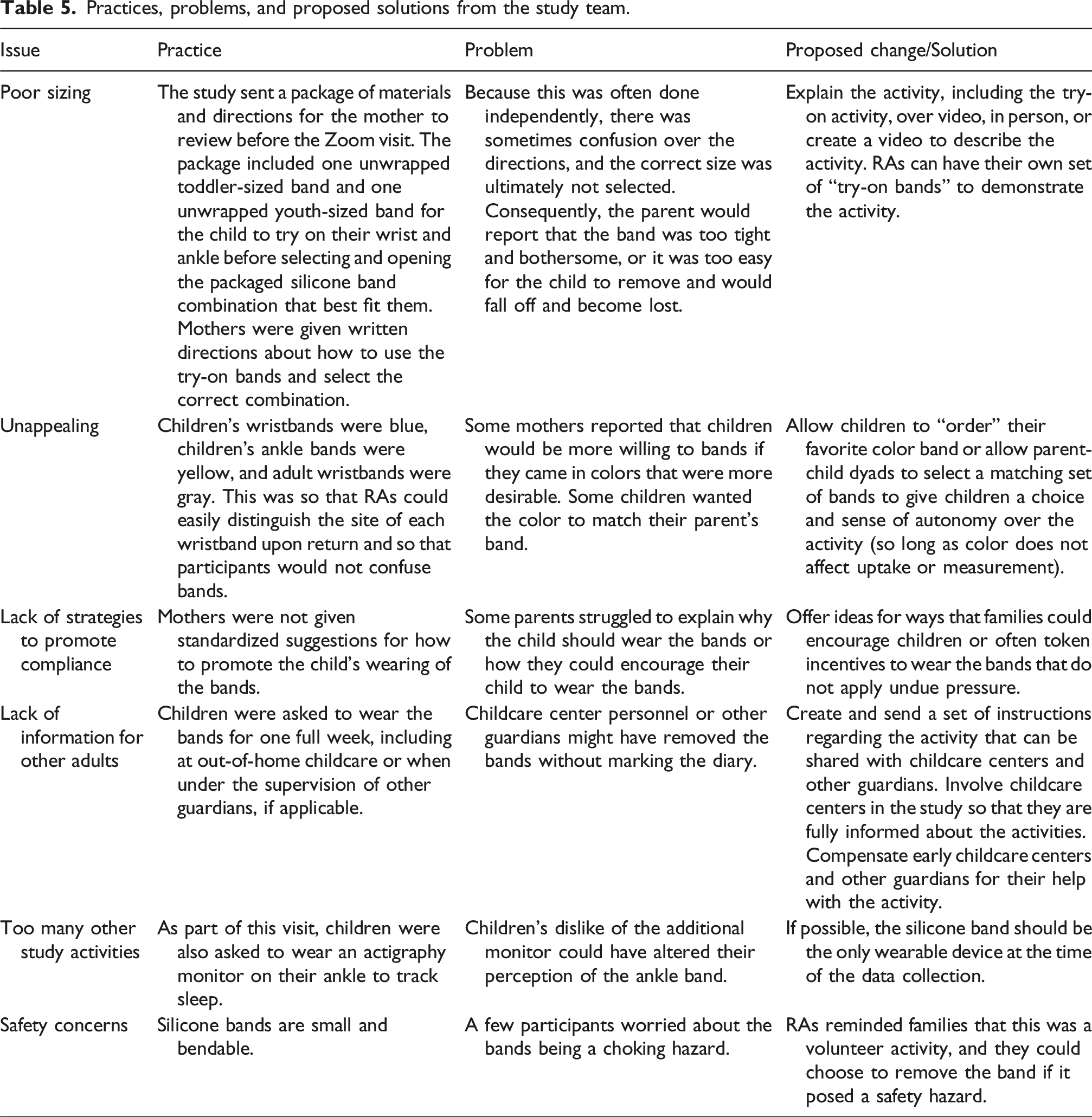
Practices, problems, and proposed solutions from the study team.
