
Abstract
Models of positionality tend to focus on the researcher’s paradigm and how they interpret the world around them, but less emphasis has been placed on the concept of time as a methodological lens. The following commentary examines what it takes to embrace such an approach—making use of three components of positionality (identity, power and context) as a framework for examining qualitative inquiry. It is proposed that one of the conditions for validity in qualitative inquiry is for the researcher to embrace positionality as a moment in time. This approach will help qualitative health researchers make purposive methodological choices so that they can find an approach that is ‘right for them’ rather than ‘right per se’. Further, a model that outlines the components of methodological self-consciousness is offered, to support the qualitative health researcher in deciding the approach that is ‘right for now’.
Keywords
Introduction
Health is not static. It changes over time due to environment, lifestyle factors, trauma and aging, driven by physical, cognitive and social determinants.1,2 As time passes, we age, we grow, our bodies change, human factors become more complex, we become more mature, our knowledge base becomes broader and deeper, and our understanding and interpretation of events is enhanced. How a patient experiences the world changes over time. Likewise, clinicians change as they move through time: growing their knowledge, skills and understanding through experience, enquiry, and reflection. This lived experience means that clinicians will experience and understand the world in different ways as they move through time. When this lived experience is applied to qualitative health research it might be thought of as positionality. Typically, positionality can be thought of as recognising one’s own position and role within a research project such that the meaning of the research output can be contextualised. 3 While much has been written about the positionality and reflexivity of the researcher, this has not always been done so in alignment to temporal shifts in researcher identity. Simandan 4 identifies four epistemic gaps in positionality—possible world versus perceived world; perceived world versus current situation; current situation versus remembered situation; and remembered situation versus witnessed situation. This work addresses the third of these epistemic gaps and, through triangulating current debates on positionality, offers a template for the consideration of positionality as a moment in time.
Qualitative and quantitative research look like two very different worlds and the meaning participants ascribe to the phenomenon under study is either embraced or ignored.5–11 Further, because of the espoused rigour and validity of the (natural) scientific method, qualitative researchers have spent a long time justifying their methodologies to a positivist community who may never fully appreciate the ambiguities inherent in this paradigm. This has produced a rather ironic outcome, especially for clinicians involved in qualitative enquiry—who might feel like small islands surrounded by a sea of positivistic health studies—whereby an implied credibility problem in qualitative inquiry has led qualitative researchers to try to overemphasise the objective components of their work.12–14 This process has led to a reduction in the researcher’s agency, leading to a position where qualitative health researchers might do what they feel they are supposed to do rather than what their positionality tells them they should do. In addressing this tension to conform to external power, Cassell and Gummesson 15 recommend that qualitative researchers reflect on the ongoing relationship between identity and context and do what they feel is right rather than trying to mimic the actions of others. Since positionality is not a fixed commodity, qualitative health researchers should not simply use the same old research tools but revise their approach as their relationship with the environment develops. Here is it proposed that one of the tools for refining this interpretation is an examination of the role of time.
Positioning in qualitative research
The topology of time is generally shown as a line indicating the apparent consequential succession of events from past to future. 16 Humans experience time in a number of ways. At the daily level the suprachiasmatic nucleus of the hypothalamus acts as the central circadian clock regulating the body’s daily temporal functions. 17 More generally, time is experienced through aging, as indicated by functional, phenotypic and biological metrics (such as cognitive and physical function, fitness, muscle quality, cellular senescence and energy deficiency). 18 Time might bring decay, but it also brings maturity and wisdom. 19 Thus the perspectives of patients, clinicians and researchers are not fixed commodities, but are subject to the impact of experience. 20 Time changes perspective. In this way, the contextual knowledge that qualitative researchers develop through their experiences offers them the opportunity to view the same data through a new lens21,22; therefore, how we see and interpret the world as teenagers is very different to how we might do so during our retirement. The same data reviewed through the lens of time might lead to very different interpretations. In this way, we should see time as a descriptor of change and note that the impact of moving through time is a change in perspective.
Positioning theory challenges the essentialist views of identity as static and rooted in dominant individual and group characteristics—instead, emphasis is given to the “situatedness of identity”.( 23 , p. 166) It is suggested that we are not automatons following a research recipe in the hope that the right mix will lead to the right outcomes—instead we should consider ourselves as agents and authors of social interaction, whose situation is constantly under change. Such situational change brings with it a new perspective. Thus, what is ‘correct’ at any given time is not necessarily ‘correct’ forever. This can be demonstrated in the work of clinicians, where the latest guidelines, procedures and approaches are adhered to, and where practice is constantly updated. However, since there is no policy guidance on qualitative research, clinicians might not feel the same need to revise their methodological lens.
