
Abstract
Although women outlive men, women report poorer self-rated physical health over much of the lifespan. Objectification theory may offer insight into this gender difference. Objectifying culture promotes self-surveillance, which encourages prioritizing the body’s appearance over its physical functioning and well-being. As women may engage in self-surveillance more so than men, this sequence of events may help explain this gender difference in self-rated health. However, the few studies examining this idea show an inconsistent relationship between self-surveillance and self-rated health. Nonetheless, self-surveillance may promote body shame and diminished awareness of internal bodily states. As these factors are associated with poor self-rated health, self-surveillance may predict poor self-rated health via these mechanisms. In study 1 (N = 166 undergraduate women), self-surveillance was unrelated to self-rated health. However, body shame and low interoceptive awareness mediated this relationship. In study 2 (N = 347 undergraduate women and men), self-surveillance correlated negatively with self-rated health for female participants but not male participants. Female participants reported poorer self-rated health, and this effect was serially mediated by self-surveillance, body shame, and low body responsiveness. These studies suggest a potential avenue by which self-surveillance may explain the gender difference in self-rated health in college samples, providing an important basis for future longitudinal investigations in more diverse samples. Moreover, these results suggest that interventions targeting body shame and low internal awareness may be used to promote good self-rated health as well as to prevent disease and poor health behaviors related to self-rated health.
Global mortality rates suggest that women outlive men across most of the world (World Health Organization, 2022). Despite this apparent advantage in longevity, women generally report lower self-rated health than do men (Case & Paxson, 2005; Idler & Benyamini, 1997; Phillips et al., 2023). Self-ratings of health are valid and powerful indicator of a person’s physical health status, reflecting respondents’ physical rather than mental health (Smith et al., 1999), converging strongly with objective measures of health (e.g., chronic conditions, functional disability, Leger et al., 2015) and predicting mortality above and beyond health behaviors (Idler & Benyamini, 1997). That is, while their lives may be longer, women may be more likely to experience poorer health during them. This gender difference in self-rated health has been identified in adolescence and young adulthood (Chen & Lucock, 2022; Jerdén et al., 2011; Vaez & Laflamme, 2003; Yoo & Jang, 2023) and has been shown to persist into late middle age (McCullough & Laurenceau, 2004; Rani et al., 2022). It has been identified across many countries, races, and ethnicities (Cummings & Braboy Jackson, 2008; Oksuzyan et al., 2009; Tabler & Painter, 2023). It has not been well explained by biology (e.g., hormones, Rieker & Bird, 2005), behavioral risk (e.g., smoking, van Oyen et al., 2013), or self-report factors (Oksuzyan et al., 2009; Phillips et al., 2023) alone. However, sociocultural explanations for this gender difference offer several promising leads. For example, women more so than men experience sexism, lower access to resources, poorer healthcare, and gender-based violence. These sociocultural factors may combine with biological, psychological, and behavioral factors to negatively impact women’s self-rated health (Spitzer, 2005). Discerning possible reasons for this gender difference in self-rated health may inform health promotion and disease prevention in women, making women’s longer lives more enjoyable to lead (Phillips et al., 2023).
Self-Surveillance and Self-Rated Health
Another sociocultural model that may help explain this gender difference in self-rated health is objectification theory (Fredrickson & Roberts, 1997; Moradi & Huang, 2008). This model proposes that women more so than men experience objectification or being valued as a body for visual and sexual consumption by others, while their subjective, internal experience is discounted. Women’s bodies are evaluated against body ideals comprising a visually appealing appearance devoid of natural bodily functions (Roberts & Goldenberg, 2007). Women are taught that their self-worth depends upon meeting these ideals (Fredrickson & Roberts, 1997) and are punished interpersonally and economically for not meeting them (Fikkan & Rothblum, 2012; Frieze et al., 1991). Thus, women may engage in self-surveillance, or the habitual self-monitoring of the body’s appearance and functions, that prioritizes an outsider’s view of their own bodies over their own inner experience (McKinley & Hyde, 1996; Murray et al., 2023). Self-surveillance occurs for women across ethnicities and cultures (Moradi & Huang, 2008; Schaefer et al., 2018) and across much of the lifespan, especially from adolescence to middle age (McKinley, 2011). Finally, women’s internalization of body ideals occurs despite recent positive body image ad campaigns (Couture Bue & Harrison, 2019; Selensky & Carels, 2021).
