
Abstract
The development of culturally safe intimate partner violence (IPV) services for immigrant and refugee women is strongly tied to understanding how IPV and its concomitants can be different for immigrant and refugee women. A lack of knowledge will contribute to inefficient, inappropriate, and less effective services. This study draws upon the expertise and wisdom of immigrant/refugee IPV survivors who serve on a survivor-only advisory board for IPV programming. The dialog of 35 attendees who participated in immigrant/refugee IPV survivor advisory board meetings was analyzed using reflexive thematic analysis to generate themes that captured their lived experiences of IPV, IPV support (i.e., their journey and recovery process), and their wish list for what they hoped would have been different. Three major themes and nine subthemes were generated (Theme 1: Experience of Intimate Partner Violence Is All-Encompassing; Theme 2: Immigrant and Refugee Survivors Experience Gaps and Therefore Feel Lost When Seeking or Receiving Support; Theme 3: Empowerment Is a Core Need). This study’s results study contribute to a more nuanced understanding of IPV for immigrant and refugee women (including how they tend to experience and navigate IPV differently than locally born ethnic/racial minoritized individuals) and provide valuable information that could help service providers and policy-makers develop and implement more culturally safe and effective intervention and prevention strategies.
Keywords
Within the last 5 years, an estimated 2% of Canadian women have experienced physical or sexual intimate partner violence (IPV), and about 7% have experienced emotional abuse (Lysova et al., 2019). Although rates of IPV are reportedly lower in Canadian immigrant women compared to their locally born counterparts (Du Mont & Forte, 2012), rates increase for immigrants the longer they reside in Canada (Brownridge & Halli, 2002). Additionally, immigrant women who are survivors of IPV report significantly lower levels of trust among people in their community and more instances of discrimination, which may act as barriers to help-seeking (Du Mont & Forte, 2012). The harmful physical and psychological consequences of IPV appear similar for immigrant and non-immigrant women in Canada (Du Mont & Forte, 2012); however, there is a larger familial impact of IPV against immigrant and refugee women because they are more likely to have children in the home (Du Mont & Forte, 2012).
The research that does exist substantiates the need to investigate IPV separately for immigrant and refugee survivors rather than generalize from locally born populations, including from those who hail from racialized or non-Western ethnic backgrounds (Okeke-Ihejirika et al., 2020). Immigrants and refugees possess many IPV-relevant experiences related to the settlement process that locally born women do not possess, such as those related to acculturation, learning a new language, learning new laws and social customs, not having educational or work credentials recognized, the threat of deportation, and potentially having undocumented immigration status (American Psychiatric Association, 2019; Okeke-Ihejirika et al., 2020). In addition, it appears that the typical profile of protective and risk factors for IPV differs in some important ways between immigrants/refugees and locally born women (Sabri et al., 2018). For example, U.S. and Canadian laws against IPV, provision of information about rights and legal recourses if IPV happens, and community integration and support are more protective for immigrant and refugee women than locally born women, whereas factors like threats of public humiliation, familial preference for a male child, and having a partner from a different race/culture place immigrant and refugee women at greater risk (Sabri et al., 2018).
Nevertheless, due to various cultural and settlement-related barriers, as well as prejudice, cultural biases, and discriminatory policies and laws, immigrant and refugee women often do not seek institutional support services for IPV (Okeke-Ihejirika et al., 2020). Moreover, when they do seek professional support, it is common for them to experience discrimination or non-culturally adapted treatment from healthcare workers and service providers (Du Mont & Forte, 2012). This is sometimes because professionals unjustifiably blame the IPV on the cultural values and practices that foreigners from non-Western countries bring to Canada or because professionals psychopathologize their emotion-focused coping strategies because problem-focused coping resources are the Western norm (Okeke-Ihejirika et al., 2020). It is also sometimes because many IPV programs in Canada, implicitly or explicitly, consider divorce/separation as the preferred or most empowering solution and are not focused on reconciliation, yet many immigrant and refugee women are consumed with rebuilding their lives with the abusive partner (Okeke-Ihejirika et al., 2020). Hence, the occurrence of IPV, how it manifests, its impact, involvement with support services, lived experiences, and pathways forward seem to be, in some ways, distinctive for women from immigrant and refugee communities compared to locally born populations, including racialized and ethnic minority ones (Okeke-Ihejirika et al., 2020). Therefore, it should come as no surprise that professional services cannot just adopt mainstream IPV procedures. These are often not culturally safe (Curtis et al., 2019), are typically less effective with immigrant and refugee women, or are often not effective at all (Okeke-Ihejirika et al., 2020; Simon-Kumar et al., 2017). In fact, Okeke-Ihejirika et al. (2020), on the basis of their scoping review, concluded that “the majority of existing services and policies. . .are not well suited to immigrant women’s needs and may undermine [their] capacity to find satisfying solutions” (p. 788). They further go on to say “immigrant’s women’s. . . reluctance to access formal help has primarily to do with the failure of services and policies to provide adequate assistance that corresponds with their specific situations” (p. 802).
Although there is slowly growing research on IPV with immigrants and refugees (Okeke-Ihejirika et al., 2020), one generally uninvestigated source of knowledge is survivors, especially immigrant and refugee survivors, who serve on survivor-only advisory boards for IPV programming. Survivors on advisory boards can provide a perspective not common in the literature that may offer novel insights or at least strengthen the existing knowledge base through validation and expansion with a different type of survivor. It is acknowledged that the contributions of survivors on advisory boards may, in some way, resemble the perspectives provided in research on survivors in peer-led support groups. However, those in peer-support groups are focused on receiving support and perhaps on supporting peers in day-to-day circumstances. In contrast, those on advisory boards are, through self-selection, generally survivors who have experienced some notable degree of success or are able to look beyond their own situation and have (and are highly motivated to share) ideas on what would be helpful for others in similar circumstances. In addition, the advisory board context alleviates the expected emotional investment of giving and receiving support in peer-support groups. Therefore, survivors on advisory boards are permitted more opportunity to engage in deeper retrospective self-analysis, to look beyond just their own experiences, and to contribute ideas about what was or would have been helpful for them and for other women in similar circumstances. In summary, conducting research with IPV survivors who serve on advisory boards holds potential to offer novel insights and generalize previous findings.
Purpose of the Study
This study conforms to the following two underlying premises:
“Service providers [and researchers] need to acknowledge immigrant [and refugee women] survivors as active knowers of their situations and trust their decision-making processes” (Okeke-Ihejirika et al., 2020, p. 802).
