
Abstract
Introduction
The prevalence of sexually transmitted infections (STIs) among MSM (men who have sex with men) and transgender women (waria) in Bali is of significant public health concern. According to the 2015 Integrated Biological and Behavioural Survey (IBBS), HIV prevalence among MSM in Denpasar (the capital city of Bali) was 36% – the highest prevalence in this population reported nationally. In addition, 26% of MSM and 25% of waria in Indonesia were living with HIV in 2015. There is limited research examining the attitudes, behaviours and experiences of MSM in Indonesia, and specifically in Bali. This study will develop a model to help understand the social-cultural context, attitudes, behaviours, and experiences to inform interventions to increase safe sex practices amongst Indonesian MSM and waria who live in Bali.
Methods and analysis
The community-engaged research (CEnR) study, employing a sequential mixed-methods approach, will engage MSM and waria community throughout all five phases. The first two phases will include partnership building and exploratory research (focus group discussions/FGDs). Phase three will include the administration of a survey (n = 374 Indonesian MSM and waria). Phases four and five include explanatory (in-depth interviews) and dissemination phases, respectively. Multivariate analysis will be employed for the quantitative data (the survey) and thematic analysis will be used to analyse the qualitative data (FGDs and in-depth interviews).
Discussion
The findings of this CEnR will inform culturally congruent interventions for organisation working with MSM and transgender to promote safer sexual health practice and improve general well-being of this community
Strengths and limitations of this study
• This CEnR project will be conducted as ‘participatory research’, presenting substantial challenges including working with a marginalised population, managing bias and retaining confidentiality and anonymity. • The mixed-methods approach will add to the literature on the use of CEnR in marginalised populations. • Using exploratory and explanatory phases within CEnR, this study will ensure issues relevant to MSM and waria are explored and rich data are gathered to enable a sound understanding of attitudes, behaviours, and experiences of MSM and waria in Bali, Indonesia as well as ensuring the research outcomes are culturally congruent. • The recruitment of the respondents in phase 3 of this project will include partner-driven and online sampling, which may under-sample isolated MSM and waria and those who do not have access to the Internet.
Introduction
Bali is an island and a province in Indonesia comprising 5780 square kilometres with an estimated population of over 4.2 million people. 1 The island is home to the largest Hindu minority in Indonesia with approximately 83.5% of the population following Balinese Hinduism. Other religions practiced in Bali include, but are not limited to, Islam, Christianity and Buddhism. Traditionally, Balinese Hinduism has recognised homosexuality since ancient times and is celebrated in traditional practices including ceremonies and performances. 2 Bali is a popular tourist destination with attractive beaches as well as highly developed arts and culture. 3 Many expatriates live in Bali with an estimated 30,000 people originating from other Indonesian islands and other countries. 3 The number of MSM in Indonesia as estimated by the Indonesia Ministry of Health 4 is to be around 1.2 million with more than 14,000 living in Bali. The Bali AIDS Commission also estimated there were 650 waria in this province. 5
MSM include those who identify as gay and also men who engage in sexual activities (e.g. by hand, anal sex and/or oral sex) with men without self-identifying as gay or transgender. This may include male sex workers, bisexual and heterosexually identifying men who have other partners (male and/or female) or a wife. 6 The term waria originally comes from the combination of wanita (woman) and pria (man) terms which are roughly similar to ‘male transvestite’. 7 The term waria is complex and has a range of different interpretations. 7 Waria does not only include ‘men who imitate women in their clothing styles or mannerisms while retaining a masculine identity’ as stated by Dede Oetomo nearly 20 years ago, but has a broader definition based on Indonesian culture. 8 In some parts of Indonesia, waria belong to the third gender, 8 while in many parts they are assigned as men. 7 Others have defined waria as males who become and dress like females in order to provide financially; and, who tend to work as hairdressers, entertainers and sex workers. 9 The WHO recognises waria as a specific indigenous term in Indonesian culture ‘to describe people who form same-sex relationships and those who exhibit non-binary gender identities’. 10