Self-surveillance may have implications for women’s self-rated physical health. In self-surveillance, the body’s appearance is valued over its internal experience, including both subjective feelings and the body’s physical functioning (Fredrickson & Roberts, 1997). As the body’s physical functioning is part and parcel of physical health, this form-over-function imperative would logically be linked to self-rated physical health. Indeed, self-surveillance has already been tied to poor health behaviors in which the body’s appearance is prioritized over the body’s physical health. For example, self-surveillance has been linked to restrained eating (McKinley, 2006; Slater & Tiggemann, 2002), cigarette smoking (Fiissel & Lafreniere, 2006), indoor tanning (Choukas-Bradley et al., 2019), and willingness to undergo elective cosmetic surgery (Vaughan-Turnbull & Lewis, 2015). In these behaviors, aligning the body’s appearance with objectified body ideals takes precedence over the body’s physical health. It would be reasonable to expect a similar relationship between self-surveillance and self-rated health.
Nonetheless, the link between self-surveillance and health behaviors has proven complex. Indeed, self-surveillance is sometimes unrelated to health behaviors and may even predict beneficial health behaviors. For example, Greenleaf (2005) found self-surveillance to be negatively related to physical activity in older women but not in younger women. Self-objectification, a self-surveillance-like state in which the appearance of the body is also valued over its subjective experience, has also been inconsistently related to exercise, predicting decreases in some types of exercise (e.g., yoga) and increases in other types (e.g., individual cardio), and having no relationship to still other types (e.g., weight training, Prichard & Tiggemann, 2008). Self-surveillance has been negatively correlated with preventative sexual health behaviors (Ramseyer Winter, 2017), but increasing the similar state of self-objectification predicts increased intentions to perform breast self-exams (Morris et al., 2012). Finally, Ertl et al. (2022) found self-surveillance to be associated with increased condom use, a risk-reducing sexual health behavior, but also greater number of sexual partners, a potentially risky sexual health behavior. Such inconsistency may suggest that self-surveillance produces multifaceted effects on health behaviors: some positive and some negative.
Such complexity may extend to the link between self-surveillance and self-rated health. Despite the dire implications that the form-over-function doctrine may logically present for self-rated health, the few studies examining this link reveal no connection. Sveinsdóttir (2017) found self-surveillance to be unrelated to self-ratings of physical health-related quality of life in women. Rollero and De Piccoli (2015) found that although women scored higher on self-surveillance and lower on self-rated health than men, self-surveillance only predicted poorer self-rated health in men. Baceviciene et al. (2022) found that self-objectification was negatively correlated with self-rated health in adolescent girls but uncorrelated with self-rated health in adolescent boys. Based on these studies alone, one might conclude that the relationship between self-surveillance and self-rated health is inconsistent at best. However, given the reasonable connection between the form-over-function directive and self-rated health, a reliable link between self-surveillance and self-rated health may yet exist. This link, however, may be more complex than its bivariate correlation lets on. As with health behaviors, self-surveillance may be related to many processes, some that benefit self-rated health, but some that may detract from it. As such, the sum total of the relationships between self-surveillance and self-rated health may at times be nonsignificant. Teasing out the reasons for this inconsistent link could reveal important mechanisms by which self-surveillance may be associated with self-rated health, thereby identifying novel avenues for health promotion and disease prevention.
A Mechanistic Approach
Indeed, whether self-surveillance is associated with poor self-rated health in women may depend on the mechanisms by which this relationship occurs. One of these mechanisms is body shame (Fredrickson et al., 1998; Noll & Fredrickson, 1998). Body shame is a negative self-conscious response to a perceived failure to meet objectified body ideals, a failure that is then attributed to immutable flaws in the self (Fredrickson & Roberts, 1997). As objectified body ideals are virtually impossible to meet (Noll & Fredrickson, 1998), especially for women, women may perceive that they fall short and experience body shame more so than men (Lamont, 2021; McKinley, 2006). Several cross-sectional studies have revealed a positive correlation between self-surveillance and body shame (Augustus-Horvath & Tylka, 2009; Holmes & Johnson, 2017; Kozee & Tylka, 2006; Tylka & Hill, 2004; Watson et al., 2013). Moreover, experimentally induced self-objectification, a self-surveillance-like state, has been shown in many investigations to increase body shame (Dimas et al., 2021; Fredrickson et al., 1998; Hebl et al., 2004).