Discussion
Considering the increasing use of silicone band technologies as exposure monitoring devices, it is necessary to understand the feasibility of deploying silicone bands to young children as well as predictors of silicone band compliance. Our investigation explored (1) compliance with a weeklong silicone wrist and ankle band activity among children between the ages of 2 and 3 years old and (2) child and family characteristics that were associated with silicone band wear. Our goal is to inform future research interested in incorporating EC exposure characterization via silicone bands with young children, particularly for studies that seek to associate levels of ECs to child cognitive and behavioral outcomes. We found that (1) children were compliant and consistent with wearing the silicone band, particularly the ankle band, but that total days worn may not fully describe the child’s compliance with the activity; (2) several child-level characteristics (e.g., language, effortful control, behavioral inhibition) may be associated with children’s level of participation in the silicone band activity; and (3) sizing, appeal, and burden were common challenges nominated by parents and RAs on the ground. We discuss each of our main findings from this research in turn.
Children’s compliance with bands
First, as hypothesized, children tended to fall into one of two categories: those that were willing to wear at least one silicone band for most of the week and those that were unwilling to wear either band for any portion of the week. Nearly 80% of the children in our analytic sample wore the ankle band and 61% wore the wristband for a median of 11–12 hours during the day over the 7-day week. Kile, Scott 30 similarly found that 64% of their sample of 3–5-year-olds wore the silicone band (work on either the wrist or ankle) for seven days—though it is not clear whether days were counted if they were worn for part of the day or the entire day only. Comparing wear time to other studies that used silicone bands with early childhood samples is more difficult because of variations in data collection protocols 31 or the absence of detailed information on participants’ compliance with the silicone band activity. 29 If future studies are deploying only one silicone band with young children and desire a consistent placement, our results suggest that the ankle band will yield higher wear time than the wristband.
Notably, of the 130 participants invited to participate in the band activity, 15 were excluded from analyses due to their noncompliance with the activity as a whole—that is, they did not appear to attempt the silicone band activity at all (n = 13) or actively opted out of the activity (n = 2). While silicone bands are a noninvasive means of exposure assessment, the week-long activity in addition to other study activities may have been burdensome to some families. The silicone band activity was not a planned activity at enrollment (in mid-pregnancy); hence, this rate of total missing data may be higher than expected for studies with a planned focus on silicone bands.
We found wide ranges in total daytime wear (ranging from 0 to 84) within strata of total days (ranging from 0 to 7) that parents may have reported their child “wearing” the band (assuming that if the band was worn for at least 2 hours, the band was “worn” for the day). That is, there were instances in which children who wore the band for only 4 days had higher total wear hours than children who wore the band for 7 days. The current recommendation is to adjust chemical values by the total number of days worn (i.e., from 1 to 7). Chemical exposures may be underestimated among children who wore the band for fewer hours over more days. Our results suggest that researchers deploying silicone bands with young children should explicitly state what constitutes wear time for a day when asking caregivers to report on the number of days worn (e.g., at least 8 hours) or request that caregivers capture wear time in hours and adjust accordingly (see Supplemental Material 2 for our daily diary example).
Child and family predictors of compliance findings
We were encouraged to find that children’s age, sex, use of childcare services outside of the home, developmental delay/disability status, family socioeconomic status, and parenting stress were generally not associated with children’s wear time with either band. Families with lower socioeconomic status are at higher risk of EC burden, 58 and families with more socioeconomic and psychosocial stress are often disproportionately vulnerable to the toxic effects of ECs. 59 Our results suggest that disparities in EC exposures captured by silicone bands would not be explained by socioeconomic or social-stress related differences in band wear time. These results are consistent with prior investigation of wristband wear time among 3–5-year-olds, which found no differences in wear time (7 days vs < 7 days) by child age or family context (combining parent education, income, employment status, and the home learning environment). 30 We also considered that children may wear the bands for longer durations if they forgot about their placement due to long sleeves or pants; however, clothing choices were not associated with children’s daily wear time of either band. Only mother’s wear time of her own wristband was correlated with children’s wear time of the ankle and wristband. Observing their mother wearing her silicone wristband may have motivated children to wear their bands, and/or mothers who were wearing their own wristband may have been more consistent with ensuring that their child was wearing their bands. Future studies may employ “dummy” parent wristbands as a strategy to improve child compliance.