Positioning allows for the subjective reality of each individual (and the multifaceted dimensions that make up their identity) to play a critical function in the production of human understanding.24,25 Reflexivity then becomes a continuous introspective process that runs throughout the qualitative research process where the key is not to remove bias but to “to make the relationship between and the influence of the researcher and the participants explicit”.( 26 , p. 45) Hobson 27 suggests that since the located expert within the researcher cannot be extracted, then their subjective knowledge, skills and behaviours should be used rather than removed. Discussion on identity tends to focus on the facets of personhood but since identities “move, grow and develop, and different aspects of identity come to the fore at different periods of time”( 23 , p. 167) there is much to be gained by considering positionality in relation to the moment in time when the research was undertaken and the perspectives of the researcher at that time.
Researcher identity
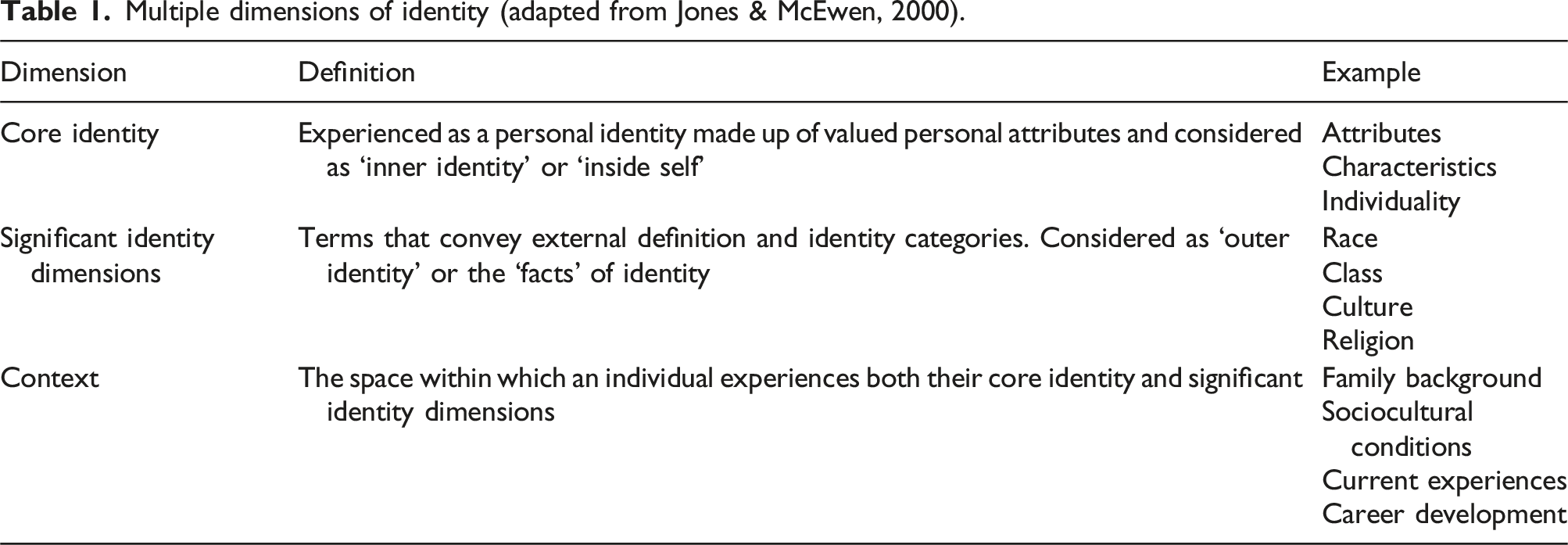
Multiple dimensions of identity (adapted from Jones & McEwen, 2000).