Since the early 1990s, MSM and waria have been identified as key populations for STIs and HIV surveillance along with people who inject drugs (PWID) and female sex workers (FSWs).9,11 The Indonesia Health Profile 2016 reported that 26.1% of 41,250 newly infected PLHIV in 2016 were MSM. There was an increase of HIV/AIDS amongst MSM from 2011 to 2016, with this group being the second highest high-risk behaviour group after the heterosexual group. According to the 2018–2019 Indonesian integrated HIV biological behavioural surveillance (IBBS), national HIV prevalence was 17.9% and 11.9%, and 2,1% among men who have sex with men (MSM), and waria respectively. 12 Furthermore, studies have found HIV prevalence amongst MSM in Denpasar to be 36.0% 13 and to be 18.7% amongst gay men and 40.9% among transgender people in Bali. 14 The main transmission risk behaviour of reported HIV cases in Bali from 2011 to 2015 was from homosexual (20%) and heterosexual (76%) intercourse. 11 Until 2019, it was reported that among the HIV new cases, 76.4% were associated with heterosexual and 14.2% with homosexual transmission. 15
A recent survey conducted in Bali amongst the MSM and waria community (Indonesia Sexual Health Survey (SekSI) study 2018) found 20% of respondents (142/709) reported having had sex with female partners in the last 6 months. Of these, 48.6% had sex without condoms. 16 Further, 15% and 28.1% of respondents had sex with sex workers and sex workers’ clients, respectively, in the last 6 months. Of these, 48.1% of those who had sex with sex workers and 42.2% of those who had sex with sex workers clients had condom-less anal intercourse (CLAI). Sex work was the main income for 44.6% of waria and 8.3% of MSM. 16 This study highlights the risk of HIV and STI transmission among MSM due to the proportion of participants reporting multiple sex partners and unprotected sexual intercourse. MSM reported having sex with their female partners, casual partners, and sex workers, highlighting the significance of sexual health risks outside the MSM community.
Research conducted in Bali among MSM and waria communities has largely focused on prevalence and sexual behaviour. This includes a prevalence study 5 ; the IBBS survey in the capital city of Bali 12 ; HIV biomedical and behavioural survey in all districts in Bali 16 ; and research on pre-exposure prophylaxis use awareness. 17 To the best of the authors’ knowledge, while these studies explored behaviours of MSM, data exploring the attitudes and experiences of MSM living in Bali were not collected. 16 Research is needed to understand the unique MSM and waria population in Bali, especially those who do not openly identify as gay or waria. Moreover, research formally adopting a community-engaged approach among these populations in Bali has never been conducted. While other studies have engaged the community during recruitment,12,16-18 to our knowledge this is the first study among this target group in Bali that formally engages community members throughout the research.
Before developing health promotion interventions, it is critical to understand the sexual risk behaviours among specific groups and barriers to practising safe sex behaviours.19-22 The complexity of the issues faced by MSM and waria, along with increasing stigma and discrimination against MSM, waria and HIV positive people, in Indonesia, is significantly slowing the country’s response to HIV infection; 23 therefore, it is important to understand the socio-cultural aspects of safe sex practices to inform the development of STIs and HIV behaviour change strategies20,24,25 and the influence of community/social norms risk reduction on MSM behaviours. 24 Understanding attitudes, behaviours, and experiences of MSM is necessary in order to develop a culturally appropriate prevention program. 24 Engaging MSM in the research will provide a better understanding of the social-cultural perspectives and sexual practices specific to HIV in Bali. 14 Involving MSM and waria as research partners during this study is intended to ease the complexities influenced by culture or geographical locations and issues faced by MSM and waria in Bali.
The findings of this study will inform policy and intervention development including recommendations for the development of specific, culturally appropriate health promotion programs designed with the community to give and place MSM and transgender the proper way to prevent HIV and other STIs infections, which indirectly (if applicable) will also prevent sexual communicable diseases to the broader community with the ultimate aim of slowing the epidemic of STIs and HIV amongst the MSM community in Indonesia.
CEnR has been employed in trials in clinical settings, 26 and developing public health initiatives (translational research) however these studies have not used a mixed-method approach. 26 Little has been published related to the used of mixed-methods design within CEnR. Furthermore, including a multi-sectoral partnership is also a focus in CEnR. 27 This project will add to the literature regarding the use of sequential exploratory explanatory mixed-methods design within a CEnR project and will provide a grounding for further research and model development in other settings and populations. The social model to be developed as a result of this study will help understand attitudes, behaviours, and experiences of MSM and waria in Bali and will inform guidelines, policy and practice for stakeholders and organisations working with MSM and waria to promote safer sexual health.
