
Abstract
This research examined the process of engaging people with lived and living experience (PWLE) of mental health and substance use concerns in the co-design of a mental health service in Ontario, Canada known as an Alternate Destination Clinic (ADC). Specific objectives were to: (a) to explore the experiences of PWLE within a community-led health service co-design process; and (b) to identify lessons learned for engagement of PWLE that can be applied to future health service co-design processes. Using qualitative descriptive methodology, from March to April 2024, focus groups were conducted with organizational staff (n = 2 focus groups) and semi-structured interviews (n = 17 total) with service providers (n = 11) and PWLE (n = 6) involved in the ADC co-design process. Data collection focused on participant experiences and observations with respect to the participation of PWLE. Data were analyzed using content analysis, informed by the Bee et al. framework for service user-involved care planning. Participants emphasized organizational recruitment efforts, the co-design committee’s structure, and how roles were designed and communicated as factors that affected PWLE experiences. Lessons learned include a need for diverse recruitment practices, the provision of appropriate training to service providers (i.e., on trauma-informed care, language use), and the importance of empowering PWLE to develop and hold key decision-making roles within co-design processes. Findings point to the integration of individual, relational, and organizational factors in shaping the experience of PWLE in the service co-design process, and collaboration dynamics overall.
Introduction
Over recent years, there has been increased emphasis to meaningfully engage patients and communities within the development of healthcare services (Boivin et al., 2018; Bombard et al., 2018; Domecq et al., 2014; Holmes et al., 2019; Manafo et al., 2018; Vojtila et al., 2021). Patient engagement integrates service users and carers into service co-design processes, often referred to as user-led or user-involved care planning (Bee et al., 2015; Grundy et al., 2016). Service users are typically included in activities to increase participation and represent the perspectives of similar individuals, all with the intention of contributing to transformation of the health service. Indeed, in health service co-design, service users work collaboratively alongside service providers—as the end-users of a healthcare service being offered—to develop new services or iterate existing services to more effectively respond to healthcare needs (Veldmeijer et al., 2023). Successful co-design processes are typically characterized by shared decision-making power among participants; working relationships of trust, empathy, and reciprocity; and the privileging of perspectives among those impacted by a service (i.e., service users) in relation to those in service provision roles (Bellingham et al., 2023; Vargas et al., 2022).
People with lived and living experience (PWLE) are key service users who play a crucial role to community engagement in the mental health and substance use space (Sunkel & Sartor, 2022; Veldmeijer et al., 2023). Described as “experts by experience,” PWLE can be defined by a variety of roles depending on the identified criteria, including individuals with mental health and substance use challenges; caregivers of these individuals; or even, health professionals within this system (Vojtila et al., 2021). For the purposes of this research, PWLE will refer to individuals with mental health and substance use challenges and caregivers. Engaging PWLE in mental health and substance use service co-design has been shown to enhance relevance, accessibility, and effectiveness of the services developed (Sunkel & Sartor, 2022; Telford & Faulkner, 2004; Vojtila et al., 2021). Previous research indicates that involving these individuals fosters a deeper understanding of patient needs and preferences, leading to more patient-centered and impactful interventions (Telford & Faulkner, 2004). Moreover, engaging PWLE promotes representation, decreases stigma, and can empower individuals, providing a sense of ownership and agency in their care, which can improve care outcomes and satisfaction (Sunkel & Sartor, 2022; Vojtila et al., 2021). However, the inclusion of PWLE in service co-design is not without challenges. Barriers include potential tokenism, where participants’ contributions are undervalued or ignored, limited diversity of PWLE included in co-design processes, limitations in terms of the time commitment PWLE can offer, and power imbalances between professionals and service users that could potentially impact collaboration efforts (Mikolajczak-Degrauwe et al., 2023; Veldmeijer et al., 2023). Indeed, the experience of PWLE within service co-design, as well as the overall collaborative process, is invariably shaped by individual, relational, and organizational factors and the complex, cross-cutting dynamics therein (Bee et al., 2015). Overall, literature on the benefits and challenges of co-designing mental health and substance use services often emphasizes outcome-related aspects of the co-designed services (Austin et al., 2021; Schlichthorst et al., 2020); however, there is limited focus on the process-related outcomes of service co-design, such as the experiences and perceptions of PWLE during their engagement. A more fulsome understanding of these experiences, including the multilayered influence of individual, relational, and organizational factors, may contribute to the strengthening of community engagement within service co-design and—by extension—health service delivery.