The competing identities within the researcher and within the researched can be captured and controlled only if we conceptualise research as a snapshot in time but, as we step outside this time bubble, we find that time has given us new “shifts and contradictions”( 29 , p. 5) that alter our lens of understanding. Anthias( 30 , p. 498) refers to this altered lens as a “narrative of location [that] tells a story about how we place ourselves in terms of social categories such as those of gender, ethnicity and class at a specific point in time and space”. Qualitative research can, therefore, only produce partial truths if it is not aligned with an understanding how our situation in time and our life experience impact upon our positionality. 31
Simandan 4 offer four epistemic gaps regards to positionality. Firstly, that an individual’s personhood means that each of us experience slightly different worlds. The second gap states that we can never fully appreciate a situation as we only ever have a location-specific understanding of it. The third epistemic gap highlights how people change over time and how this change affects our memories of the past and our interpretation of previous and current facts. And the fourth epistemic gap focusses on the nature of understanding being a social construct. There is not space or time to fully explore these epistemic gaps in this paper, but the third gap aligns to its overall thesis, as highlighted in Simandan’s question, “is a person a spatiotemporally stretched entity or are we different persons at different slices in time?”.( 4 . p. 137) Using this conception, it is argued that the tools used for qualitative health research should not be employed in a naive manner—rather they should be positioned so that the researcher can find an approach that is ‘right for them’ rather than ‘right per se’. Further, the qualitative health researcher should consider what is ‘right for now’.
Being ‘right’ in qualitative health research
Research itself is a value-laden activity, and the pursuit and analysis of data is saturated with epistemological and ontological assumptions. 32 This means that there is a possible tension between the desire to draw meaning from data and the perspectives of the individual researcher. The ‘right per se’ approach in this instance might be for the qualitative health researcher to turn to their textbook and find what the literature deems to be the best method to theme and code their data and rely on that recipe to give rigour to their work. Thus, validity becomes an outsourced commodity, and the positionality of the researcher is negated. The ‘right for them’ approach would be for the researcher to examine their own positionality. Recognising the relationship between the whole of a research project and the individual researcher involves being methodologically self-conscious—a condition where the underpinnings of research are “as much about choosing a tape-recorder as reading Habermas”.( 33 , p. 32) Finally, in considering what is ‘right for now’, qualitative researchers should reflect on their positionality, not as a fixed point but as a socially produced construction developed through the interplay of context, meaning and time. 24 Reflecting on what is ‘right for now’ means embracing the researcher’s multiple and developing identities as being “contingent on time and space in the field, thus making them contextual and contestable, rather than static”.( 34 , p. 555)
Components of positionality (adapted from Kezar & Lester, 2010).

Identity
Identity is not a fixed commodity rather it is a “dynamic, self-organizing system”( 35 , p. 5) and the conceptualisation of identity is multi-faceted. As Kroger( 36 , p. 34) points out “[a]t times, identity refers to a structure or a configuration, at other points it refers to a process. Still on other occasions identity is viewed as both a conscious subjective experience as well as an unconscious entity”. As individuals we have multiple identities which are determined by our core identity (e.g. our manner) and our significant identity dimensions (e.g. our gender) and by life experiences (e.g. our career path). These multiple identities impact how we see ourselves and how others see us.37–40 Working in inter- and multi- disciplinary teams, means that clinicians are constantly negotiating the many personalities of the many people they work with. This same negotiation can be applied to qualitative research.
For qualitative health researchers, identity does not only impact how we understand ourselves in relation to the situation under study it also determines the practical aspects of the research process, from the nature of the questions; to the selection of literature; to the design of the data collection tools; to the unpicking of findings; to the pulling together of recommendations. None of these activities is a neutral act, they are all tempered in individual bias. This bias is a function of one’s position in time and current perspective, where the researcher must consider what is both ‘right for them’ and ‘right for now’. But rather than assuming that bias is a negative factor that the researcher must work to correct a methodologically self-conscious approach examines the nature of this bias and even seeks to find strength in it. Humberstone 41 notes that the researcher’s personal experiences, feelings, emotions, and knowledge of situations are significant in understanding different contexts and that having the examined self at the centre of a research project not only problematises that data but problematises the lens through which the data is examined. In this way, the individual, current perspective of the qualitative researcher can be embraced. A similar message can be found in patient data, where patients see the benefit of care at an individual level and patients can identify the characteristics of various clinicians that they feel are right for them at a particular moment in their care.42–44 Therefore, identity can be described as a positive phenomenon with core characteristics wrapped in many different layers that change over time. 45
Power
Epstein( 46 , p. 20) reports that “truth is constructed by social processes, is historically specific, and is in part shaped through the power struggles within a community”. From this perspective it is important to recognise that these meanings are often constructed through an “active, cooperative enterprise of persons in relationship[s]”.( 47 , p. 15) If qualitative health research is to rely on the participants’ views of the situation under study, then the lens through which data is examined needs to be examined for its capacity to tell participants’ truths. Taking an inductive approach to this truth-telling process means that the “primary purpose [of qualitative research] is to allow research findings to emerge from the frequent, dominant or significant themes inherent in raw data”.( 48 , p. 1) But it is the researcher who creates the conditions for these themes to emerge and whose life history creates the (current) narrative lens through which to draw meaning.21,22,30
Jamal and Hollinshead( 49 , p. 65) report that, qualitative research involves “a bricoleur… a kind of do-it-yourself persona” whereby, “the qualitative researcher selects from the rich array of methods, tools and practices available, in order to address the research question(s) and assumptions”. The researcher then constructs a “complex, dense, reflective, collage like creation that represents the researcher’s images, understandings, and interpretations of the world or phenomenon under analysis”.( 50 , p. 3) In this bricolage, power is central to the way that researchers make meaning. 23 Thus, meaning is not something that is found, rather it is something that is constructed, and the tools of its construction are decided by the researcher.