In turn, body shame may encourage diminished awareness of internal bodily states. Indeed, Western body ideals also condemn natural bodily processes and encourage their concealment. Functions like sweating, menstruation, and body hair growth are to be hidden at all costs, especially for women (Roberts & Goldenberg, 2007). Thus, body shame may cause women more so than men to distance themselves from their internal bodily functions, thereby becoming less aware of the processes occurring within their own bodies (Lamont, 2021). Body shame has been associated with deficits in interoceptive awareness or attention to internal bodily functions (Augustus-Horvath & Tylka, 2009; Holmes & Johnson, 2017; Tylka & Hill, 2004; Watson et al., 2013). Moreover, body shame has also been linked to diminished body responsiveness or the awareness and valuing of bodily functions as a source of information (Lamont, 2015, 2019). Furthermore, experimentally induced body shame has been shown to be associated with subsequent decreases in state body responsiveness (Lamont, 2021). Importantly, Dimas et al. (2021) showed that although a self-objectification induction increased body shame, it did not directly influence state interoceptive awareness. Taken together, these experiments may suggest body shame as a necessary bridge between self-surveillance and diminished internal awareness.
Finally, diminished internal awareness may promote poor self-rated physical health. Body responsiveness has been shown to correlate negatively with poor health outcomes (Lamont, 2015, 2019). Moreover, interoceptive awareness has been shown to correlate negatively with pain symptoms (Duschek et al., 2017). In a longitudinal study, Lamont (2015) demonstrated that body responsiveness at the beginning of the semester were associated with poor self-rated health, increased physical symptoms, and increased infections in college women. Importantly, physical health outcomes at the beginning of the semester were not associated with body responsiveness at the end of the semester, supporting the temporal precedence of body responsiveness in that relationship. Additionally, in patient populations, internal awareness interventions have shown subsequent decreases in physical symptoms and increases in quality of life (Landsman-Dijkstra et al., 2004) as well as decreased pain symptoms (Courtois et al., 2015; Zucker et al., 2017).
Thus, self-surveillance may be associated with poor self-rated health through the mechanisms of body shame and low awareness of internal bodily states, particularly for women. Several cross-sectional studies support a similar model, where self-surveillance is associated with poor health behaviors through the mechanisms of body shame and low awareness of internal bodily states. In these studies, self-surveillance has been shown to correlate with high body shame and in turn low interoceptive awareness, which ultimately was associated with disordered eating, which is a poor health behavior in both undergraduate and community women (Augustus-Horvath & Tylka, 2009; Kozee & Tylka, 2006; Tylka & Hill, 2004). This same serial path has been shown to emerge in more complex models that include additional variables like sexual victimization (Holmes & Johnson, 2017) and racial identity (Watson et al., 2013).
If the serial cascade of self-objectification, body shame, and low internal awareness is associated with poor health behaviors, then it is reasonable to expect that this same progression of factors would be associated with poor self-rated health. Although both Sveinsdóttir (2017) and Rollero and De Piccoli (2015) measured body shame in their investigations, neither tested whether body shame mediated the link between self-surveillance and self-ratings of health. Moreover, neither these investigators nor Baceviciene et al. (2022) examined the potential role of awareness of internal bodily processes in this relationship. Thus, what is missing from the current literature is a test of whether self-surveillance is associated with poor self-rated health via the likely mechanisms of body shame and diminished awareness of internal bodily processes. Finally, if self-surveillance is indeed linked to poor self-rated health through these mechanisms, it may help to explain why women experience poorer self-rated health than do men.
The Current Investigation
The current investigation aimed to fill these gaps. Two cross-sectional studies tested whether self-surveillance was associated with poor self-rated health, whether body shame and diminished awareness of internal bodily functions mediated this relationship, and whether self-surveillance and its sequelae may explain the gender difference in self-rated health. Study 1 tested this model in a sample of undergraduate women, and study 2 tested this model in undergraduate women and men.