This study was anchored by a practitioner-researcher partnership between Region of Waterloo Public Health and Paramedic Services (ROWPHP) and the University of Waterloo (Canada). ROWPHP facilitated a collaborative process to co-design an Alternative Destination Clinic (ADC) for Waterloo Region, Ontario, Canada. ROWPHP prioritized a co-design model for the ADC initiative, referred to as the ADC Steering Committee, that brought together key regional health and social community service providers, while also engaging the perspectives of individuals with lived and living experience of mental health and/or substance use concerns, and their family caregivers (PWLE). ADCs represent just one of the possible alternative mental health and substance use services; other services such as peer support programs, treat and refer initiatives, and crisis centers have been initiated worldwide (Creed et al., 2018; De Cotta et al., 2021; Shattell et al., 2014). In the ADC model, paramedic services would be permitted to transfer consenting patients who have called emergency services with mental health and/or substance use concerns to a community-based clinic, diverting away from hospital emergency departments where paramedics would otherwise be legally required to transfer patients (Meijer et al., 2024). Although numerous, varied approaches to emergency department diversion exist worldwide (McKenna et al., 2015; Pereira et al., 2021; Ribbers et al., 2020), within our Ontario study context, an ADC model is an innovative approach for paramedic services to support mental health and substance use crisis response. There is currently limited research evidence related to its effectiveness, beyond short-term pilot projects (Ford-Jones & Daly, 2022; Meijer et al., 2024; Weeks, 2023). Aside from the benefit of reducing overcrowding in emergency departments and reducing strain on acute care systems, diversion for mental health and substance use concerns to community-based clinics may also support improved mental health outcomes for patients seeking care who may be redirected to more appropriate services for their needs (Meijer et al., 2024). Individuals may also be more likely to seek early intervention through an emergency diversion model, which may promote patient autonomy and well-being and prevent the development of more severe mental health and substance use concerns (Meijer et al., 2024). Further, there may be opportunities through an ADC model to connect patients with community-based wraparound services that may also promote well-being and support the prevention of more serious health outcomes (Hubberstey et al., 2022; Tremblay et al., 2024).
Using the ADC Steering Committee as a case study, the purpose of this research was to examine the process of community-engaged co-design of a mental health and substance use service (2023–2024) with respect to the inclusion and participation of PWLE. The specific objectives were: (a) to explore the experiences of PWLE within a community-led health service co-design process; and (b) to identify lessons learned for engagement of PWLE, from the perspectives of both PWLE and service providers, that can be applied to future mental health service co-design processes. In doing so, the article aims to strengthen the application of co-design, implementation, and evaluation of community-engaged mental health services globally.
Method
Co-design of an ADC
In 2022, recruitment began to establish a Steering Committee of service providers and PWLE to co-design an ADC for Waterloo Region, Ontario. In an intentional effort to ensure broad and inclusive participation, ROWPHP took a multifaceted approach to recruitment which included hosting community information sessions and leveraging existing networks to reach individuals connected to mental health and substance use services. A total of 22 individuals were recruited to the ADC Steering Committee, which included 14 service providers who tended to be senior leaders within organizations or health facilities aimed at addressing mental health and substance use concerns in the community, and 8 community members with lived or living experience (PWLE) of accessing mental health and/or substance use services. To contribute to the inclusion of and accessibility for PWLE within co-design meetings, ROWPHP provided appropriate compensation to PWLE in the form of honorariums and implemented accessibility accommodations (e.g., closed captioning in videoconference meetings; opportunities for in-person meetings). Importantly, to guide ADC Steering Committee activities, a committee co-chair model was established, and a PWLE stepped into the leadership role of community co-chair. This individual guided the creation of meeting agendas, co-facilitated meetings, and contributed more broadly to committee operations, strategic planning, and direction-setting for the committee’s discussions and priorities.
From June 2023 to June 2024, the Steering Committee met to engage in ADC co-design. This consisted of collectively discussing a broad vision for what an ADC model would include (i.e., guiding principles), possible funding opportunities, and more technical/operational details regarding the ADC model. Meetings were conducted weekly for approximately the first 2 months, then transitioned to bi-weekly in Fall 2024, then monthly for the last few months.
Study Methodology
This case study used a qualitative descriptive methodology (Colorafi & Evans, 2016). As it is characterized by an in-depth inquiry of novel phenomena, this methodology was appropriate to closely examine the processes involved in co-designing a novel ADC mental health and substance use service model. This study was conducted by a team of three academic researchers from the University of Waterloo, Canada. Two researchers identify as female (LJB as a White Canadian cisgender woman; KR as a South Asian Tamil-Canadian cisgender woman). One researcher (WD) identifies as a White Canadian cisgender male. This study was also supported by the two co-chairs of the ADC Steering Committee, an ROWPHP manager (KM) and a community member with lived experience of caregiving (SK), who contributed to the study’s design and conceptualization and supported recruitment. Although closely partnered with ROWPHP to design and conceptualize the study, the researchers’ roles exist outside of the organization, and they were thus positioned to be able to provide an external evaluation of the ADC co-design process.
Participant Recruitment and Characteristics
Participants were recruited purposively for this study based on their involvement in the development and/or ongoing work of the ADC Steering Committee. Two members of the University of Waterloo research team attended a Steering Committee meeting in advance of data collection to verbally invite all Steering Committee members to participate in the study and followed up with an email invitation and information about how to participate.