“To effectively help immigrant [and refugee] women who have histories of abuse, policies and services need to value immigrant women’s diverse and creative responses to IPV” (Okeke-Ihejirika et al., 2020, p. 802).
In line with these premises, the purpose of this study was to draw on the wisdom and experiences of advisory board members for immigrant/refugee IPV programming to generate themes that capture their lived experiences of IPV and support (i.e., their journey and recovery process) and their wish list for what they hoped would have been different. By tapping into their wisdom and lived experience and constructing themes to capture patterns of meanings in their accounts, we hope to (a) contribute to a slowly developing and more nuanced understanding of IPV for immigrant and refugee women, (b) continue to elucidate differences in how locally born and immigrant or refugee women navigate IPV, and (c) provide valuable information that could help service providers and policy-makers develop and implement more culturally safe and effective intervention and prevention strategies.
Method
Participants and Setting
Eligible participants (a) had at least basic conversational English proficiency, (b) had previously received counseling for IPV, and (c) were immigrants or refugees who identified as women. The advisory boards were facilitated and run by moderators (registered counselors) from a large nonprofit community organization. The community organization, located in the metropolitan Vancouver, Canada, area, provides settlement and counseling services to new immigrants and refugees. This organization received a federal government grant to develop a new counseling program for immigrant and refugee survivors of IPV and had been mandated to allocate some of the funding toward formal program development activities. The second author volunteered to assist them with the grant funding application, and they subsequently reached out to him to assist with analysis of the advisory board data.
There were 35 total attendees to the six advisory board meetings that provided the data for the present study. The attendees were all previous clients of the community organization. They ranged in age from 29 to 57 (M = 41.3, SD = 8.2). Each meeting was attended by an average of 5.8 women (SD = 2.0), with a minimum number of three attendees and a maximum of nine per meeting. The advisory board meetings had open enrollment. It is estimated that 16 different participants attended the meetings and that some women attended up to three advisory board meetings. Due to the sensitive nature of the discussions and privacy worries amongst some of the participants, the research team was not given permission to identify the recurring participants and to collect additional participant characteristics. The basic demographic information collected is provided in Table 1 and was obtained as part of a feedback questionnaire administered at the end of each meeting, based on 28 attendees who provided this information (80.0% response rate).
Demographic Characteristics of Attendees Across Meetings
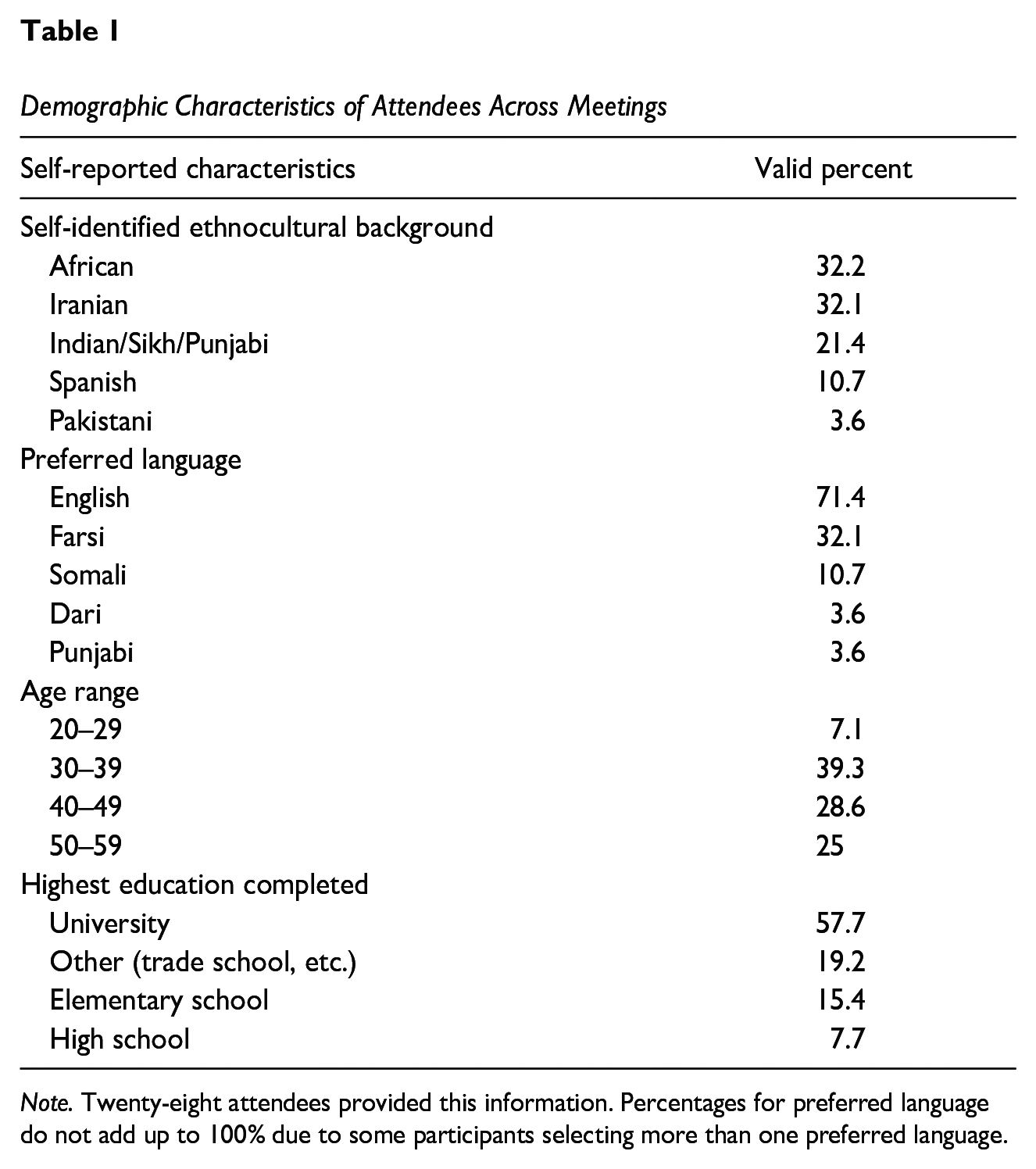
Note. Twenty-eight attendees provided this information. Percentages for preferred language do not add up to 100% due to some participants selecting more than one preferred language.