Study 1
The purpose of study 1 was to test whether self-surveillance was associated with poor self-rated health through the mechanisms of body shame and poor awareness of internal bodily states in a sample of undergraduate women. Poor awareness of internal bodily states was defined as low interoceptive awareness. Moreover, body mass index (BMI) and eating disorder risk were included as covariates. Although self-surveillance is inconsistently related to BMI, BMI has been reliably associated with body shame (Daubenmier, 2005; McKinley, 2006) and diminished self-rated health (Lamont, 2015, 2019; Rollero & De Piccoli, 2015). It is possible that the proposed associations are limited to the higher end of the BMI spectrum. Moreover, self-surveillance, body shame, and poor internal awareness have all been linked to disordered eating (Augustus-Horvath & Tylka, 2009; Holmes & Johnson, 2017; Kozee & Tylka, 2006; Tiggemann & Williams, 2012; Tylka & Hill, 2004; Watson et al., 2013), which in turn has been linked to poor physical health (Kärkkäinen et al., 2018; Landstedt et al., 2018), thus confounding poor psychological and physical health.
The following hypotheses were made. First, given prior research showing an inconsistent relationship between self-surveillance or self-objectification and self-rated health (Baceviciene et al., 2022; Rollero & De Piccoli, 2015; Sveinsdóttir, 2017), no hypothesis was made for the bivariate relationship between self-surveillance and self-rated health. Also based on previous research (Lamont, 2015, 2019), it was hypothesized that (H1a) body shame would correlate negatively with self-rated health and that (H1b) interoceptive awareness would correlate positively with self-rated health. Finally, it was hypothesized that (H1c) body shame and poor interoceptive awareness would serially mediate the link between self-surveillance and self-rated health. Specifically, it was expected that self-surveillance would predict high body shame, which in turn would predict low interoceptive awareness, which would ultimately predict poor self-rated health.
Method
Participants
One-hundred seventy-seven undergraduate women at a small liberal arts college completed the study and received course credit in return. Participants were not included in the study if they were not women or if they were not in a class in which course credit was offered in exchange for participation. Some participants completed the survey more than once, and those duplicate responses (n = 11) were removed from analyses. This method left 166 participants in the final sample (age, M = 25.58, SD = 6.31). These participants self-identified as White (82.5%), Black or African-American (5.4%), mixed race or biracial (6.0%), Hispanic or Latina (3.0%), and Asian (2.4%), with 0.6% not reporting ethnicity.
Materials
Demographics
To measure gender, participants responded to the open-ended question, “What is your gender?” To measure race or ethnicity, participants responded to the open-ended question, “What is your race or ethnicity?” Participant age was calculated by subtracting the participants’ self-reported birthdate from the date the participant completed the survey and dividing by 365. Participants responded to the open-ended questions, “What is your height in feet and inches?” and “What is your weight in pounds?” To calculate BMI, participant height was converted into inches, and that number and weight in pounds was entered into the standard BMI formula, BMI = (weight/[height]2) × 703.
Self-Surveillance
The surveillance subscale of the Objectified Body Consciousness Scale (OBC; McKinley & Hyde, 1996) was used to measure self-surveillance. This subscale contains eight items that assess valuing form-over-function (e.g., “I think more about how my body feels than how it looks” [r]) and preoccupation with appearance (“I rarely think about how I look” [r]). Participants responded to each item on a 1 (strongly disagree) through 5 (strongly agree) scale. After reverse-scoring (r) items, all items were combined to create a mean self-surveillance score for each participant, with higher scores representing higher levels of self-surveillance. This measure has been shown to be highly correlated with similar measures like self-objectification (Vaughan-Turnbull & Lewis, 2015) but distinct from body shame (McKinley & Hyde, 1996). This measure has demonstrated good internal reliability in previous investigations (e.g., α = .79, Holmes & Johnson, 2017; α = .87, Tylka & Hill, 2004) as well as in the current study, α = .86.
Body Shame
The body shame subscale of the Objectified Body Consciousness Scale (OBC; McKinley & Hyde, 1996) was used to measure body shame. This subscale contains eight items that assess shame about the body (e.g., “When I’m not the size I think I should be, I feel ashamed”) and global attributions of the failure to meet body ideals to the self (e.g., ‘Even when I can’t control my weight, I think I’m an okay person’ [r]). Participants responded to each item on a 1 (strongly disagree) through 5 (strongly agree) scale. After reverse-scoring (r) items, all items were combined to create a mean body shame score for each participant, with higher scores meaning higher levels of body shame. This measure is distinct from constructs such as appearance anxiety (Watson et al., 2013). This measure has demonstrated good internal reliability in previous studies (e.g., α = .85, Holmes & Johnson, 2017; α = .83, Tylka & Hill, 2004) as well as in the current study, α = .84.