Of 22 Steering Committee members actively involved at the time of this study, 5 declined participation or were not contactable: 3 service providers and 2 PWLE. Thus, study participants included a total of 17 Steering Committee members: 11 service provider representatives from approximately 13 different community partner organizations 1 and 6 community members with lived and living experience (PWLE). The six PWLE participants held intersecting personal and professional roles that influenced their participation and perspectives on the steering committee. Of the six PWLE, four individuals identified themselves as a caregiver for someone with mental health and substance use concerns. Two individuals held Indigenous and racialized identities, respectively. Furthermore, several PWLE were retired professionals who had now transitioned to participation in various community roles and networks including mental health advocacy committees, as well as family and parent support groups.
Study participants also included ROWPHP staff (n = 3) and management (n = 3) involved in the development, administration, and strategic support of the ADC Steering Committee. All participants provided written informed consent to participate. Ethics approval was provided by the Research Ethics Board at the University of Waterloo (Certificate #: 45579).
Data Collection
Focus Groups
In February 2024, we conducted two separate focus groups with ROWPHP staff (n = 3) and management (n = 3). Focus groups were conducted in-person and facilitated by two research team members (each approximately 1.5 hr in duration). Discussion focused on understanding the historical and organizational context leading up to the ADC co-design process, with an emphasis on recruitment approaches and strategies used to embed lived experience perspectives within the process from the outset.
Semi-Structured Interviews
From March to April 2024, we conducted one-to-one interviews (n = 17 total interviews; each approximately 1 hr in duration) with ADC Steering Committee members, both service providers (n = 11) and people with lived experience (n = 6). Interviews were conducted either in-person or online via Zoom videoconference software. All interviews focused on participant experiences, perceptions of, and observations on the co-design process, specifically with respect to the participation and inclusion of PWLE. Participants who were PWLE were invited to share in more detail about ways in which they felt supported and/or challenged in their participation on the committee. In addition to their experiences during the co-design process, all participants were asked to share lessons learned that might inform future community-engaged processes with PWLE across health services. Interview and focus group guides were developed in collaboration with ROWPHP staff and management, who provided feedback on the structure and content of the guides (see the Supplemental File for data collection guides). All focus groups and interviews were audio-recorded with participant consent and transcribed verbatim.
Data Analysis
Qualitative data were analyzed using content analysis (Kleinheksel et al., 2020). First, all transcripts were reviewed by two research team members (LJB and KR) for data familiarization and immersion. These team members were the same individuals who conducted all data collection procedures. Next, a round of initial coding was conducted by KR using QSR NVivo® qualitative analysis software for organization and retrieval of codes and coded excerpts. Bee et al. (2015)’s conceptual framework for service user-involved care planning was considered as an a priori framework within this initial coding. These authors identified a gap in the meaningful involvement and alignment of the priorities and experiences of service users and service providers in shared care planning. This framework describes process-focused hierarchical levels (individual, relational, and organizational) and can be used to conceptualize the experiences and challenges associated with successful user-involved care planning. The individual domain characterizes the personal identities and positionalities of PWLE as key drivers that influence degree of involvement within health service co-design, while the relational and organizational domains point to the influencing interactions that occur between service users and service providers and the structural features and organizational decisions that influence service user experience, respectively. Given how closely the ADC service co-design process aligned with these three hierarchical levels, the Bee et al. (2015) framework was chosen as an appropriate conceptual guide to provide analytic depth and nuance to our conceptualization of the experiences of PWLE in the ADC Steering Committee.
To enhance rigor and validity, the research team members (LJB and KR) reviewed the generated codes together to collapse, create new codes, and develop a parsimonious codebook to fit the data, which was then reapplied to all focus group and interview transcripts. Finalized codes were, therefore, reflective of the Bee et al. (2015) framework, with some data-driven adaptations. Triangulation of findings across data sources (focus groups and interviews), as well as collaboration among research team members, also contributed to the validity of the analyses (Creswell & Miller, 2010).
Results
Participants’ descriptions of their experiences of the ADC Steering Committee map to three chronological phases of engagement across the service co-design process: (1) set-up, recruitment, and initial impressions; (2) ongoing implementation and experience of the process; and (3) recommendations for future engagement.
Engagement Phase One: Set-Up, Recruitment, and Initial Impressions
Organizational Structure and Set-Up of the Co-design Process
Service providers, ROWPHP staff, and PWLE reflected on how they experienced the intentional efforts and actions taken by ROWPHP during the establishment of the steering committee and overall set-up of the co-design process. Both service providers and PWLE commented on the challenge of prioritizing and maintaining inclusivity within organizational efforts to recruit PWLE to a co-design process, while also managing practical constraints (i.e., the size of the co-design group). The need for a balance between open calls for community engagement and ensuring appropriate representation was reflected in many participants’ interviews (P1, P2, P3, P6, P15, P17). As one staff participant noted in a focus group, “we didn’t want to be a gatekeeper. . .Like, how do we decide who gets to sit on [the Steering Committee] and who doesn’t?”