Researcher Descriptions
The first author is a cisgender South Asian Indian man who was born in Canada but who also lived in the United States as a permanent resident before returning to Canada. He is currently an associate professor of counseling psychology. He was drawn to this project because the primary population served by the nonprofit organization running the services was Indo-Canadian individuals primarily of Punjabi descent—one of his main areas of counseling and research interest—and because his first job as a counselor was as a domestic violence counselor and he was eager to rebuild his knowledge and competence in this area. Because this researcher was extremely familiar with IPV specifically within the Punjabi community, and not highly familiar with its unique manifestation within other non-Western cultures, he had to be mindful during the research process not to over-accentuate understandings congruent with the manifestation of IPV within the Punjabi community. This researcher expected that the survivors would emphasize culture, cultural inconsistency, and culturally adapted counseling as central to their lived experiences of IPV and IPV recovery. He also expected them to highlight the intersection of IPV with other experiences characteristic of the migration process in a manner that would be less common amongst Canadian-born survivors
The second author is a cisgender woman who was born in Japan and who has lived in the United States, Germany, and Canada. Her own lived experiences with immigration and mental health drew her to the current research topic. She is employed in the field of crisis intervention and has previously conducted research on the intersection of culture and counseling using reflexive thematic analysis (RTA). Given her past reading on the topic, she expected that cultural stigma surrounding IPV and cultural incompatibility between Canadian services and the survivors’ needs would be salient topics. Because she was not involved in the advisory boards and thus did not interact with the participants, she had no prior knowledge of the nonprofit or experience with it. Therefore, she was able to review the data in a potentially more creative manner not constrained by past personal impressions of the participants.
The third author is a cisgender Iranian-Canadian woman and doctoral candidate in a PhD program in school and applied child psychology. As an immigrant herself, she has a passion for understanding immigrants’ experiences across different settings, and this is what drew her to this project. Her main research focus centers around immigrant families’ experiences with receiving psychological services. This author attended advisory board meetings as an observer and was the only member of the research team to do so. She expected participants to focus mostly on the familial aspects of IPV rather than on legal and other systems-wide experiences. Because this author attended the advisory board meetings, she was least involved in data analysis, only providing feedback and thoughts after initial themes and codes were generated (and not during initial coding). This was to limit the influence of any idiosyncratic personal or interpersonal reactions to specific participants that could unnecessarily affect interpretation of textual data—the unit of analysis in this study.
Data Collection Procedures
This study received behavioral research ethics board approval from the three authors’ institution. Immigrant or refugee women who were survivors of IPV and had previously or were currently receiving counseling services at the specific nonprofit organization devoted to serving immigrants and refugees were invited to participate in a survivor advisory board to inform service provision at the organization. Invitations were provided by staff members of that organization or via word of mouth from other clients of the organization. Prospective attendees were told that we wished to draw upon their lived experiences and wisdom related to their IPV journey and recovery process. Specifically, they were informed that they would be asked to share their general experiences of IPV and of support services, provide feedback on the IPV program offered by the organization, identify the gaps in support for immigrant and refugee survivors of IPV, and report what was or would have been (more) helpful.
Six survivor advisory board meetings were held at the particular community nonprofit organization and facilitated by its counselors. Participants were compensated with $80 per meeting attended. The same counselor moderated each meeting, and she started each session with an introduction, the agenda, and a review of an aspect of the IPV programming provided by the organization as a way to begin the discussion. Subsequent discussion was moderated but mostly unstructured, although the moderator utilized prepared discussion prompts as necessary to continue the discussion. The moderator also utilized group counseling-type skills (e.g., empathic reflections, clarification questions, inviting individuals) to (a) promote group safety and deeper levels of self-disclosure and (b) ensure all participants were given the opportunity to speak versus allowing a few group members to dominate the discussion.
Meetings were held over a 19-month period. They occurred at various time intervals due to staff availability but averaged about once every 3 months. Each meeting lasted 90 min. The first two meetings were held in-person, and the last four meetings were held virtually through Microsoft Teams. Four out of the six meetings were audio-recorded for verbatim transcription purposes, and two meetings had live transcription because at least one attendee during those two meetings did not feel comfortable being recorded. Following each advisory board meeting, within a week, participants were emailed the same online questionnaire, administered using Qualtrics, which included questions about demographics and general questions about ways to adapt IPV services specifically to their culture and community services improvements that could be implemented to better support survivors of IPV. The questionnaire’s completion rate was 80%, indicating a sizeable continued investment of the individuals in their advisory role beyond just meeting attendance.
Analysis
RTA following Braun and Clarke’s six-phase process (Braun & Clarke, 2006, 2019; Terry et al., 2017) was used to analyze the transcriptions and feedback forms obtained during advisory board meetings. The main analyses were conducted by the second author, with support and auditing roles assigned to the first and third author. Analysis was conducted through a critical realist epistemological lens, which asserts that a true reality exists but is never directly accessible because it is always mediated by cultural meanings and the individuals’ subjective understandings (Terry et al., 2017). Therefore, we recognize that the themes generated in the present study represent the researchers’ interpretations, and other coherent elucidations might have been generated by different researchers (Braun & Clarke, 2019).
Phase One: Familiarization With the Data
Each questionnaire response and transcribed advisory board meeting was read at least three times over several weeks before coding began with the objective of solidly grasping the information, beginning to observe patterns, and generating preliminary analytic ideas. Personal reflexive notes were taken during this prolonged engagement with the data to refer back to during later phases of analysis to increase credibility and confirmability (Braun & Clarke, 2019; Lincoln & Guba, 1985; Nowell et al., 2017).
Phase Two: Generating Initial Codes
For coding purposes, no distinction was made between data provided by questionnaire responses and transcribed meetings. Codes were generated and documented in Microsoft Excel along with the raw data that they were associated with, and any changes to codes were also documented to provide transparency regarding the analytic process. Changes to initially documented codes sometimes occurred based on new understandings developed from review of additional data or insights developed from further familiarization with the data. Two strategies were utilized to ensure that the codes were reflective of the entire sample of individuals. First, during review of transcripts, the audio of the advisory board meeting was reviewed to give some idea of when comments came from different speakers. Second, questionnaires were numbered, and therefore it would be evident during coding and theme generation if a grossly disproportionate number of codes or themes reflected a small subset of individuals. Peer debriefing and consultation with the other two members of the research team were utilized once initial codes were developed to promote more thoughtful engagement with the data and to explore alternative codes (Braun & Clarke, 2019). The other members of the research team were there to generate alternative ideas, address possible contradictions, offer additional insights, and allow the primary coder to reflect on different ways of understanding the data, but the primary coder retained final authority on coding. In line with RTA’s underlying epistemology (Braun & Clarke, 2019), this was done to ensure that the findings represented the primary coder’s conceptualization of the data and “embrace researcher subjectivity as a resource for research” (Braun & Clarke, 2023, p. 2) rather than seek a consensual understanding that implies a degree of accuracy or underlying objective truth to the final results. During these debriefing meetings, revisions were made, and notes for the audit trail were taken.