Throughout this construction of meaning, different dynamics of power exert themselves and impact on the positionality of the researcher. For example, many qualitative researchers seek to redistribute the power between themselves and their participants, offering empowerment and agency to the researched. 51 But much as the balance of power between clinicians and their patients’ needs to be carefully nurtured, there needs to be careful nurturing of the balance of power between qualitative heath researchers and the researched. For example, the ability to develop purposeful relationships with patients is not always something that comes naturally. Some novice clinicians may find difficulty in supporting older, more assertive patients, and may find themselves relying on experienced colleagues. Here inexperience may limit the novice clinician’s ability to fully support a particular patient. The same is also true of qualitative health research, where the novice researcher does not feel fully empowered to make certain decisions or feels that their participants will perceive this inexperience and that this might impact the resultant data. Both these positions of power are time dependent as the clinician’s experience may help them overcome interpersonal power hierarchies and, over time, they will learn ways to reduce and allow for more equitable access to all participant research groups. But, at the particular moment the researcher attempts to construct meaning, their positionality will be impacted by their previous and current relationships with these power dynamics. In these examples, the impact of time is felt and what is ‘right’ at one point in time is not necessarily ‘right’ at another.
The classic model of reliability through triangulation imagines that the truth of research is to be found in a Venn diagram of results – but this seems to place great emphasis on the products of triangulation rather than the processes of triangulation. A methodologically self-conscious approach to qualitative research recognises that there is more than just interconnected points of data from which to construct meaning and that the lens through which data is interpreted is dependent on current power dynamics. In constructing meaning, qualitative health researchers should consider how the situatedness of their current perspective and their research choices are dependent on their place in time and their power relationships with their context and their participants.
Context
Denzin and Lincoln 52 define qualitative research as a situated activity that embeds the researcher in the social world, but this social world is not a fixed commodity. Thus, the ‘narrative of location’ is the story of how the researcher has been influenced by their context and how this has led to the current interpretative lens they apply to their context. 30 Qualitative health research thus consists of a set of interpretative practices that help us make sense of the world but our capacity to make meaning of social reality is constantly changing as a result of experience. Thus, positionality is also context dependent. 53
From an interpretative point of view, reality is not something out there that a researcher can easily explain or translate into a research report or thesis. The relationship between identity and context shifts through time and choices regarding what is ‘right for me’ and ‘right for now’ are always “mediated through the researcher”.( 48 , p. 40) Of course, this does not mean that the world is not real, but rather that we can only experience it “through our perceptions which are influenced by our preconceptions, beliefs and values”.( 54 , pp. 21-22) In drawing together the meaning that is found in qualitative inquiry, Foote and Bartell( 31 , p. 46) report that it is “important to illuminate that one’s life experiences inform researcher viewpoints, which therefore are positional—they are partial truths, at times oppositional, and they acknowledge that researchers themselves exist within socio-cultural, political, and historical contexts”.