Aim and objectives
This CEnR aims to explain attitudes, behaviours, and experiences of MSM and waria in Bali to inform sexual health policy and practice for this population group. Specifically, the objectives are to: 1. Explore factors that influence sexual health attitudes and behaviour including the enablers and barriers among MSM and waria in Bali. 2. Develop a model that conceptualises sexual health attitudes, behaviour, and experiences among MSM and waria in Bali in detail. 3. Explore experiences of MSM and waria in Bali including stigma, discrimination, and mental health. 4. Provide recommendations for the development of strategies or interventions to improve safer sex behaviours among MSM and waria in Bali.
Methods and analysis
CEnR enables a deeper understanding of health-related phenomena and actions relevant to specific communities.26-29 This is achieved through the involvement of the community in the research process ensuring the research is culturally congruent.26,27 The process of engagement commences at the beginning of the research and the community may be involved in prioritising or defining the community’s problem, developing research tools or methods, engaging in data collection, analysis, dissemination and publication of the research findings. While involvement does not necessarily have to be as equal as the researcher, it should be as significant as possible as the insiders’ perspective will help the researcher in designing effective recruitment strategies, culturally congruent data collection and suitable venues and modes for dissemination.27,28
Public health research aiming to solve complex problems in social and environmental systems involving interrelationships between families, communities and society has previously employed CEnR.
26
The approach allows for the exploration of a range of determinants, recognising the complexity of interactions that impact social, emotional and physical health.
26
This project will employ moderate engagement of the community members whereby community provides input into research questions, research design and contributes actively in the research (see Phase 1). A sequential exploratory–explanatory mixed-method design will be employed. Figure 1 provides an overview of the CABE project phases and methodology. The interrelationship between the five phases of the CABE Project.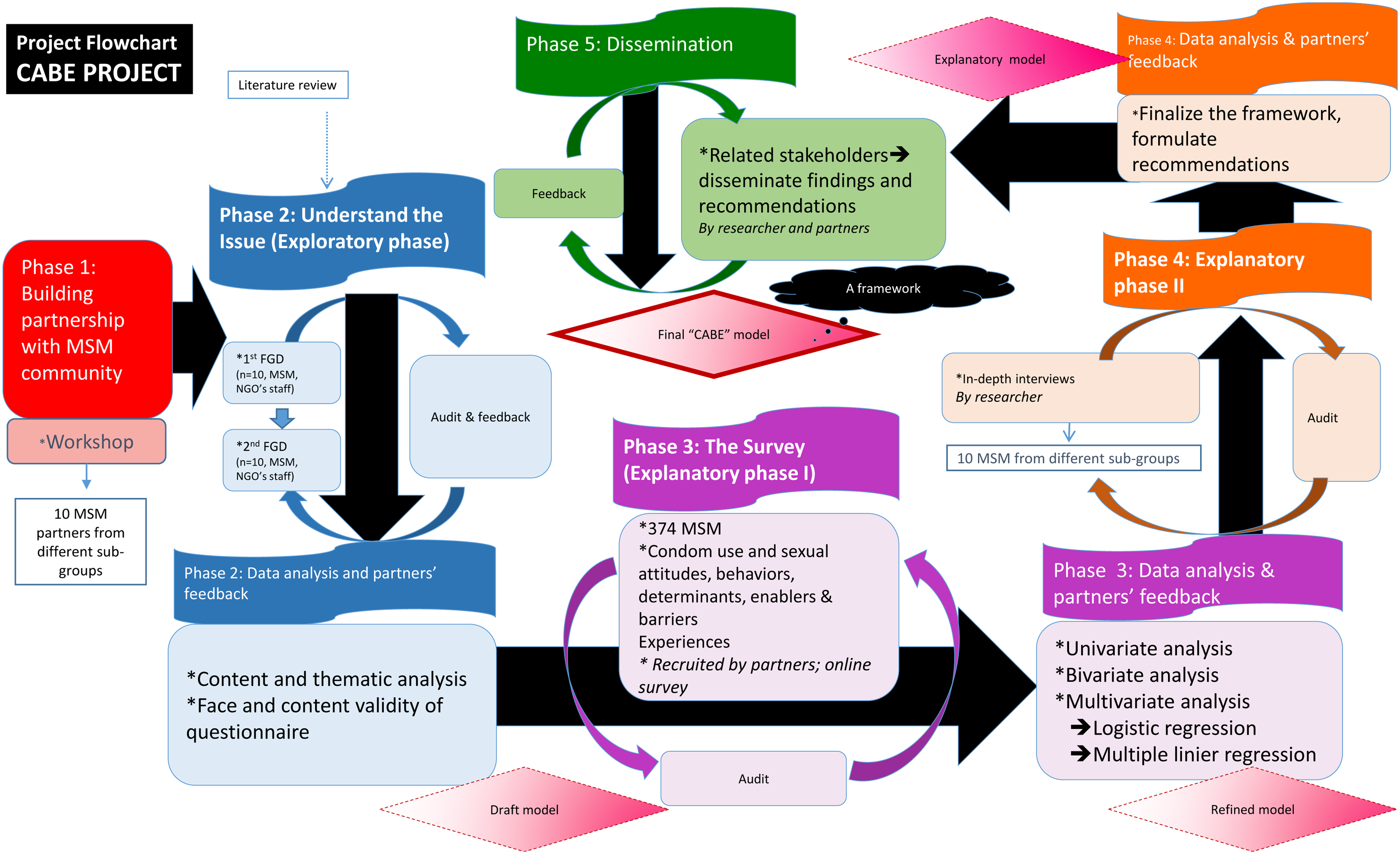
This mixed methods research will employ multivariate analysis to interpret quantitative results using SPSS. 30 Thematic analysis will be conducted for the qualitative part of this research. NVivo will be used to manage and assist analysis of qualitative data. 31
Phase 1