With respect to parent-reported child language, temperamental, and behavioral characteristics, we found that children’s total language scores were associated with higher daytime wear of the wristband (in hours and days). Children with more advanced expressive and receptive language skills may be better able to understand the activity and communicate their experience with the silicone bands, perhaps negotiating their wear time of the bands, yielding higher levels of compliance. Children’s (parent-reported) anxiety was associated with more days of wristband wear time, and children’s (parent-reported) behavioral inhibition was positively associated with children’s ankle band wear time (in hours and in days). Perhaps children who are more apprehensive are more likely to be cooperative, rule-followers. Parent-reported effortful control was negatively correlated with children’s wear time of the ankle band (in hours and days). Mothers who recognize that their child has lower levels of behavioral and emotional regulation may be more likely to monitor their child’s behavior, ensuring that their child is wearing the ankle band. Notably, several associations were attenuated when adjusting for age and sex. Future studies that are interested in examining the extent to which EC exposures captured via silicone band technologies predict child outcomes should be aware of our findings. If higher levels of ECs captured by the silicone bands are due to increased wear time (rather than truly higher levels of exposure), and wear time is not properly accounted for, associations between chemical exposures and child cognitive or socio-emotional outcomes (e.g., language, behavioral inhibition, and effortful control) may be biased. Hence, we encourage researchers to take special care to capture and covary the extent to which children are wearing the silicone bands during the study period.
Recommendations to improve compliance
Finally, we considered process-oriented solutions to improving compliance by reviewing comments made by parents on the silicone band daily diary and asking RAs who coordinated the activity to reflect on the challenges they encountered.
Parents and RAs agreed that inaccurate sizing was a challenge to child compliance; correcting sizing issues may also reduce the experience of accidental removals and lost bands. We attempted to circumvent sizing issues by providing toddler- and youth-sized “try on” bands with multiple combinations to choose from. Though RAs provide directions to the mother, visits occurred remotely, without the hands-on help of an RA. Future studies may provide in-person guidance or more detailed advice for what constitutes a well-fitting band, offer additional (smaller) sizes or bands that can be adjusted in size. Unfortunately, most adjustable bands currently on the market can fail or become brittle and break during the cleaning process.
Many parents reported a general unwillingness by their child to wear the band. RAs nominated the unappealing bands and lack of targeted strategies to improve compliance as common issues encountered. Allowing the child to choose their own color band may enhance children’s compliance by improving their interest and autonomy. In the current study, child wristbands were blue, and ankle bands were yellow; each were embossed to designate their positions, allowing researchers and participants to easily distinguish them. If studies only distribute one child band or identify other strategies to keep wrist and ankle bands in order, it may be feasible to allow children to choose their color; however, it is first necessary to understand if color influences chemical uptake or could bias measurements. Future studies may also employ strategies like (1) providing a token incentive or toy to children when they wear their band, (2) offering a small stuffed animal that has their own wristband and ankle band, or (3) offering fake bands for siblings to wear. These strategies may encourage children to wear their bands or reduce hesitation with the bands without coercion.
Several issues nominated by parents—removal of the bands by other adults, incorrect outfitting (sometimes intentionally, other times accidentally), and that unique activities precluded wear—may be resolved by offering additional information to parents about the activity. Given that parents were completing several post-visit activities, including actigraphy and sleep diaries, we opted to keep instructions and explanations of the silicone band activity brief (assuming that lengthy instructions would be less likely to be read). Studies with fewer parent activities, and especially those with a sole focus on the silicone band activity or EC exposure monitoring, may be able to go into greater detail about the wristbands and overcome misconceptions. Specifically, we suggest that future studies (1) provide information that can be shared with other caregivers, (2) make it exceptionally clear the importance of keeping wristbands and ankle bands in their respective locations, if that is a goal of the study, and (3) underscore that bands are durable and intended to be taken in any environment where it is safe to wear them (e.g., camping and swimming). Future studies may instruct parents to identify a week to complete the activity that does not include pre-planned, unique events that affect their willingness to wear the bands.
Post-visit activities for this remote toddler visit included an actigraphy monitor to be worn by the child for 7 days and nights (with a daily diary), a language monitor to be worn on the chest for 2 days (with a daily diary), and questionnaires. As such, RAs felt that children and mothers may have felt overburdened, contributing to their non-compliance or even refusal of the band(s). Future studies may limit the number of study activities that accompany the silicone band activity and/or reduce the length of the band activity in efforts to reduce burden on the participants and promote compliance.
Finally, an RA shared a concern about the silicone bands being a choking hazard; this sentiment was reported only once by a parent in the daily diary. Children who risk their safety by putting the silicone band in their mouth may need to withdraw from the study activity.
Strengths, limitations, and future directions
The study benefitted from the careful design and dissemination of silicone wrist and ankle bands, which enabled comparison of wear time between the two sites in a remote data collection setting. Specifically, wrist and ankle bands were differentiated by color and embossing, and accompanying daily diaries were designed to be user friendly. Although some parents reported sizing issues, we provided try-on bands and multiple sizing option pairs in a way that allowed us to understand which pairs were opened (and unusable for a future child).