One PWLE reflected on the significance of the honorarium offered by ROWPHP for their participation: “It made me feel appreciated, and it wasn’t because of the money, it was because someone was like, ‘we want you to be here’…It kind of made me breathe easier” (P1). Some PWLE noted that providing financial compensation for participation and considering accessibility accommodations can make members feel valued and supported at the individual level, thus promoting a more inclusive co-design environment (P1, P13, P17).
Reflecting the organizational domain, several participants, service providers and PWLE alike, expressed appreciation for the structured nature of the steering committee, provided by ROWPHP staff in the form of handling operations and strategic planning (P3, P5, P7, P9, P12, P14). As a result, the administrative and mental burden were offloaded from PWLE and service providers, which reportedly enabled more effective participation from members. However, the novel nature of the co-design process led to some lack of clarity regarding the purpose and role of steering committee members. One service provider used the analogy of “building the plane as we fly it” (P5) to describe the iterative changes that surfaced as the co-design process started to unfold. Several participants perceived of their roles as ambiguous within the committee’s evolving structure and emphasized the need for clarity and ongoing, effective communication moving forward among all steering committee members (P1, P2, P3, P7, P8, P10, P11, P16).
Early Impressions of the Co-design Process
In general, participants largely expressed being initially receptive to and encouraged by the co-design process. At the individual level, PWLE appreciated the potential for positive change stemming from their involvement, contrasting with previous experiences where consultations regarding service design and improvement did not lead to measurable action (P1, P2, P9, P17). As noted by one PWLE, “One of the things that this community has said for years and years. . . [is], ‘Thank you for your consultation. This is great. Can you put some action into that?’ And this [co-design process] has made action” (P2).
Some participants—service providers and PWLE—described their participation in the co-design process as the first of its kind (P1, P3, P10, P17). The inclusion of other PWLE made them “hopeful” (P10), especially among those who had never seen the degree of lived experience representation before (P1, P3, P10, P16, P17). As one PWLE participant shared, “This has not happened before. I have never in my whole life had health providers [put] effort collaboratively at a top level to create something workable” (P1). Furthermore, the novelty of the co-design process reportedly made both PWLE and service provider participants feel empowered as individuals in the process.
Effective Facilitation
Both service providers and PWLE described the facilitation of meetings as an integral contributor to a positive relational experience in the early phase of the co-design process. As one ROWPHP staff shared in a focus group, “that’s really where those small groups that we often do in the steering committee meetings came out because we realized that’s where we’re going to hear those voices and that’s how people are going to feel more comfortable.” PWLE and service providers highlighted the importance of creating an environment where PWLE felt their voices were heard, made possible through meaningful facilitation from those leading the process (P1, P2, P7, P8, P12).
The presence of a community co-chair was noted as a significant contributor to success in engaging PWLE (P1, P3, P5, P7, P8, P12). This was the first time that participants at large had experienced representation of PWLE in a leadership role within a community-engaged process, as shared by one service provider: I think having [the co-chair] with lived experience facilitating and leading has been great because it is about making sure there’s that champion there. . .So that [the co-design process] is truly for the community. (P3)
Furthermore, PWLE members particularly expressed appreciation for the PWLE in a leadership position, allowing them to advocate for, as well as amplify the voices and needs of PWLE (P1, P2, P9).
Engagement Phase Two: Ongoing Implementation and Experience of the Co-design Process
Imposter Syndrome and Perceived Underutilization Among PWLE
Despite initial positive impressions, PWLE identified several obstacles related to their personal confidence and skills while engaging in the co-design process. Some PWLE found it challenging to follow along with meetings due to the use of abbreviations and health systems-related jargon (P1, P13, P17): “I’m still struggling to understand when people just throw [abbreviations] out and I’ve written them down. . .Then I’m lost” (P13). Several PWLE felt that their input and skills were underutilized, with focus and priorities shifting more toward technical or operational details to which they were less equipped to contribute (P1, P10, P13, P17). Service providers seconded their concerns, perceiving a shift to meetings that were focused on communicating project updates rather than facilitating a more fulsome and collective decision-making and co-design process (P1, P3, P5, P8, P11, P13, P14, P16). PWLE questioned their individual competencies and whether this gap was due to not having adequate knowledge as community members, in relation to service providers (P1, P10, P13, P17): I wanted to participate more, but at the same time, I’m not sure in what way I could have. Even something as simple as writing the mission statement. . .I’ve written enough over my years in [my career]. . .Obviously the goal is to open a clinic. . .if these people [service providers] are doing it faster and they didn’t need my input or other parents’, then, that’s fine. (PWLE, P1)
Based on these concerns expressed, select PWLE participants vocalized personal feelings for whether the co-design initiative would lead to any substantive change for the mental health and substance use services available in the community (P1, P17). One PWLE participant shared: “That’s my fear, that at the end of the day, it’s gonna be exactly the same thing we have been seeing all the time, being replicated. And then you ask yourself, what was the point?” (P17). These concerns reflected PWLE’s hesitation with the co-design process, as well as a dissonance between some participants’ expectations regarding their individual involvement and the level of participation they felt was invited at later stages of steering committee activities as the co-design process evolved.