Phase one involves the establishment and development of partnerships with non-government organisation (NGO) staff who are also MSM and waria. NGOs throughout Bali that focus on sexual health are accessed by MSM and transgender. The organisations have the capacity to reach hard-to-access groups. Therefore, partnership with staff that works with these groups will be established. In Bali, government agencies refer to NGOs for sexual health information. Further, both government and NGOs are in collaboration when delivering health intervention which is most commonly implemented by NGOs. There is a chance recruitment of MSM and transgender people for this research from very remote areas will be difficult; this will be acknowledged as a study limitation. Participating staff will comprise approximately 10 MSM and waria who come from different sub-groups. Consideration will be given to recruiting Balinese born as well as Indonesians born outside Bali. This will enable the views of Balinese and non-Balinese Indonesians to be heard. The partners will be invited to a one-day workshop which will include the opportunity to: 1. Develop a good rapport and relationship with partners. 2. Discuss the project, the researcher and the partners' roles. 3. Discuss the recruitment methods for the survey and in-depth interviews. 4. Discuss health issues around MSM and waria’s attitudes and behaviours. 5. Partners to contribute to the development of interview guide (for Phase 2) and the questionnaire (for Phase 3).
The one-day workshop (6 hours) will allow for engaged interaction which is necessary community engagement. This will allow the researcher develop a rapport with the partners and for partners to contribute to the program. The length of the workshop will be alleviated by ensuring the workshop activities are flexible and interesting. 32
Phase 2
Phase two will include two focus group discussions (FGDs) and will involve the development of the data collection tools. Focus groups are useful to explore group or community views and needs. 33 In Bali, MSM and waria commonly work together; therefore, when conducting FGD in the same group, they may encourage new thoughts and enhance depth, nuanced and varied responses. 33 FGD1 will explore attitudes, behaviours and experiences of MSM and waria in Bali. FGD2 will inform the development and face and content validity of the survey. Participants will include approximately 10 MSM and waria (referred by partners), from the MSM community. The same participants will be invited to FGD1 and FGD2. The FGDs will be facilitated by the lead author using a semi-structured interview guide. A trained research assistant will take notes, including making reference to non-verbal communications, and manage the audio recording. 34
The interview guide for FGD1 will be informed by the literature and will be prepared with research partners during Phase 1. The questions could include current health and social problems faced by MSM and waria in Bali related to sexual attitudes, behaviours, access to health services, mental health issues as well as stigma and discrimination.