Phase Three: Generating Themes
The consensual set of codes was then examined for patterns of shared meaning to generate themes and subthemes. The goal was to consider themes’ utility in representing an overarching narrative for answering the research questions rather than have the themes serve as predictable topic domain summaries (Braun & Clarke, 2019; Byrne, 2021). When beneficial, subthemes were generated to provide further nuance and clarity to the results. The survivors’ own words were used as much as possible in titling themes and subthemes.
Phase Four: Reviewing Themes
The provisional themes/subthemes were reviewed in relation to the original codes to check whether they still represented the data. When a code seemed inconsistent with the theme it was grouped under, the code was moved to a more appropriate theme, or the theme name was modified to better capture its assigned codes. After a satisfactory thematic map was created, the second author checked whether each of the themes was meaningfully distinct and whether they came together to form a coherent and informative narrative that represented that data or if further analysis was necessary (Terry et al., 2017). As a part of a negative case analysis (Lincoln & Guba, 1985), checks on whether there were any themes or data points that were overwhelmingly contradicted were carried out. When there were only a couple contradictory data items in relation to a theme, it was subject to peer debrief again and then finalized. Peer debrief was discussion-focused and centered on clarification questions and possible alternative interpretations of the codes’ meaning, and emphasized developing a richer and more nuanced understanding of the data rather than full consensus on meaning (see Braun & Clarke, 2019). Discussions centered around each members’ thoughts, and the primary coder incorporated the content of the discussion as they saw fit to better their own understanding and conceptualization of the data.
Phase Five: Defining and Naming Themes
Short summaries of the meaning behind each theme and subtheme were created and then named based on their underlying meaning (Terry et al., 2017). Titles and definitions were reviewed by other research team members, and peer debriefing was utilized to discuss and have the coder revise the titles and definitions as needed. Finally, an inquiry audit was carried out by the third author according to the procedure outlined by Lincoln and Guba (1985) to review the analytical procedures and decisions for fidelity to the research design and the confirmability of the findings.
Phase Six: Producing the Report
The order in which the themes were presented followed a logical ordering of the narrative of the story that was derived from the data. Thick (elaborate) extracts of client statements were utilized to provide contextual information (Lincoln & Guba, 1985).
Methodological Integrity and Trustworthiness
To build the trustworthiness of the study and findings, steps were taken to establish credibility, transferability, and confirmability (Lincoln & Guba, 1985). To ensure that the results of the analysis were credible, the second author engaged in prolonged observation of the data and reviewed ample literature on IPV amongst immigrant and refugee populations prior to beginning the analytic process. Additionally, each source of data was read three times before codes were generated to ensure that the codes and themes would be based on a sound understanding of the data. Furthermore, throughout the analysis, the research team was consulted to review generated codes and themes to promote sufficient elaboration and coherence as well as to review the analytic process itself for fidelity to RTA procedures. To allow for readers to make a sound judgment of the results’ transferability to different situations, the researchers ensured that rich descriptions of the themes were provided along with contextual information that included transcript excerpts (Lincoln & Guba, 1985; Nowell et al., 2017). The researchers also reported demographic information from the participants to aid in judgments about transferability. To promote results’ confirmability (Nowell et al., 2017), a detailed audit trail (Lincoln & Guba, 1985) was created, which included all data, a coding history, a history of the thematic structure developed, and reflective notes from the analytic process (Halpern, 1983; Lincoln & Guba, 1985). The audit trail was evaluated by the third author.
Results
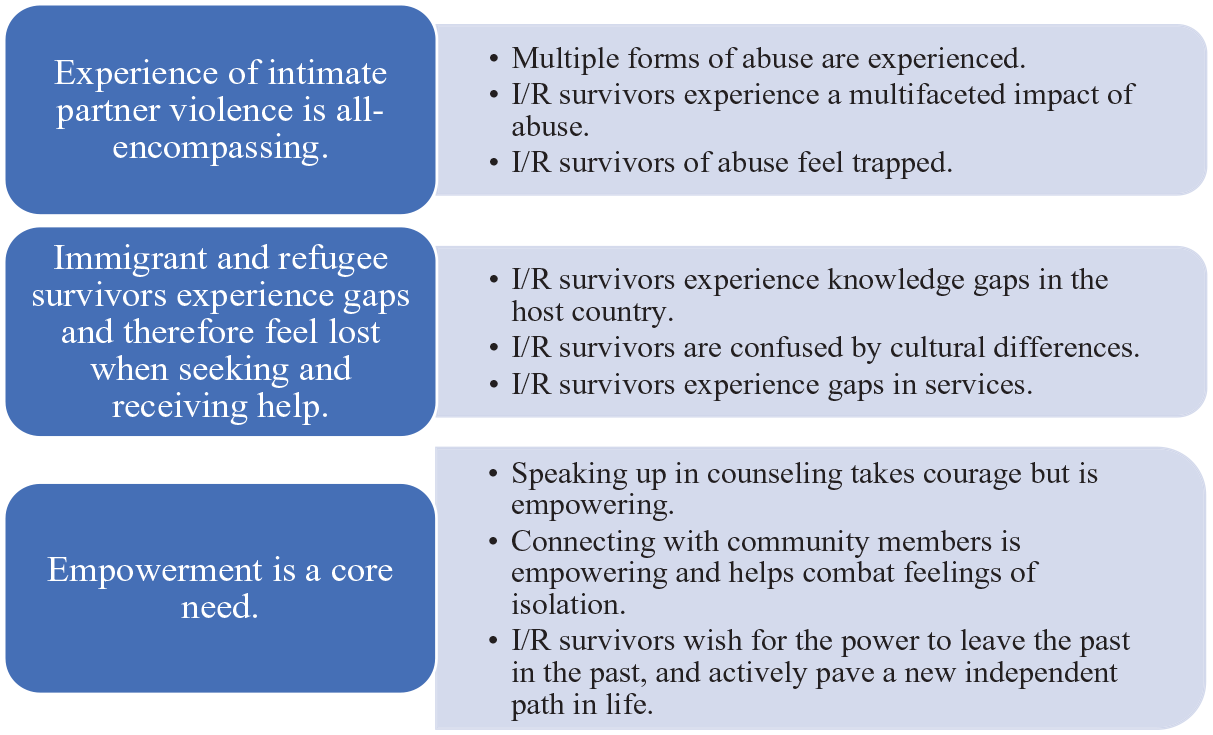
Figure 1 shows the thematic map of the survivors’ journey and recovery process, which includes three macro themes, each of which is built upon smaller subthemes.