Personal Values and Priorities Among Co-design Participants
As the process unfolded, some participants (PWLE, especially) described the difficulty of balancing their steering committee role with other responsibilities such as full-time employment and caregiving duties (P1, P9, P10, P17).
I would have loved to be part of the project until it comes to [opening the clinic]. . .but unfortunately, I need to pay my bills. [The service providers] get paid for being in the meeting already. . .I signed up for full-time employment. I need to go fulfill my purpose, right? (PWLE, P17)
Furthermore, the condensed timeframe and conflicting schedules of service providers and PWLE uncovered the role of steering committee members’ personal priorities. A PWLE participant reflected on the value they place on building relationships with community members and the time required to make this engagement meaningful (P1). This personal value appeared to conflict with the perspectives of some service providers who expressed a desire for the co-design process to take less time and exhibit more actionable tasks (P1, P5, P9, P11, P12, P16). Participants acknowledged that time was limited and it was not always possible for mainstream processes to move at a pace they would individually hope for, highlighting how personal identities and values can affect participation in community-engaged processes.
Informal Conversations and Historical Context
During the co-design activities, rapid changes to available funding opportunities relevant to the ADC initiative, competing priorities among service providers, and shifts in leadership led to discussions and actions occurring outside of formal steering committee meetings, typically among selected service providers. These external conversations resulted in feelings of “missing something” among most PWLE participants (P1, P2, P10, P13, P17). As a service provider described: I was getting calls from other partners saying, “What do you think about this? Did you read that email? What are we going to do about that?” So, there are all these conversations happening that people with lived experience wouldn’t even be part of. (P8)
Moreover, historical relationships and collaboration among key service provider organizations created underlying confusion for individuals outside of the mental health and substance use systems space (i.e., many service providers had worked together on past initiatives which necessarily shaped their relationships and interactions within the co-design process). “There’ve definitely been a lot of things happening behind the scenes, and I think that’s a challenge in these processes where you have agencies that work together or have some form of relationship,” one PWLE shared (P10). Especially for those unaware of this historical context, these informal conversations and dynamics reportedly influenced relationships between PWLE and other stakeholders involved, as well as overall perceptions of the evolution of the co-design process.
Overall, PWLE and service providers engaged positively through collaborative facilitation and shared priorities; however, informal discussions that occurred as the co-design evolved, as well as historical relationships and ongoing collaboration amongst service providers occasionally left PWLE feeling excluded. These experiences highlighted the relational domain and impacted the overall experience within the community-engaged process.
Group Ethos: “The Coalition of the Willing.”
Overall, steering committee members held a shared priority and importance for engaging PWLE, which was emphasized throughout the initiative by both PWLE and service providers (P1, P2, P3, P4, P5, P7, P10, P11, P13, P17). The support from service providers for the inclusion and meaningful participation of PWLE contributed to the progress made in the co-design process. The process of multiple stakeholders coming together and having shared values for engaging PWLE in their individual and organizational priorities was described as a “coalition of the willing” (P5).
Support for the community-engaged process reportedly extended beyond committee members to the broader community, providing further motivation and relationships among members for the co-design process. As one PWLE explained, “there’s a lot of interest in moving forward in the region to figure out how to engage community well in a way that centres people’s voices who have experience of services” (P17). Additionally, through media exposure and “unanimous support” from a regional government body, the steering committee received positive support for their community-engaged process.
Across the first two phases of the engagement process, intentional recruitment and accessibility-related efforts, well-structured committee operations, and effective facilitation enhanced engagement of PWLE by ensuring broad representation as well as a supportive and inclusive environment (organizational and relational implications). Moving forward, the evolving nature of the co-design process occasionally created confusion and what was perceived as fragmented communication that challenged effective participation. Although PWLE and service providers had a shared interest in creating a new model for mental health and substance use services, their relational interactions served to both enhance and detract from how PWLE experienced the community-engaged process. Individually, PWLE viewed the co-design process as novel and empowering for meaningful change; challenges were also experienced in the form of inexpertness in mental health systems and dissonance with their personal values. Findings mapped to individual, relational, and organizational domains, as inextricably connected in terms of their influence on the experiences and perceptions of PWLE within the co-design process.
Engagement Phase Three: Looking to the Future
Recruitment and Capacity Building Activities Moving Forward
Some participants highlighted the necessity of training (e.g., trauma-informed care for working with PWLE) and thoroughly orienting all committee members to the process, in order to facilitate a community-engaged approach and effective engagement of PWLE (P1, P8, P13).