Participants of FGD 1 will be invited to participate in a second FGD one month after the first. During the one month period, it is anticipated participants will have the opportunity to reflect on the first FGD. This time period will also provide researchers and partners adequate time to analyse workshop findings and prepare a revised version of the survey. The purpose of FGD 2 will be to review the survey for face and content validity. In addition, academic and community experts (intervention-based expertise through the Ministry of Health Bali) (n = 4) who have been working and conducting research with MSM and waria nationally and internationally will review the survey for content validity.
To ensure a culturally relevant, acceptable and understandable instrument is developed, the TRAPD (Translation, Review, Adjudication, Pretesting and Documentation) team translation approach will be employed. 35 The survey will also be reviewed by partners, academic and community experts for face and content validity assessment. In order to prevent researcher bias, as the researcher team have worked and conducted research with marginalised groups including MSM and transgender people for many years, there will be a bracketing process at the beginning and throughout the study to set aside and document the researcher’s preexisting assumptions and beliefs related to the research. A reflexive process will be employed which will enable the researcher to consider these issues. 36 The researchers will constantly identify, discuss and record their assumptions and interests about topics that emerge during the data collection process. 37 This documentation will be used as part of the reflective process, and will be followed by critical reflection after each focus group with other researchers as well as conducting ongoing analysis of data. Reflection will be conducted throughout the study to enhance trustworthiness, permit emergent design and assess for saturation. Comprehensive descriptions of the contextual data and activities of the study; through engagement, reflexive journaling and documentation will also be conducted. 38 Moreover, the researcher will be collecting and coding the data, and a regular discussion with research team will be conducted. 39 Credibility will be enhanced by building a good rapport with the focus group participants and regular member checking of raw data. 40 In addition, as the first author/researcher is also an academic from a national university in Bali and has been involved in collaborative projects with some NGOs, existing networks and knowledge of services and programs will be beneficial throughout the research process. In order to reduce researcher bias, in addition to the bracketing process, member checking with research participants will be conducted to clarify whether the interpretation is representative of their thoughts/beliefs.
Data analysis
The FGDs will be recorded and transcribed verbatim. The transcription will be reviewed for errors. Notes will be made during and at the conclusion of the FGD to describe body language and group dynamics. A thematic analysis of transcripts and notes will be conducted. NVivo software will be used to assist data analysis and to manage the coding. Data analysis will include categorisation/merging codes/nodes and developing themes. 31 Coding is used to make sense and identify or thematic ‘tagging’ text with nodes/codes which emerge from the data.31,41 Coding detail approach will be used to cluster nodes/codes together in a ‘tree-structured’ system in order to obtain connected idea or concept in a set. 31 A codebook will be created as part of the analysis process to keep detailed descriptions about codes/nodes. 31 Themes developed from the findings of FGD1 will inform the survey questions. FGD2 will include specific discussion about the survey to ensure the content, language and format are consistent with the project objectives, are culturally appropriate and are easy to complete. FGDs will be conducted by the lead author who has expertise in qualitative data collection with these population groups and will ensure appropriate procedure for adults discussing sensitive issues.
Phase 3
Ten NGOs staff will be recruited during phase 1 and invited to the one-day workshop. These participants will become the research ‘partners’. Using a partner-driven sampling, an online survey (developed during Phase 2) will be administered to a minimum of 374 MSM and waria.42,43 Partners will identify respondents who are in a similar group as themselves (gay, waria, bisexual, HIV+ MSM and male sex workers/MSW). Partner-driven sampling is employed to ensure diversity of socio-demographic characteristics and geographic area representation. 44 Due to overlapping peer groups, sexual or social networks, partners may recruit the same people 44 ; however, partners will ask potential participants if they have previously completed the survey. In addition, place and date of birth and religion will be asked and matched data reviewed to reduce the chance of double responses from the same person. Each partner will be asked to recruit 30–40 respondents during a three-month period. Partners will provide respondents with a link to the survey. The survey will be anonymous, and informed consent will be given before participants start the survey. Partners will provide the link and recruit using different modes such as WhatsApp, email, SMS and gay dating mobile phone applications (gay-apps, such as Grindr, Hornet, Blued and BoyAhoy). If potential participants do not have internet access, they will be able to access an offline app available in a tablet which will be supplied by the partners and used for this project only. The online (and offline) survey will be conducted through QualtricsXM. To reduce the likelihood of multiple entries to the survey and to ensure respondents only complete the survey once, several screening questions will be included at the beginning of the survey. All respondents will be given a 30,000 rupiahs (AU$3) internet voucher. Contact details will be separated from the surveys as soon as data is downloaded.