We recognize that our qualitative methods were exploratory and informal; these methods were designed to capture practical insights to guide future research. Comments left by parents in daily diaries were consistently brief and direct, which facilitated their categorization into the coding scheme developed by study authors. Feedback from RAs were gathered informally rather than through a structured protocol. Nonetheless, these contributions reflect on-the-ground experiences and offer relevant solutions that can inform future research efforts.
We deployed the silicone band activity in a remote data collection capacity, wherein the activity was largely self-directed with minimal oversight. RAs reviewed the activity along with several other post-visit tasks with the mother over Zoom at the completion of the 90-min home visit. These additional activities, particularly the ankle actigraphy monitor, could have compromised the child’s compliance with the silicone band activity. RAs did not monitor the parent’s selection of the band sizes or check in with the parent during the week to trouble shoot challenges (though parents had RA contact info if they had questions). These limitations should be encouraging to future studies, as it suggests that even in remote settings with limited supervision and high levels of independence in a diverse sample, overall high compliance (particularly with the ankle band) with the silicone band activity in young children can be achieved. Closer monitoring of the activity is likely to yield even better results. Given that 64 children in our sample wore both the silicone wrist and ankle band for 72 or daytime hours over the course of the week, our next steps are to test the silicone bands for environmental chemicals of interest and test for differences in exposure levels between the two wear sites. Discordance in exposures detected between the two wear sites would support the deployment of both wrist and ankle silicone bands to provide a more comprehensive understanding of a child’s chemical environment.
It is important to note that daily diaries of child silicone band wear relied on parent-report and are therefore subject to reporting bias and social desirability bias. Parents were compensated for attempting any of the post-visit activities; children’s wearing of silicone bands was not a requirement for compensation. Still, parents may have over-reported band wear to appear more compliant. They may have also avoided using silicone bands due to concern over the results. Researchers should stress that accurate reporting to the extent possible will only make results more valid and informative for remedial purposes. Future studies may also benefit from explaining that chemical exposures are often colorless, odorless, and tasteless—even the most environmentally knowledgeable families encounter them daily. Finally, we did not follow-up with families who consented to participate in the activity but failed to complete any portion of their silicone band daily dairy about why they chose not to participate.
Conclusions
Valid quantification of EC exposure in the young child’s environment is a critical step in reducing the global burden of EC-associated diseases. Our study supports the use of silicone wristbands and ankle bands as feasible EC exposure monitoring devices to deploy with children ages 2–3 years old. Ankle bands were exceptionally well-accepted by the children in our sample. Though sociodemographic characteristics like age, sex, and family socioeconomic status were generally not associated with silicone band wear time, we found wear time of the wrist or ankle band to vary as a function of child characteristics like language skills, anxiety, and behavioral inhibition. This finding underscores the importance of tracking silicone band wear time to ensure compliance with the current recommendations of presenting time-normalized data. Strategies like deploying dummy bands for other household members, improving the sizing and appeal of bands, offering child-level incentives, and reducing the number of other study activities may improve participants’ experience, yielding even higher rates of silicone band compliance among young children.
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Supplemental material
Supplemental Material - Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children
Supplemental Material for Feasibility and recommendations for the use of silicone bands for environmental exposure monitoring in young children by Amanda C. Wylie, Jenna C. Frey, Allison C. Spring, Elise Hickman, Hadley J. Hartwell, Nicole Sagarnaga, Heather M. Stapleton, Sarah J. Short, W. Roger Mills-Koonce, Rebecca C. Fry, Cathi B. Propper, Julia E. Rager in Research Methods in Medicine & Health Sciences
Footnotes
Acknowledgements
We thank the participants and research assistants of the BEE Study.
Ethical considerations
Study was approved by the University of North Carolina Institutional Review Board (17-1914 and 21-1223). This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to participate
Adult participants provided written informed consent prior to enrollment and at every follow-up visit to participate in study activities. Adult participants also provided written parental permission for their child to participate in study activities.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by NC TraCS Institute 2KR1382107 and the National Institutes of Health (NIH) UH3OD023348, including the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD091148), and the National Institute of Environmental Health Sciences (F31ES034256, T32ES007018, F32ES036096 and T32ES007126). Further support was provided by the UNC Institute for Environmental Health Solutions (IEHS).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data and script are publicly available (see methods).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.