Experience of Journey and Recovery Process After Intimate Partner Violence
Theme 1: Experience of IPV Is All-Encompassing
Multiple Forms of Abuse Are Experienced
In many cases, the survivors were abused in multiple different ways. For example, one attendee described, “In my past, I have bad relationship with my ex, and it was hurting me physically, emotionally, everything. And I was in danger.” In addition to physical and psychological abuse, survivors often described the ways in which their abuser took control over different aspects of their lives, such as by limiting the survivors’ autonomy, attempting to control joint property, or claiming financial assets. The following quote presents an example: It is the threats, “I am going to burn it up, I am going to give it to so and so. . .when I came home, he took the lock out, he was gonna lock me out. . .I called the cops. . .But there has been problems now, my problem right now, is I have no job, right? So, he took all the money out of the bank.
Immigrant/Refugee Survivors Experience a Multifaceted Impact of Abuse
These survivors described the complex, multilayered personal and interpersonal impact that the experience of abuse had on them. It was not uncommon for survivors to describe experiencing conflict in interpersonal relationships with family members and significant others. For example, in one instance, the abusive husband sparked an interfamilial conflict by contacting the survivor’s family to attempt to gain property rights, while others described being blamed for the IPV by family members or pressured by them to stay in the abusive relationship. One survivor described that her roommate leveraged the survivor’s situation in a conflict by threatening to contact her former spouse. Such experiences further isolated the survivors.
One survivor’s description of her life after leaving the abusive relationship most clearly highlighted the overall disempowerment and financial impact that remained: For me, I was so controlled, I did not know. I did not know what to cook, because I did not make any choice. He was the one that guided me. So I was just like, “I don’t know what to do. I didn’t have any money.”
Another survivor recounted that she was forced to change her workplace multiple times due to concerns about her former spouse tracking her down and confronting her. The direct effects of IPV often gradually led to a loss of identity. For example, one survivor stated: For me. . .loss of identity. . .I did not know who I was anymore, because coming from a very good profession, I was a journalist, and coming here, and it was absolutely nothing, I even did not know what to do! Where to go! What am I? Who are you? I could not identify who I was as a person and professionally. . .So I was like a ghost.
Immigrant/Refugee Survivors of Abuse Feel Trapped
The confinement that these survivors were made to feel because of the abuse was prominent in the survivors’ accounts of feeling trapped and unable to escape literally and figuratively. The survivors described how difficult it was to take their first steps toward receiving support and attaining safety, causing them to feel stuck and unable to act. Most prominent in their accounts was the fear of social stigma and going against gendered cultural expectations. Many survivors also described that the cultural stigma surrounding divorce, separation, and being a single mother was promoted by family members. The following survivor’s recount especially illustrates this point: One thing is hard for me with my culture, like when I went through the separation time after I got to my 50, so everyone around me like my mom, my aunty, said, “Okay, you get old enough, just don’t divorce. If your husband, he will enjoy the time with another one a little bit, he will come back home, you have a grown-up daughter, so what if she wants to marry? And what people will say? How you will act if they understand after that many years, her parents get divorced?” and blah blah, and yeah, this is part of my culture.
A diminishing of the seriousness of the survivor’s situation related to different conceptualizations of abuse between mainstream culture and their own culture contributed to their feeling trapped. As one survivor described, “the culture I came from, like in my country, we have a different (inaudible), there is a tribe who believe the woman, if the husband did not beat her, that means he did not love her.” Therefore, she partially felt it was wrong not to accept the abuse. Two women also described that the term “abuse” in their culture meant something different from what abuse means in Canada, suggesting that there is a different threshold for what is considered abuse between cultures, and at times this results in women’s call for help not being taken seriously by others, especially by those within her own culture.
Numerous survivors recalled being afraid to call authorities for help because of unfamiliarity with the process, social stigma, and the feared implications of calling out the abuse for the family (e.g., forced separation of the family due to the partner going to jail or the survivor and children going to a shelter). This dilemma further contributed to feeling ensnared. While two survivors described that calling for intervention was eventually helpful, there were more examples of how these survivors felt brushed off or invalidated by the police, which resulted in additional discouragement and disempowerment and an unwillingness to try to take action again.
Theme 2: Immigrant and Refugee Survivors Experience Gaps and Therefore Feel Lost When Seeking or Receiving Support
Immigrant/Refugee Survivors Experience Knowledge Gaps in the Host Country
Lack of knowledge of available support services stood out amongst these survivors’ descriptions of their difficulties in knowing how to find help, as well as in their accounts of what they saw as ways to improve supports for immigrant/refugee survivors of IPV. Some survivors spoke to how they were initially unaware of their rights and that legal action could be taken to ensure their safety (e.g., “I did not know there are so many things that are rights for me in Canada”); some others expressed that education surrounding the law/court systems, child welfare, and the rights that women have in their situations is something that they really wished they had upon arrival in Canada. There also seemed to be some consensus that it would be helpful if newcomers to Canada were all given standard informative material upon arrival regarding governmental and other official supports available to them, including but not limited to those related to IPV. Additionally, in some instances, survivors expressed an unmet need for agencies to proactively connect with immigrants and refugees and provide referrals to community programs to help clients receive multifaceted support above and beyond IPV. This would help prevent them from feeling confused about how to cope or act.
The survivors described that information surrounding the immigration process, the resources that were available to them, and family services was also unfortunately lacking early in their recovery process. Some specific options brought forth by survivors to improve informational support included having welcome centers where survivors could access a variety of information, having educational workshops, improving referral systems, and providing support in filling out various documents. Some survivors also demonstrated a complete gap in knowledge about what resources were available to their children and how they could best support their children.