Interoceptive Awareness
The interoceptive awareness subscale of the Eating Disorders Inventory (EDI; Garner et al., 1983) was used to measure interoceptive awareness. This subscale contains 10 items that assess the ability to detect internal functions (e.g., “I don’t know what’s going on inside me” (r); “I can clearly identify what emotion I am feeling”). Participants responded to each item on a 1 (strongly disagree) through 5 (strongly agree) scale. After reverse-scoring (r) items, all items were combined to create a mean interoceptive awareness score for each participant, with higher scores meaning greater interoceptive awareness. This measure has demonstrated good internal reliability in previous studies (e.g., α = .86, Holmes & Johnson, 2017; α = .82, Tylka & Hill, 2004) as well as in the current study, α = .89.
Self-Rated Health
Self-rated health was measured using the standard single-item measure, “In general, my health is. . .,” to which participants responded on a scale of 1 (poor), 2 (fair), 3 (good), 4 (very good), or 5 (excellent). Single-item self-rated health measures have been shown to converge reliably with health-related outcomes in college populations (Lamont, 2015, 2019) and to be associated with mortality in community studies more effectively than physician’s assessments (Idler & Benyamini, 1997).
Eating Disorder Risk
Eating disorder risk was measured using the 26-item Eating Attitudes Test (EAT; Garner et al., 1982). This measure contains 13 items assessing restrained eating (e.g., “I engage in dieting behavior”), six items measuring bulimia behaviors (e.g., “I feel that food controls my life”), and seven items measuring oral control (e.g., “I take longer than others to eat my meals”). Participants responded to each item on a 1 (strongly disagree) through 5 (strongly agree) scale. After reverse-scoring (r) items, all items were combined to create a mean eating disorder risk score for each participant, with higher scores meaning greater eating disorder risk. As in prior studies with non-clinical samples, this measure was treated as continuous (Daubenmier, 2005; Slater & Tiggemann, 2002). This measure has demonstrated good internal reliability in previous studies (e.g., α = .87, Holmes & Johnson, 2017; α = .91, Tylka & Hill, 2004) as well as in the current study, α = .88.
Procedure
Study procedures were approved by the Bellarmine University Institutional Review Board. Participants were recruited over email for a study on personality and health. All research materials were administered by a female research assistant and completed in a campus computer lab. No more than 10 participants at a time were present in each data collection session, and participants were separated by privacy screens. After providing informed consent, participants completed all research materials on a computer, beginning with health-related and demographic items and followed by randomly-presented trait measures. Other variables (e.g., authoritarian parenting) served as filler items. Analyses on these items are not reported here.
Results
All data were analyzed using the SPSS Statistical Package v28.0. To examine the link between self-surveillance and self-rated health as well as to test the first two hypotheses, bivariate correlations were run. Consistent with Sveinsdóttir (2017) and Rollero and De Piccoli (2015), but contrary to Baceviciene et al. (2022), self-surveillance was unrelated to self-rated health. However, as expected (H1a), body shame was negatively correlated with self-rated health, and (H1b), interoceptive awareness was positively correlated with self-rated health. These results appear in Table 1.