[We] needed to go back to the group and say. . .“Here’s a bit of an orientation on what shared decision making looks like. Here is our trauma-informed care practice. The people who are recruiting with lived and living experience, their expertise is. . .“I lived this. Listen to me”. . .which is something that you don’t [always] have, and you desperately need. . .for any initiative to be successful. (Focus Group Participant)
Building relational connections within the broader community for effective recruitment was another key recommendation shared among participants. The need for patient, intentional, and persistent engagement efforts to foster meaningful relationships within the community was noted as integral for inclusive and comprehensive recruitment (P2, P6, P17). Participants also noted the importance of increasing diversity and intersectional perspectives (P1, P3, P4, P5, P6, P7, P8, P14). As a service provider shared: I’d be more curious about engaging with individuals. . .to understand how marginalized populations—like equity-deserving populations, BIPOC [Black, Indigenous, People of Colour] populations—reasons why they’re not going to the [emergency department] or why they won’t want to engage with police and how we can work to repair those relationships or fix them through [this co-design process]. (P8)
Participants, both PWLE and service providers, highlighted the need for more equitable representation of marginalized groups such as individuals experiencing homelessness, the 2SLGBTQIA+ community, refugees and newcomers, as well as racialized individuals.
Structure and Organization of Future Co-design Processes
Participants shared valuable structural insights for future community-engaged processes, emphasizing the importance of transparency in communication to keep all members informed (P4, P5, P9, P10, P11, P15). As one PWLE noted, “I think there’s a part of communication that needs to improve. Even if it just is saying ‘this group met independently and they’ve worked on this’, at least you’ve been made aware of that” (P10). Another crucial insight from participants was the need for PWLE in leadership within community-engaged initiatives to ensure the voices of other PWLE are heard and valued in decision-making processes (P2, P4, P8, P9). Finally, aligning with the organizational domain considerations of the user-involved care planning framework, providing a defined structure and specified roles for PWLE was noted as an important consideration for future initiatives: Ask people to provide input, to give feedback, but be very clear on scope and parameters. That is what would be meaningful engagement and actually productive so that people are coming to the table with realistic expectations, with some important feedback to share, but in a way that’s grounded and reasonable. (Service Provider, P11)
As reflected in participants’ insights, these actions related to communication and setting shared expectations would help ensure that all committee members have shared understandings of their role in order to contribute effectively. Several lessons for future community co-design processes were consistent across PWLE and service provider participants’ perspectives (Box 1).
Lessons Learned for Future Community Engagement Initiatives
These three domains (individual, relational, and organizational), together with the positive and negative influences and interconnections within, ultimately shaped the overall experience for PWLE and their engagement across the phases of the health service co-design process (Figure 1).
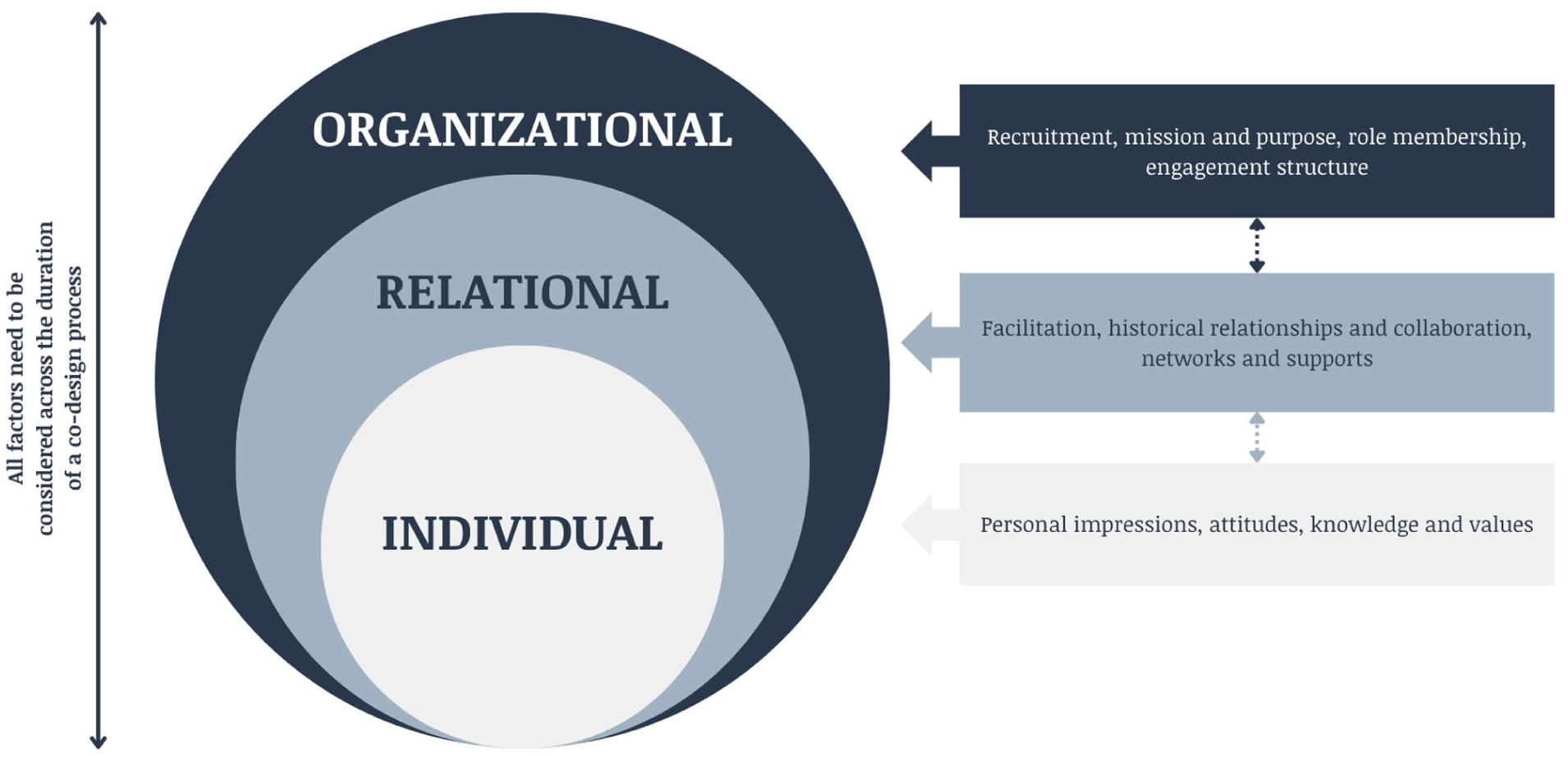
Factors Influencing PWLE Engagement Across the Duration of a Service Co-design Process
Discussion