Immigrant/Refugee Survivors Are Confused by Cultural Differences
These survivors described several cultural differences that played a role in impeding the help-seeking process even after receiving local knowledge or information about available support services. On many occasions, survivors faced ongoing general challenges from being in a country with contrasting values and beliefs. Language barriers were also frequently mentioned as further contributing to cross-cultural confusions. Some survivors mentioned that terms associated with “abuse” in Canada such as “safety,” “domestic violence,” and “well-being” were perplexing to them and, even after repeated explanation, difficult to fully grasp. In addition, the survivors in a few instances expressed personal discomfort with or cultural incongruence when using the word “abuse.” These survivors suggested that it may be helpful to avoid using the word “abuse” to improve the immigrant/refugee women’s willingness to initially access services.
Immigrant/Refugee Survivors Experience Gaps in Services
These survivors’ accounts illustrated the wide variety of needs that they attempted to address or tried to get services for to promote safety and independence in their journey and recovery process after IPV. These needs were not easily fulfilled due to the lack of local/easily commutable or culturally appropriate resources available, particularly those that offered long-term support. In many cases, financial constraints needed to be overcome first before availing oneself of IPV services. For example, survivors often struggled to meet their basic needs (food, shelter, etc.) as well as cover legal fees associated with the IPV. Therefore, free services and the need for monetary resources were paramount. Survivors indicated that vocational support services, such as language training, job training, and further education, were or would have been very helpful to address financial constraints and permit them to better take advantage of available support services and promote recovery over the long term.
Most notably, the survivors’ experiences highlighted the need for services to be available in their first language, and for them to be able to receive support from a person who understands cultural differences that exist between Canada and their country of origin. This was often not available for them. One survivor said, “The best thing is to reach the person who knows the culture better, because. . .it’s easy to explain the situation or scenario.”
Theme 3: Empowerment Is a Core Need
Speaking Up in Counseling Takes Courage but Is Empowering
Many of these survivors expressed that it was challenging to open up about their experiences given the stigma that surrounds abuse, cultural expectations, and feelings of shame and fear. However, when they were given a supportive platform to speak about their experiences, they found it eye-opening, connecting, and empowering. Survivors emphasized that it was important for them to first be able to feel a sense of safety in order to speak about their experiences and achieve empowerment, and counseling seems to have been a helpful platform for many survivors to become empowered. For example, one survivor explained: I had come for counseling, that really helped, ‘cause it was like I had a whole lot bottled up, no one to or you’re scared someone is gonna judge you, you can’t speak out, then because where we come from, women we don’t have that voice. You are silenced. . .Even if you speak up it’s like, “Oh please, you are a woman, sit down.” You know? That type of thing. So we don’t have a voice. And coming here, you know, coming for counseling, it opens up a whole lot of things for you. It’s like an eye-opener, like you are not alone.
To establish safety, some survivors noted that it is important for counselors to recognize that it may take time for survivors to be able to trust the counselor, given that they would normally look to close friends and family for support in their culture. They further reiterated that it was or would be most helpful to be able to receive support from professionals of the same ethnicity. One survivor said, “The best thing is to reach the person who knows the culture better, because if you got the person or counselor from same culture, it’s easy to explain the situation or scenario.”
Connecting With Community Members Is Empowering and Helps Combat Feelings of Isolation
Many of these survivors expressed the helpfulness of connecting with peers and community members. While a few reported that family was a source of support, most survivors described feeling isolated and insufficient support as a result of relocation and alienation from family, and they mentioned this very often. The benefits of feeling a part of any community and having opportunities to engage rather than isolate seemed to support the women’s desire to feel empowerment and increase their motivation levels. For this reason, group formats for wraparound community services for immigrants and refugees beyond just counseling were frequently mentioned as being very beneficial. Survivors especially spoke about how they were able to gain new perspectives on their situation through hearing stories of other survivors, and how they felt empowered and supported by knowing that they were not alone. One survivor explained: We learn new things from each other; we listen to other people’s stories, and we learn from them; we learn how next time to proceed in terms of our safety, how to take care of the family, how to take care of ourselves.
Immigrant/Refugee Survivors Wish for the Power to Leave the Past in the Past and Actively Pave a New Independent Path in Life
Many survivors expressed a strong desire to move beyond the past and receive support to galvanize their power to become self-sufficient and move forward in life. As one survivor put it: We have to look after ourselves. . .The past is the past and we have to be strong, and we have to see if it is happening or it continue in our relationship, so we have to be strong now and fight and be like you know! We have to protect ourselves and our kids.
In some instances, survivors regaining a sense of self-worth and agency was an important first step that emboldened them toward healing. These survivors eventually became focused on gaining a sense of personal strength as they worked toward independence. They noted that dwelling on the past made this more difficult. To demonstrate this point, one survivor described how she did not wish to use the word “victim” anymore because of how disempowered it made her feel and because it took the attention away from her capabilities and agency over her own life. Underlining the survivors’ accounts was the sense of personal responsibility in rebuilding a new life. Survivors also commonly indicated that they valued education about self-care so that they maintained the energy to work toward self-sufficiency and independence.
Discussion
This study analyzed survivor-only IPV advisory board transcripts to capture their lived experiences of IPV and of support and their wisdom about what was or would have been (more) helpful. What emerged was a collective account of the typical and most sought-after journey and recovery process after IPV for these immigrant and refugee survivors.
Collective Story of Their Journey and Recovery
As anticipated (Du Mont & Forte, 2012), the experience of IPV for these survivors was all-encompassing. These survivors had usually faced several types of abuse concurrently, the impact of which was multifaceted and all-consuming in their lives, which is consistent with past research (Okeke-Ihejirika et al., 2022). The IPV exerted a considerable psychological impact and affected all/most aspects of the survivor’s life, including family relationships, non-family relationships, financial circumstances, and employment. As a result of this abuse, its impacts, gendered cultural expectations, family and social stigma, different cultural definitions of abuse, minimization/denial by others, unfamiliarity with the law enforcement/legal process, and fear of forced family separation, the survivors felt discouraged and disempowered and therefore trapped (metaphorically and literally). The survivors reported various gaps in knowledge about local culture, laws, and official systems of support. This resulted in confusion, disorientation, and difficulty knowing where to go and what to do to obtain desired help. After they received useful knowledge or information about support services, language difficulties and challenges with navigating a different local culture (including understanding what is and is not considered IPV) further contributed to a sort of metaphorical paralysis. Even after identifying and attempting to utilize an available service, language difficulties, transportation difficulties, and financial difficulties often prevented them from being able to utilize official services and second-language services and the cultural inappropriateness of those services often led to unsatisfactory results. Clearly, immigrant and refugee survivors have many IPV-relevant experiences related to the settlement process that many locally born women do not (American Psychiatric Association, 2019; Okeke-Ihejirika et al., 2020).