Pope, Ziebland and Mays 55 suggest that different researchers may interpret the same data in different ways because the act of interpreting data is imbued with individual qualities. The same is true of the generation of qualitative data where individual participant accounts cannot be held to universally represent the whole of the answer. The imbuing of such interpretative qualities is a function of the relationship between the researcher and their context over time. Further, Kitzinger 56 argues that even the process of listening to what participants say is not a straightforward task as meaning-making during data collection is also at play with all parties interpreting and re-interpreting meaning in line with their own epistemological and ontological biases. Thus, the generation and interpretation of qualitative data is a subjective process where “different people in different places at different times, interpret things differently”.( 57 , p. 103)
In their review of literature, Yeh and Inman 58 found six strategies for interpreting qualitative data. They discuss the role of the self, culture, collaboration, circularity, trustworthiness and deconstruction as filters through which the research process and data are passed. From this perspective, qualitative researchers tend to embed themselves in the social situation to be studied, to closely connect with the people within the study and to try to attempt to see things from their viewpoint. 59
Triangulating current positionality models
Much discussion on positionality has been focussed on biography, place and the researcher’s relationship with the research process. This has led to a conception of positionality that is focussed on the underlying ontological and epistemological orientations of the researcher.60–62 However, the temporality of the researcher is not discussed with due regard to identity. Where discussion has recognised that the interpretation of data is temporarily situated, there is a gap in relation to how the dimensions of identity factor into this interpretation.4,61–63 In drawing together discussion on the dimensions of identity (core identity, significant identify and context) alongside the literature of the components of positionality (identity, power and context) we can see that there is an unexplored nexus that, when combined with Simandan’s third epistemic gap (people change over time and this change affects our memories of the past and our interpretation of previous and current facts), offers scope for a new template for the consideration of positionality as a moment in time. Drawing together these factors allows us to see that understanding oneself as a qualitative health researcher is a process of being and becoming over time.
Discussion