These findings highlight the complex dynamics among individual, relational, and organizational factors that shape the experiences of PWLE in engaging in mental health service co-design. Particularly within the individual domain of the Bee et al. (2015) framework, this study’s findings align with existing literature that highlights the positive impact of engagement on self-perception and hopefulness among PWLE (Austin et al., 2021; Dreier et al., 2021; Schlichthorst et al., 2020). As service users and carers, PWLE in this study held strong intrinsic motivation for participation and sustained engagement in the co-design process, which is known to significantly contribute to the outcomes of community engagement (Mikolajczak-Degrauwe et al., 2023). Although the process was experienced positively overall, some PWLE reflected on discord between their expected role (e.g., as a partner or decision-maker) and actual engagement role (e.g., as co-thinker or advisor) and feelings of inadequacy or a sense of underutilization that resulted (Veldmeijer et al., 2023). These findings underscore a need for setting and reiterating clear expectations regarding involvement and roles across the duration of a co-design process, regardless of participants’ identities (e.g., as service providers, operational staff, or PWLE). Within the relational domain, power imbalances between service providers and PWLE can often complicate communication and relationship-building—crucial for fostering an inclusive environment—and potentially marginalize the voices of PWLE (Hawke et al., 2024). This study underscores the need to continually assess and address these challenges to fully realize the benefits of empowering lived experience voices in co-design initiatives (Maguet et al., 2023). Finally, within the organizational domain, this study highlighted the need for intentional organizational recruitment practices and training of co-design participants (i.e., steering committee members) to ensure effective community engagement (Austin et al., 2021; Maguet et al., 2023; Vojtila et al., 2021). For example, recruitment and training processes should aim to enhance participants’ capacities to support PWLE and clearly outline a shared commitment to equitable inclusion and support of PWLE.
Indeed, results emphasize the ongoing interplay of individual, relational, and organizational factors across phases of the steering committee process, shaping participant experiences, and process-related outcomes. These findings point to the importance of continually and critically reflecting on inclusion across all phases of engagement, with careful consideration of contextual factors that can undermine engagement efforts. For example, despite well-intentioned organizational structures and processes, historical context and preexisting individual relationships among service providers, organizations, and individuals can play a significant role in shaping collaboration dynamics. Similarly, participants held a shared value and commitment to the inclusion of PWLE in the co-design process; however, at times, this “individual factor” influenced relational dynamics as service providers appeared to hold some underlying assumptions about PWLE members’ time, capabilities, and experiences. Evidently, it is necessary to contend with, and thoughtfully account for, each domain in the development of inclusive co-design processes. Moreover, this study’s conceptualizing of the integration and embeddedness of individual, relational, and organizational factors in shaping PWLE engagement and experience presents a theoretical contribution as well, where the Bee et al. (2015) framework and other similar models (Carman et al., 2013) have typically conceptualized these dynamics within hierarchical and discrete levels, rather than as cross-cutting and integrative.