The inclusion criteria are the following: 1. Males who in the last 6 months have ever had sex (by hand, mouth or/and anus) with a man, 2. aged 18 years and over, 3. have lived in Bali for at least 6 months and 4. have Indonesian citizenship.
The exclusion criteria are the following: 1. Those who plan to leave Bali to live in other parts of Indonesia or other countries in the next 6 months.
Sample size determination
Given the estimation of the MSM population in Bali, of around 14,000 adults, to obtain 95% confidence level and 5% precision (margin of error), the required sample for the survey is 374 respondents. 43
Every effort will be employed to enhance participation including: a well-respected institution managing the study; emphasis on the importance and relevance of the study; providing different completion options (online and offline including phone, tablet and computer formats); treating participants with respect and appreciation; ensuring confidentiality; ensuring the survey is as short as possible; and providing access to telephone and email for questions and comments about the survey. 45
The final survey will be developed based on consultation with MSM and waria in Phase 1 and with participants of FGDs in Phase 2 of this project. It will include demographic characteristics such as age, religion, place of residence, place of birth, educational level, occupation and marital/relationship status, and it is also anticipated to include the following: a. STIs risk attitudes and behaviours: type, determinants and enablers. b. Safe sex attitudes and behaviours: type, determinants, enablers and barriers.46-48 c. Strategies to increase safer sex behaviours amongst MSM and waria. d. Stigma and discrimination experiences.
46
e. Mental health status (distress and happiness level).
Data analysis
Descriptive statistics will be used to analyse the characteristics of respondents, and Chi-square tests will be employed to determine associations between categorical variables and t-tests for continuous variables (if applicable). Logistic regression and multiple linier regression will be employed to determine the predictors or relationship between socio-demographic and socio-ecological characteristics and stigma and discrimination; distress level and happiness; condom use and sexual attitudes and practices amongst MSM and waria. Specific variables will be informed by Phase 2. All statistical analyses including data entry will be performed in SPSS statistic version 25. 30
Phase 4
Community members (MSM and waria) will be recruited to participate in a semi-structured interview conducted by the lead author. The interview guide will be informed by the findings of the survey (phase 3). It is anticipated that the interviews may focus on discussion around the social-cultural context in which MSM and waria live in Bali including their experiences around stigma, discrimination and mental health (depression, anxiety and stress). Reasons for higher risk and safer sex behaviours, barriers that hinder safe sex behaviour, social norms around safe sex behaviour and strategies to enhance safe sex behaviours among MSM and waria may also be explored.
Research partners will purposively recruit participants. The inclusion criteria of participants will be informed by the survey (phase 3) findings. For example, if the survey found significantly different results between Balinese and non- Balinese MSM and waria, this fourth phase may be focused on gaining a deeper understanding of these differences and how this may impact interventions.
The researcher is aware that her background and experiences could influence how the data will be collected and analysed. Therefore, to enhance the validity of this data, member checking will be conducted after all the in-depth interviews have been completed, transcribed and interpreted by the researchers. A purposive sub-sample will be invited to clarify the researcher interpretation. 49 Moreover, other strategies will be used in order to maintain the reliability and validity of interviews, including note taking as well as audio-recording, avoiding leading questions and providing respondents an opportunity to clarify points made. 50
Several procedures will be used to improve the trustworthiness of this study. In order to reduce bias, the researcher will collect and code the data and discuss with the research team regularly. 39 Credibility will be enhanced by building a good rapport with the community. 40 To increase the conformability, several representative quotations from respondents that signify each theme will be included.38,40 Comprehensive descriptions of the contextual data and activities of the study through engagement, reflexive journaling, documentation and presenting the findings with quotations will provide transferability through allowing others to analyse the situation and research outcomes based on setting and context. 38
This study will be consistent with qualitative reporting, standard and criteria described in the literature including the COREQ and ENTREQ guidelines.51-53
Data analysis
The interviews will be recorded and transcribed verbatim. The transcription will be organised and reviewed for errors. A thematic analysis will be conducted. The NVivo software will also be used to help with coding, developing categories and themes and developing theory of the data (data driven). 31 This software is used to allow a better focus on ways of understanding the meaning of what is gained. 31 At the end of the analysis, themes and theory that have been shaped, in conjunction with the survey (phase 3) results, will inform the development of the explanatory model of this project.