In terms of their recovery process, these women realized that dwelling on their past misfortunes was counterproductive and hindered their newfound personal responsibility for rebuilding their lives. This was something that they had to try especially hard to overcome. They saw empowerment as a core need and necessity because the experience of IPV was very disempowering. They described that, although challenging to initiate, speaking up about their experiences, especially through counseling and connecting with supportive community members or others experiencing IPV, helped them feel better about themselves and empowered them to act toward building a new future. The social connections developed further provided motivation and strength. What these survivors most wanted was to leave the past in the past and actively pave a new independent pathway for their lives and the lives of their children.
Comparison With Existing Literature
The immigrant/refugee survivor’s experience is not wholly distinct from that of the locally born survivor (e.g., see Du Mont & Forte, 2012). As indicated by the current study’s results, the experience of IPV as all-encompassing with multiple forms of abuse likely to be perpetrated with a multifaceted impact on so many aspects of the survivor’s life, and feeling trapped as a result, appear to be common factors in the IPV experience, as verified in numerous past research studies (e.g., see the review of Okeke-Ihejirika et al., 2020). The same can be said about the importance of feeling empowered, connecting with a supportive community, receiving counseling, and building a different life in the future for successful recovery (Du Mont & Forte, 2012; Okeke-Ihejirika et al., 2020). But this study reported on experiences relatively unique to the immigrant/refugee survivor, including those related to cultural safety (Curtis et al., 2019).
The current study’s results generally replicate what has been found in the little existing research on IPV with immigrants and refugee survivors that exists (e.g., see the review of Okeke-Ihejirika et al., 2020). This is important because women on IPV survivor advisory boards and the boards themselves have rarely, if ever, been directly investigated. Therefore, comparing existing findings with those for this new type of research participant strengthens the credibility, transferability, dependability, and confirmability of past research findings. The current study’s results imply that the immigration and settlement process can instigate and maintain IPV in a manner not common amongst locally born women and that there are relatively distinct risk and protective factors for immigrant and refugee women (Sabri et al., 2018), such as acculturation and cross-cultural confusion, learning a new local language, laws and rights in the host country, social/family isolation due to relocation to a new country, inability to leave due to citizenship requirements, economic necessity, and lack of a work permit. The study results also replicate past findings that many immigrant and refugee women come with culturally distinct understandings of IPV and levels of seriousness not easily reconcilable with norms in Western countries (Okeke-Ihejirika et al., 2020; Sabri et al., 2018). For example, in their country of origin, some participants reported that certain things considered IPV in Canada were accepted or encouraged by many and that partner abuse by a man was commonly seen as a sign of love and mattering. Our results further duplicate past research that concludes that many immigrant and refugee survivors select the well-being and stability of their families over their personal well-being and are quite hesitant to disclose the abuse, get a separation, or access professional support services (Okeke-Ihejirika et al., 2020). Furthermore, our results are consistent with growing research showing that immigrant and refugee survivors’ reluctance to access official help has partly to do with (a) many IPV services’ failure to provide first-language, culturally safe, and adapted services that consider the settlement experience and (b) biased laws and policies that significantly disadvantage immigrants and refugees (Okeke-Ihejirika et al., 2020).
This study’s results also corroborate many of the findings of research on IPV peer-support groups (e.g., Tutty et al., 2017). For example, the theme of empowerment was also central in the stories of the non-White peer-support group survivors in Page et al. (2021), and their other themes of Transformation, Community, and Awakening have clear analogs with the themes and subthemes in the current study. There was no clear theme analog to their category of Advocate (a desire to advocate by helping women who face similar circumstances) in the current study, but this was implied given these survivors’ participation in an advisory board.
Compared to much past research on immigrant and refugee survivors, the survivors in the current study did not emphasize the helpful use of emotion-focused coping strategies such as relying on faith, accepting responsibility for the abuse, distracting themselves, normalizing the abuse, and avoiding violence-inducing circumstances (Okeke-Ihejirika et al., 2020). Instead, the survivors emphasized problem-focused coping (disclosing the abuse, accessing official support, getting a separation, calling the police), as is more common amongst locally born survivors in Western countries (Okeke-Ihejirika et al., 2020). However, this could be due to the inclusion criteria for the study—all survivors had previously received or were currently receiving counseling services and thus represented those who would and did already engage in problem-focused coping strategies or were trained in such through counseling. Due to the self-selected nature of survivors who choose to join an advisory board, it would have been difficult to get immigrant and refugee survivors who prioritize emotion-focused coping strategies to join and share their wisdom in this format. In addition, the survivors in the current study were strongly pro-counseling, unlike much of what was reported in past literature (e.g., Simon-Kumar et al., 2017). Unlike many immigrants and refugee survivors, these survivors also appear to be the rare ones who received culturally safe and adapted counseling from a culturally competent counselors (Curtis et al., 2019), and this likely contributed to their flattering view of counseling.
Implications of the Results
The results from these advisory board meetings had an immediate impact on the community organization’s IPV programming. For example, the organization reported that they intended to continue the advisory board past this initial pilot of it. Several aspects of the feedback were implemented (e.g., focus on developing and promoting wraparound services for survivors outside of IPV services and focus more on risk/protective factors). In addition, to address the women’s knowledge gaps about the legal system, the organization planned to involve advisory board members in educating local law enforcement and other allied governmental and nongovernmental organizations about supporting immigrant/refugee IPV survivors. The hope was, through this outreach work, the local law enforcement could become more familiar with the type of support from which IPV survivors would most benefit from.