Additionally, this study reiterated that diversity remains an area for improvement in PWLE engagement within mental health services co-design (Hawke et al., 2024; Vanstone et al., 2023). Participating service providers tended to reflect more on demographic diversity among the co-design committee (e.g., limited representation from racialized minorities, individuals experiencing homelessness, and newcomers), while PWLE highlighted the need for diversity of ideas in the process (e.g., caregiver, individual, and practitioner perspectives; representation across community groups; varying experiences with mental health and substance use challenges). This distinction reflects a need for a more holistic approach to diversity and recruitment in mental health services co-design, one that encompasses both equitable representation and the inclusion of diverse perspectives among participants.
Finally, this study’s findings indicate the tension between maintaining efficiency and ensuring equity when engaging community in co-design processes. This discourse is common in the global literature on health systems and services resource allocation (Asamani et al., 2021); however, it also has relevance to the process of engaging PWLE in mental health service co-design. Ensuring that engagement processes are both efficient and equitable is crucial for meaningful participation, yet this balance can be challenging to achieve. The findings in this study suggest that while organizations strive for efficiency, equity must remain a priority to ensure that all individual voices, particularly those of PWLE, are heard and valued throughout the process, and respectful relationships upheld. While emergent from a mental health service co-design process, lessons learned from across this study are readily transferable to other service co-design approaches that work alongside PWLE, including within health promotion and prevention initiatives. For example, these lessons could be applied to programs and initiatives that aim to address intersecting social determinants of health such as housing and employment. Although there is recognition of the need to include PWLE in co-designing housing and employment programs and policies with people experiencing low-income (Malik et al., 2024), the urgency of addressing these issues may surface similar tensions identified in this study. Moving forward, meaningful engagement of PWLE includes a strong and ongoing commitment to equity at all stages of dynamic co-design processes.
Strengths and Limitations
This study was anchored by an academic-community partnership between University of Waterloo researchers and ROWPHP, which facilitated an in-depth examination of the experiences and perceptions of service users and providers involved in a co-design process. This builds from and extends an existing literature that has, to date, largely focused on outcomes from community engagement at the co-production and implementation levels (Austin et al., 2021; Schlichthorst et al., 2020; Vargas et al., 2022). This case study was not co-designed and data were not gathered or analyzed in collaboration with PWLE, which may have provided additional depth or nuance to participant insights and interpretation of data. Additionally, there existed a lack of diverse representation among PWLE involved in the co-design process, as the majority of PWLE on the steering committee were caregivers to individuals with mental health and substance use challenges. While important, the perspectives they shared in this study may differ from those of individuals directly affected by mental health and substance use challenges. Future co-design processes—and by extension, research evaluating participant engagement—should aim to broaden and diversify participation to include individuals directly impacted by these challenges, as well as individuals with marginalized and intersectional identities. Finally, this study was limited to interview and focus group data that was collected at a single point of time during a highly-dynamic co-design process, which may not reflect the perceptions of participants over the duration of the process. Future research may benefit from a study design that aims to gather data longitudinally, across the duration of a co-design process.
Conclusion
This qualitative study explored the experiences of people with lived experience within the ADC Steering Committee, a community-based mental health and substance use service co-design process within Waterloo Region, Ontario, Canada. The implementation of this type of intervention for emergency department diversion could promote early intervention for mental health and substance use concerns and prevent the development of more severe health outcomes. Findings emphasized facilitators and barriers for the inclusion of PWLE within and across individual, relational, and organizational domains, as well as how the complex interplay among these influences can shape participant experiences and engagement across the process. Opportunities exist for strengthening community engagement within mental health services co-design, including a need for service providers and organizations to prioritize training; transparent communication between stakeholder groups; commitment to diverse, equitable recruitment and to a collective effort to include and support PWLE; and clearly defined roles for PWLE, including leadership involvement. Lessons learned from this study’s co-design process are broadly applicable to other efforts to engage individuals with lived experience in the design and implementation of health promotion or prevention initiatives.
Supplemental Material
sj-docx-1-prv-10.1177_26320770251359606 – Supplemental material for Engaging People With Lived Experience in Mental Health Service Co-design in Ontario, Canada
Supplemental material, sj-docx-1-prv-10.1177_26320770251359606 for Engaging People With Lived Experience in Mental Health Service Co-design in Ontario, Canada by Laura Jane Brubacher, Kobisha Rajeswaran, Katie McDonald, Steve Keczem and Warren Dodd in Journal of Prevention and Health Promotion
Footnotes
Acknowledgements
We wish to express gratitude to the Alternate Destination Clinic steering committee members and Region of Waterloo Public Health and Paramedic Services staff who participated in this research and shared their insights and experiences with our research team. We also thank Sabeen Abbas who supported the facilitation of a focus group.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada [892-2023-1004 to LJB].
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author KM receives remuneration from Region of Waterloo Public Health and Paramedic Services (ROWPHP). Authors LJB, KR, SK, and WD have no conflicting interests to declare.
Data Availability Statement
The data are available in the article and in its online supplementary material.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.