Creswell 9 suggests that validity in qualitative research is often influenced by the researcher’s constant scrutiny, so it is worthwhile scrutinising how strategies for interpreting qualitative data are positional. Since human beings are meaningful actors, researchers should aim at uncovering the meanings that motivate their actions and should reflect on how the situatedness of their identity is a function of their shift through history. 23
Positionality and identities are not static, they grow and evolve over time. 38 Some aspects of identity are more fluid than others. For example, personal aspects such as gender, race and nationality are not matters of choice, they are identities that we are born into. But other social aspects of identity—such as, status, parenthood and occupation—have greater capacity for change. Both the personal and social aspects of identity exist within the wider context of time. Social aspects of identity clearly change over time as migrants become workers, people marry and divorce, students become qualified, and some stereotypes are overcome. Whilst core identities will not change over time, they will be differently affected by the changing context that they find themselves in (evolving examples of this can be seen in relation to equal pay initiatives and the Black Lives Matter movement).
Power is a social construct that impacts upon the relationship between the researcher and the researched. Qualitative researchers tend to embed themselves in the social situation under study, to connect with the people within the study and to try to attempt to see things from their viewpoint—attempting to reduce power hierarchies—but participants will still view the researcher in certain ways. 59 As the researcher’s identity shifts, this power relation will also shift, allowing a senior clinician to create a different power dynamic with patients than their junior colleague might.
Data gathering and data interpretation are not neutral acts that can be replicated by a researcher at different phases of their lives. These actions are contingent upon the layered facets of identity, power relationships and contextual factors. Researchers do not have a fixed and homogenous lens with which they view all data—the lens of inquiry is constantly reformed through identity shifts that are contingent on time.22,29,34 Therefore, drawing on Jones and McEwen
28
and Kezar and Lester,
23
a new model of methodological self-consciousness is offered—one that embraces reflections on what is ‘right for me’ and what is ‘right for now’ (see Figure 1). Components of methodological self-consciousness.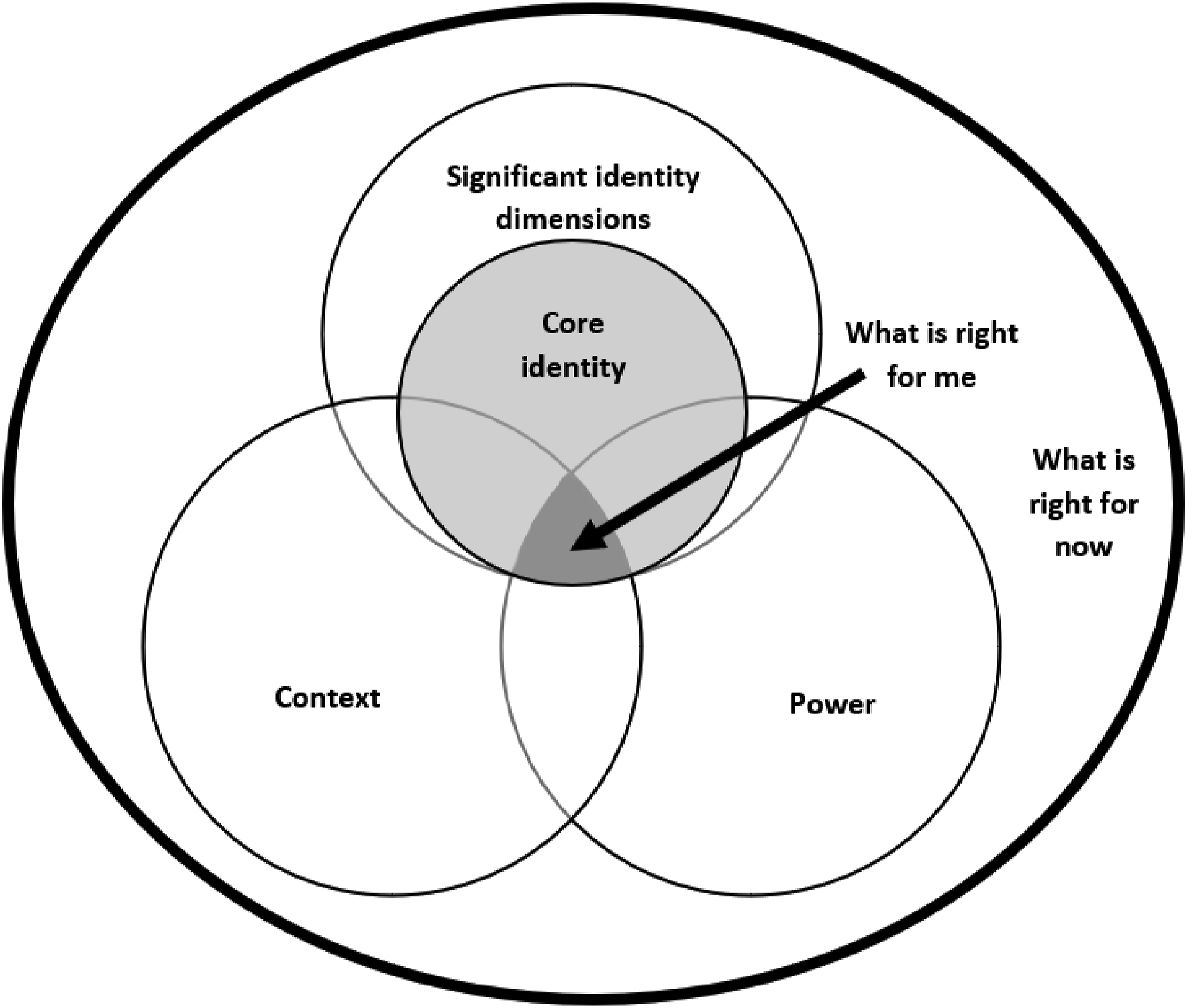
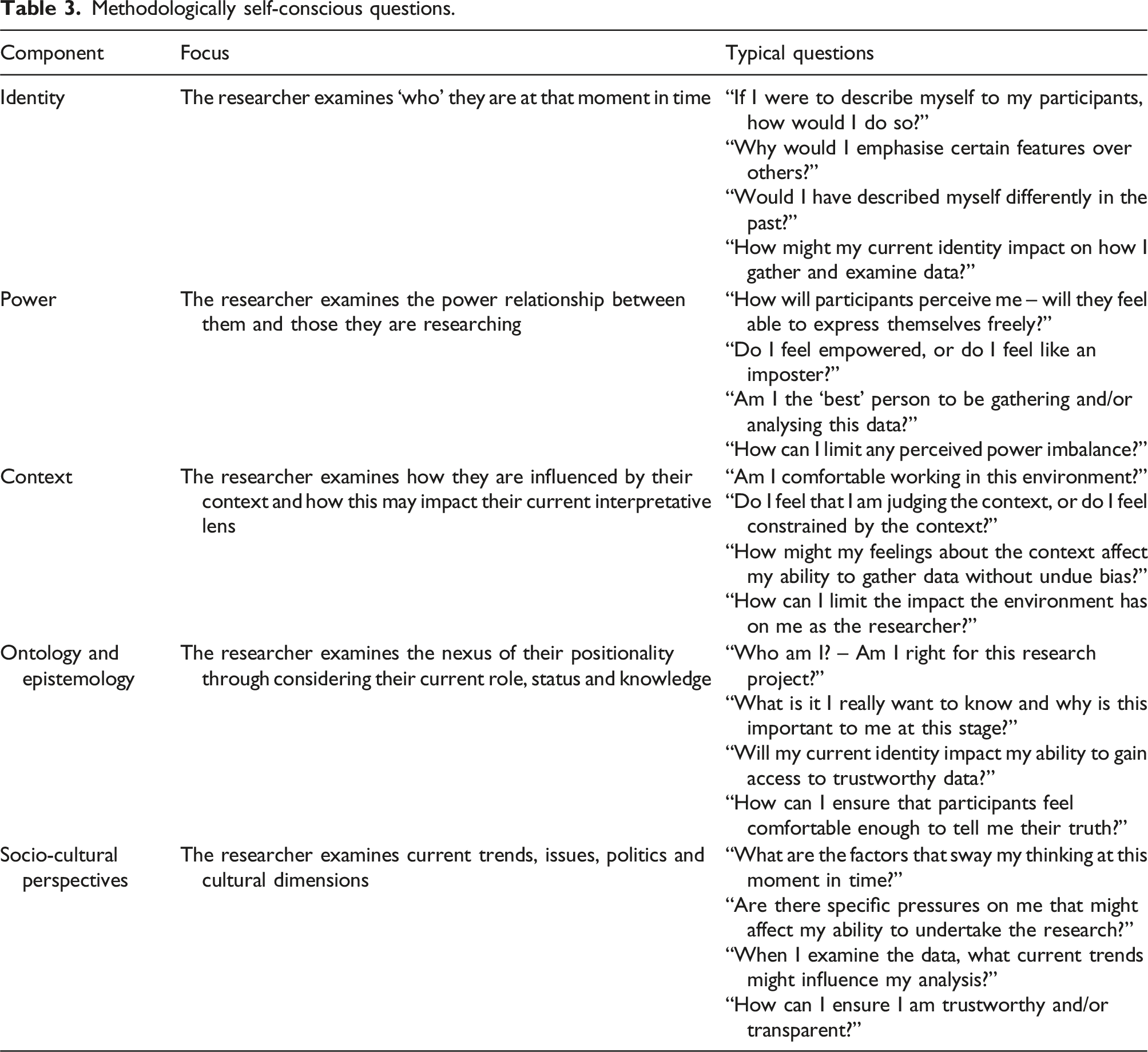
Methodologically self-conscious questions.
Conclusion