Phase 5
Phase five includes the dissemination of the study findings. The findings will be made available and presented to relevant stakeholders including staff from the Ministry of Health, public health service, related NGOs and relevant professionals (Universities and academics) in a workshop. The workshop will also discuss the recommendations for future actions and strategies in relation to study results. Partners will be involved in facilitating this event. This workshop will introduce the final model and guidelines to inform safer sex among MSM and waria in Bali. This study is a supervised doctoral research project. Moreover, the study result will also be disseminated through conference presentation, peer-review journals and in a PhD thesis.
Discussion
The use of sequential mixed-methods with exploratory and explanatory phases in this CEnR project will facilitate deeper understanding of MSM and waria living in Bali, Indonesia’s attitudes, behaviours, and experiences. The mixed-methods approach in this research will add to the literature on the use of CEnR in marginalised populations; enables a deep analysis of the research results; in addition to acknowledging different views, paradigms, explanation and interpretation of phenomena. 54 The CEnR design as ‘participatory research and partnership’ with partners and community members supports this vulnerable community providing opportunity for input to the research process and implications. This process will enhance amenability of the proposed recommendations around policy and practice. 55 Moreover, this design allows and ensures more culturally congruent findings and guidelines for practice of the research translation.26,55
This project will also ensure ethical principles for community-based research are fulfilled. 47 These include trust and transparency between the researchers and research partners; equity, inclusion and balanced power amongst research partners, along with tolerance and conflict management during the project. 56 The sustainability of the partnership will ensure regular communication with research partners related to the project. 56
While the main strength of this research project is the use of mixed-methods design within CEnR which makes the findings and recommendations more comprehensive and culturally appropriate, the potential limitation may be under-sampling of isolated MSM and waria and those who do not have access to the Internet as the recruitment of the respondents for the third phase of this project will include partner-driven and online sampling.
In conclusion, this project aims to develop a specific model to help understand the attitudes, behaviours, and experiences of MSM and waria in Bali. The research will also inform the development of guidelines to inform policy and practice to enhance the health of MSM and waria in Bali. The use of sequential mixed-methods design within CEnR will inform subsequent research and may be useful in other settings and contexts.
Ethics
The research procedures have been approved by Human Ethics Committees from Curtin University, Western Australia (HRE 2019–0759) and Faculty of Medicine, Udayana University/Sanglah Hospital, Bali, Indonesia (No: 2521/UN14.2.2.VII.14/LP/2019). The anonymity and confidentiality of study participants are really ensured in this study.
All respondents will be provided information sheets describing the research and their rights to withdraw at any time, and will provide consent prior to their participation. Participant information and consent forms and instruments (interview guidelines and survey) will be in Indonesian language (Bahasa Indonesia). Data collected will be stored on a secure server accessible to research team members only.
Footnotes
Acknowledgements
The authors acknowledge the contributions of A/Prof. Sam Winter and Dr. Linda Portsmouth for reviewing the protocol and are grateful to Prof. Wirawan (in memoriam), all research partners (Arya, Gung Arie, Rio, Gino, Tut Nik, Kharisma, Bella, Melati, Kimora, Machoman, Yudi, Bella and Billy (i.m)) and NGOs that focusing on MSM and waria in Bali who have agreed to support this research.
Author Contributions
This paper is a protocol of a supervised doctoral research project. The findings of this project will be used by NWS to pursue a Doctor of Philosophy of Public Health at Curtin University, Australia. NWS was the one who is responsible for authors’ contribution of this work. All authors have delivered significant contribution on the development and conceptualisation of this paper. NWS was drafting this paper, while BM and SB were responsible in editing and giving guidance for this protocol. Revising the protocol was the responsible of all authors. The final version of this manuscript has approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project is funded through the Australia Awards Scholarship and administered through the doctoral program at the School of Public Health, Curtin University.