Means, Standard Deviations, and Bivariate Correlations for Study 2 Variables
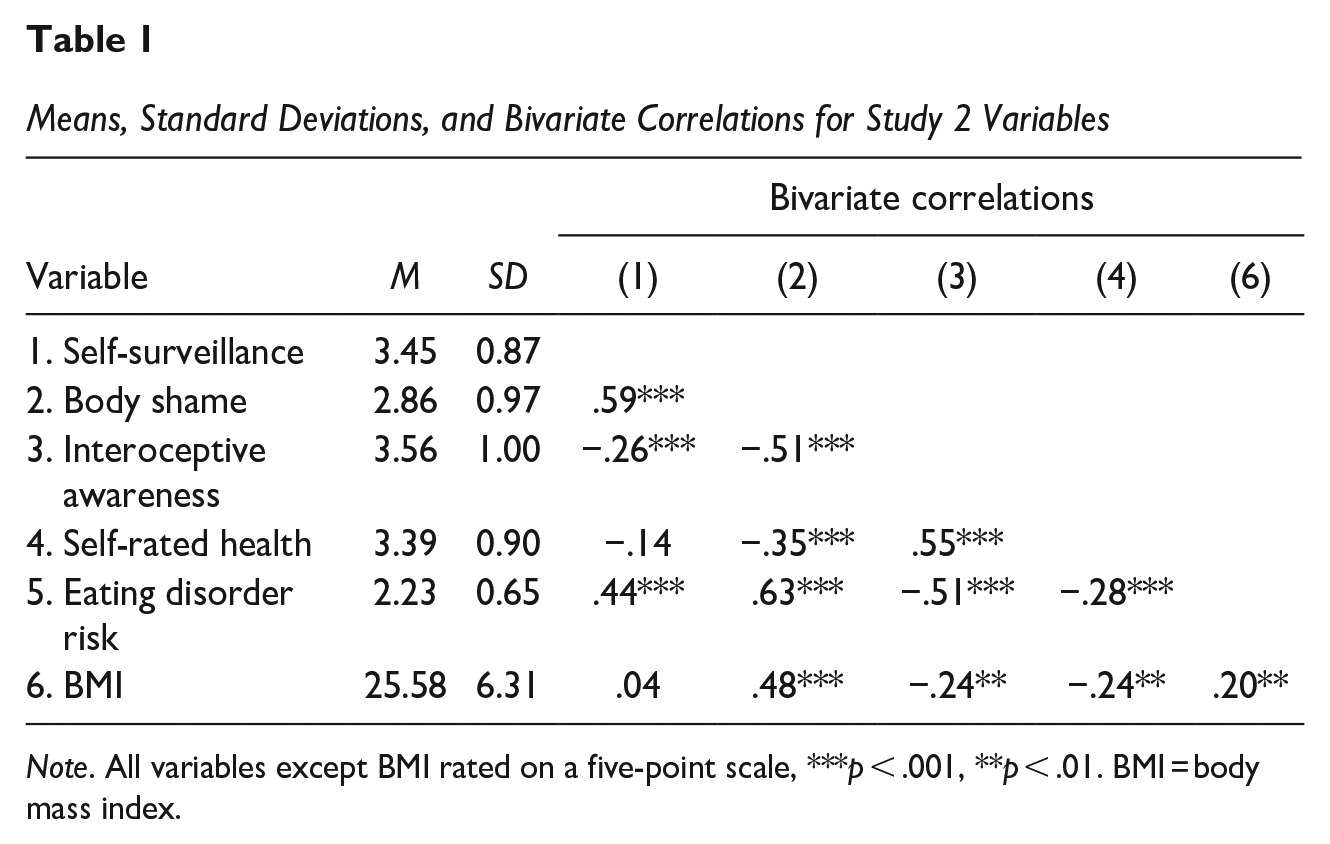
Note. All variables except BMI rated on a five-point scale, ***p < .001, **p < .01. BMI = body mass index.
To test the final hypothesis, a serial mediation model was run using the PROCESS macro for SPSS v4.0 (Hayes, 2022; model 6, 5,000 bootstraps, 95% bias-corrected confidence intervals). Self-surveillance was entered as the predictor, body shame as the first mediator, interoceptive awareness as the second mediator, and self-rated health as the outcome. BMI and eating disorder risk were entered as covariates. As expected (H1c), body shame and interoceptive awareness produced a significant indirect effect between self-surveillance and self-rated health, −0.08 (SE = 0.03), 99% CI [−0.15, −0.03]. Specifically, self-surveillance predicted high body shame, b = 0.46, p < .001, which in turn predicted low interoceptive awareness, b = −0.38, p < .01, which ultimately predicted low self-rated health. These results appear in Figure 1. Neither BMI, b = −0.01, p = .29, nor eating disorder risk, b = 0.06, p = .61, predicted self-rated health.