Qualitative health researchers should be encouraged to reflect upon whether their preferences are biases that need corrected or whether they should see positionality as a beneficial and legitimate aspect of research. Some aspects of positionality will give greater access to certain participants, and some may place barriers in the way. Time and experience will also offer the researcher guidance into what might work for them (in terms of the identity as a researcher and their personal aspects of identity). Who we are and how we perceive ourselves will impact the choices we make. Therefore, we might look for a balance between following the processes of research; doing the things that we feel would be best for the research itself and doing the things that we want to do because we feel that our agency will offer a new type of rigour. We might also reflect upon how our current identities impact upon these research choices, and how our identities are likely to impact differently in future.
A researcher’s bricolaged identity is fundamental to data gathering and data interpretation but as their ‘narrative of location’ changes their access to certain approaches will change.23,30 Being methodologically self-conscious is a process of working out what is right for a specific moment in time. What worked for a young medical researcher might not work for a busy consultant. Epstein( 46 , p. 20) reports that “truth is constructed by social processes, is historically specific, and is in part shaped through the power struggles within a community”—thus finding the ‘truth’ of any situation will involve different approaches at different points in history.
Qualitative inquiry is not the search for the answer but is a search for an understanding. In offering guidance on how to find the answers that lie within qualitative data many textbooks focus on leading the reader through the processes of research. Thus, research is presented as a recipe to be followed rather than a process of personal enquiry. Focusing on the processes of research means that the perspectives and preferences of researchers have come to be considered as secondary, subjective and unscientific. This has led to a situation where qualitative researchers might overlook the importance of their own identity, skillset and their own choices.13,14 Understanding the examined self is central to understanding the situation under study but this examination of self is not a one-time activity. 41 The tools used for qualitative health research should not be employed in a naive manner—rather they should be positioned so that the researcher can find an approach that is ‘right for them’ rather than ‘right per se’. Further, the qualitative health researcher should consider what is ‘right for now’.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.