For community organizations, this study promotes the wider adoption of survivor-only advisory boards to develop and modify IPV programming. It also promotes wraparound services for immigrant and refugee women given the successful implementation of the survivor-only advisory board in this project and the changes implemented as a result of this feedback. Becoming actively involved in public education and outreach campaigns to increase awareness of IPV as defined locally and reduce community stigma across various cultural groups would likely increase uptake of services (Critelli & Yalim, 2019). So would educating local immigrant and refugee communities on laws and their rights relevant to IPV, the court system, and what happens when the abuse is reported to different types of authorities or professionals (Reina & Lohman, 2015). It would also be helpful if newcomers to Canada were given standard informative material upon arrival to Canada regarding governmental and other official supports available to them, including but not limited to those related to IPV—something that could be accomplished by setting up immigrant and refugee welcome centers at nonprofit organizations. Because language barriers often prevent immigrant and refugee survivors from availing themselves of IPV and mental health services, it is vital that the above be available in as many locally spoken languages as possible (Critelli & Yalim, 2019). Many of these survivors suggested that it may be helpful to avoid using the word “abuse” to improve immigrant and refugee women’s willingness to access IPV services, so the programs’ titles should be carefully considered to increase uptake. Many of these survivors had to focus first on basic human needs that they struggled to address (food, shelter, etc.) before they had the time, energy, or resources to take advantage of IPV services and wished for more financial aid, legal aid, and wraparound services (language training, vocational training, job search support, food banks, education services, financial literacy programs, etc.) before or in conjunction with IPV services, which is important feedback for community organizations to heed. Feeling part of a community and having opportunities to engage rather than isolate were reported by the women to help feel more empowered to actively address IPV. Therefore, the availability of community-connecting and community-building activities unrelated to settlement or IPV is also important (e.g., community kitchens, celebrating local festivals). Therefore, group formats for wraparound community services beyond just counseling are advised.
These survivors also provided specific advice and guidance for mental health professionals to help counseling be a more culturally safe and effective intervention. Two examples of cultural adaptations reported frequently included having resources available in different languages and increasing the duration of sessions in order to build trust over time for more casual dialog and mutual sharing. The participants also highlighted the need for services to be available in their first language, and for them to be able to receive support from a person who strongly understood the cultural differences that exist between Canada and their country of origin, which was often not available in their experience. Although research is pretty equivocal about whether racial/ethnic matching between counselor and client results in better therapeutic outcomes (Cabral & Smith, 2011), it may result in immigrant and refugee survivors being more willing to try counseling initially due to the common belief that only someone from their own culture could understand their experiences. Nevertheless, because many immigrants and refugees are more accustomed to seeking help from family and community leaders (Curtis et al., 2019), it may take longer to develop trust and safety with a counselor, so counselors need to be willing to spend extra time and sessions on developing a strong therapeutic alliance with the client (Horvath & Bedi, 2002)—thus, standard session limits may need to be relaxed in order to provide sufficient benefit for immigrant or refugee IPV survivors.
Based on this study’s results, researchers are further justified in investigating survivor-only advisory boards and tapping into the wisdom of this under-investigated group of survivors who are disproportionately the success stories and extremely willing to share their expertise. There are also many analogies between peer-support groups for IPV, which have been repeatedly shown to be effective (e.g., Tutty et al., 2017), and a survivor-only advisory panel. Thus, there could be therapeutic benefits for these advisory board survivors, which should be investigated in future research. Therefore, advisory board membership might eventually also be considered a therapeutic intervention in itself.
Limitations of the Study
In generating representative themes, this study focused on commonalities across survivor narratives, which necessarily obscured dissimilarities and nuances between the individual lived experiences of the survivors who contributed to this study and renders the study unable to comment on idiosyncratic experiences. Another limitation pertains to this study’s sampling. The study made use of survivors who were part of an IPV advisory board who had previously received IPV counseling services, presumably had some notable degree of success, and were highly motivated to share ideas on what would help others in similar circumstances. The comments that would be provided from those who did not feelable, comfortable, or willing to participate in an IPV advisory board, which presumably may be the majority of survivors of IPV, could be somewhat different. In addition, it could have been that participating in an advisory board impacted these survivors’ understandings of their experiences, possibly not only by helping them become more self-aware but also by creating some novel thoughts that would not have been possible without participation in an advisory board. Furthermore, although this study focused on women immigrant/refugee IPV survivors and their experiences, they often discussed the IPV experiences of men who were the perpetrators. Noting that there is an extreme dearth of research on Canadian immigrant/refugee men who are perpetrators (and victims) of IPV (Okeke-Ihejirika et al., 2020), additional insights about IPV among immigrant/refugee women and guidance for service providers and policy-makers can be gleaned by more research with immigrant/refugee men involved in IPV.
The advisory boards were conducted in an urban city that houses amongst the largest number of immigrants and refugees in Canada (Statistics Canada, 2022). The study results may have differed if sampling was from rural areas or locations with few immigrants and refugees. In addition, the experiences of the survivors in this study are necessarily contextualized by Canadian and British Columbian laws and court precedents, and thus, careful consideration needs to be done before transferring this study’s results and implications to another geographical context.
Strengths of the Study
The follow-up questionnaire administered to the advisory board members garnered an 80% response rate, indicating strong investment of the members in the advisory board, which bodes well for the credibility of their responses. In addition, much qualitative research on women survivors of IPV, including with immigrants and refugees, is based on single-meeting interviews or single advisory boards (Okeke-Ihejirika et al., 2020). However, there is ample evidence of the difficulty immigrant and refugee survivors have, including from this study, in feeling safe and trusting enough to openly discuss their experiences, especially in a second language (e.g., Simon-Kumar et al., 2017). Therefore, there is always some question about the veracity and completeness of single-meeting interviews and advisory boards, which are the norm. However, in this study, survivors attended multiple advisory board meetings and thus had time to develop a greater sense of trust and safety, which should have promoted the veracity and completeness of their disclosures. Moreover, unlike research conducted on peer-support groups (e.g., Tutty et al., 2017), research on advisory board meetings alleviates the additional emotional investment of giving and receiving peer support. Therefore, survivors on advisory boards are permitted more opportunity to engage in deeper retrospective self-analysis, to “look at the bigger picture” beyond just their own experiences, and to contribute ideas about what was or would have been helpful for them and other women in similar circumstances. In other words, the sole focus of advisory board meetings is on sharing wisdom and trying to promote systemic change—providing more of the content needed by researchers.
Conclusion
This study contributes to a more nuanced understanding of IPV and its risk and protective factors for immigrant and refugee women and reinforces that there are key differences from how locally born women navigate IPV. In addition, this study’s results offer service providers and community organizations valuable guidance on how to maximize services uptake and provide culturally safe and effective services for immigrant and refugee survivors of IPV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was based on a program grant funded by Status of Women Canada with funding awarded to DIVERSEcity Community Resources Society and internal funding provided by the University of British Columbia Faculty of Education under their Research Infrastructure Support Program.