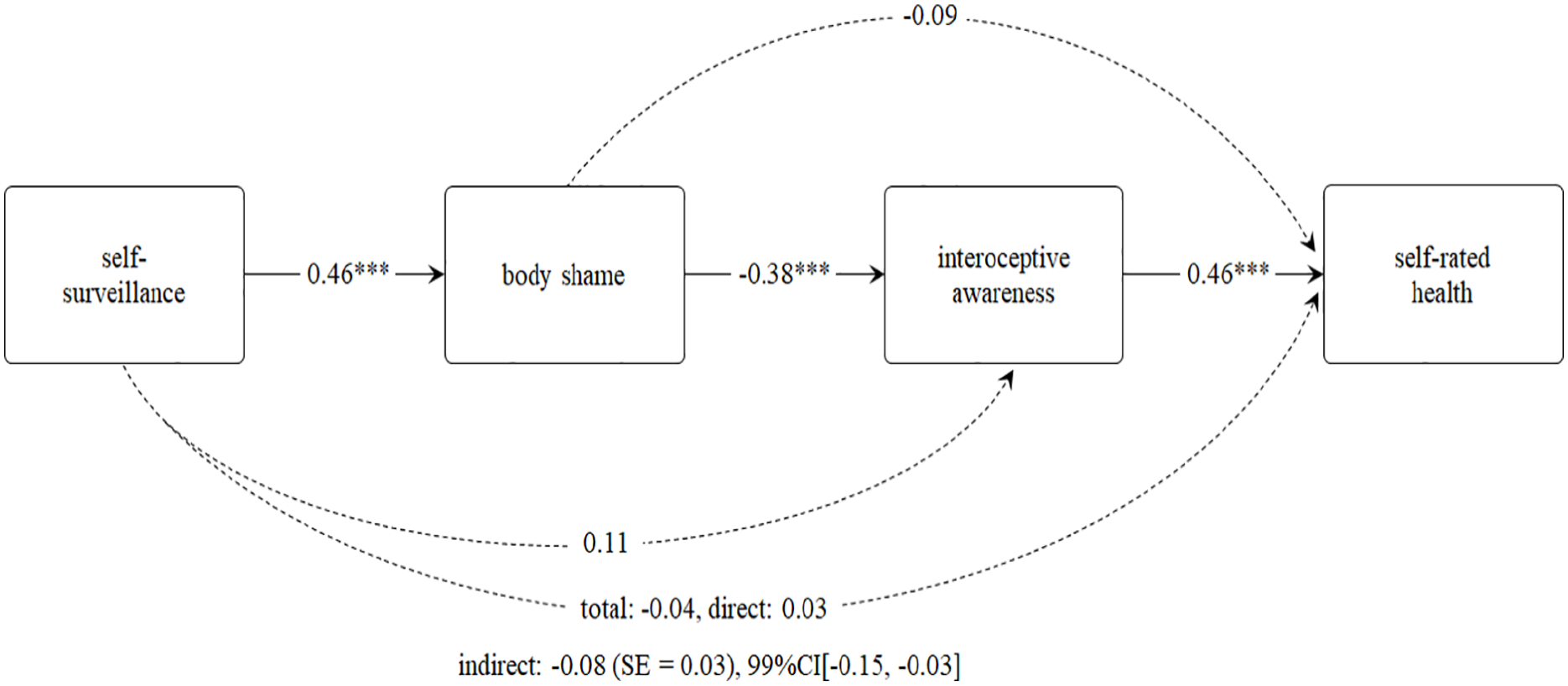
Serial Mediation of the Relationship Between Self-Surveillance and Self-Rated Health
Study 2
Study 1 demonstrated support for the proposed model in a sample of undergraduate women. Reflecting prior research, self-surveillance was unrelated to self-rated health. However, as expected, body shame and lower interoceptive awareness mediated these previously nonsignificant relationships. These results support the contention that self-surveillance may not be associated with self-rated health on its own but may do so through specific mechanisms. Finally, these results were not better explained by eating disorder risk or BMI, suggesting that this model may explain poor self-rated health in college women regardless of where one falls on the weight spectrum or whether one is at risk for an eating disorder.
As study 1 was the first to test the proposed model, study 2 was intended to replicate its results with some important changes. This time, awareness of internal bodily processes was defined as body responsiveness. Although interoceptive awareness is the ability to detect internal bodily states, body responsiveness is the ability to both detect and respond to those states. For example, as Daubenmier (2005) described, a yoga practitioner may both become aware of the sensation that a yoga pose is about to overstretch a muscle and respond to that information to optimize the pose without injury. Daubenmier (2005) found that the ability to respond to bodily sensations was associated with disordered eating attitudes beyond the mere ability to detect those sensations. Moreover, other studies have shown body responsiveness to be associated with self-rated health specifically (Lamont, 2015, 2019).
Second, the measure of self-rated health used in study 1 raises a concern. To be sure, this measure has been shown to be distinct from psychological health (Smith et al., 1999). Still, it is unclear what kind of health study 1 participants were reporting when they responded to the item, “in general, my health is. . ..” Some participants may have meant physical health, whereas others meant psychological health or some holistic combination thereof. In addition, although one element of psychological health (eating disorder risk) was controlled for, self-surveillance may co-occur with other types of psychological distress like sexual dysfunction and depression (Tiggemann & Williams, 2012). So, to ensure that this measure assessed physical self-rated health specifically, study 2 participants were asked explicitly to rate their “physical health.” Moreover, eating disorder risk was replaced with a general measure of psychological health. BMI was again included as a covariate.
Finally, study 1 tested the proposed model in women only. As a goal of the current project was to explain a gender difference in self-rated health, it was important to include men. Self-surveillance and its correlates are reliably stronger in women than in men (Lamont, 2021; McKinley, 2006). If self-surveillance, body shame, and low body responsiveness are associated with poor self-rated health, and women experience these to a greater extent than men, then these factors may help explain the gender difference in self-rated health. Therefore, study 2 employed a sample of undergraduate women and men.
The following hypotheses were made. Based on prior research showing inconsistent relationship between self-surveillance or self-objectification and self-rated health between female and male participants (Baceviciene et al., 2022; Rollero & De Piccoli, 2015), no hypotheses were made regarding the bivariate relationship between self-surveillance and self-rated physical health for women or men. Also reflecting prior research (Lamont, 2015, 2019; Rollero & De Piccoli, 2015) and study 1, self-rated health was expected to be (H2a) negatively correlated with body shame and (H2b) positively correlated with body responsiveness for women and men. Moreover, (H2c) women were expected to report lower self-rated health than men, as in prior research (Oksuzyan et al., 2009). Also based on prior work (Lamont, 2021; Rollero & De Piccoli, 2015), (H2d) women were expected to report greater self-surveillance and body shame as well as lower body responsiveness and self-rated physical health than men. Finally, it was expected that (H2e) self-surveillance and its sequelae would serially mediate the gender difference in self-rated health. That is, women were expected to have higher self-surveillance, which in turn would predict higher body shame, which would further predict lower body responsiveness, ultimately predicting lower self-rated physical health.
Method
Participants
Four-hundred fifty undergraduate students at a small liberal arts college completed the study and received course credit in return. Participants were not included in the study if they were not in a class in which course credit was offered in exchange for participation. Duplicate responses (n = 65), those participants indicating a gender identity not under investigation in the current study (e.g., nonbinary, n = 4), and those who failed an attention check (n = 25) were removed from analyses. Moreover, participants who did not complete at least one measure of a variable of interest (n = 7) were removed from analyses. This listwise deletion of cases with missing data was used because pairwise deletion would have resulted in different subsets of participants being included in the mediation analyses versus some of the bivariate correlations. Moreover, because of the tendency for imputation to restrict variability in scores (see Horton & Kleinman, 2007), that method was not used. This method left 347 participants in the final sample (age, M = 19.37, SD = 1.59). These participants self-identified as either women (n = 267) or men (n = 80) and as White (81.9%), Black or African-American (6.2%), mixed race or biracial (6.2%), Hispanic or Latina/o (2.8%), and Asian (2.3%), with 0.6% not reporting ethnicity.
Materials
Demographics
Gender, race and ethnicity, age, and BMI were measured and/or calculated using the same methods described in study 1.
Self-Surveillance and Body Shame
Self-surveillance and body shame were again measured using Objectified Body Consciousness Scale subscales (OBC; McKinley & Hyde, 1996) and again yielded good internal reliability, self-surveillance, α = .91, body shame, α = .87.
Body Responsiveness
Body responsiveness was measured using the Body Responsiveness Questionnaire (BRQ; Daubenmier, 2005). This scale contains seven items that assess one’s connection to the body (“My mind and my body often want to do different things” [r]) and the value of interoception (e.g., “I ‘listen’ to my body to advise me about what to do”). Participants responded to each item on a 1 (strongly disagree) through 5 (strongly agree) scale. After reverse-scoring (r) items, all items were combined to create a mean body responsiveness for each participant with higher scores meaning higher body responsiveness. This measure converges with like constructs reflecting internal awareness (i.e., body awareness, Daubenmier, 2005). This measure has demonstrated good internal reliability in previous studies (e.g., α = .76, Lamont, 2015; α = .81, Lamont, 2019) as well as in the current study, α = .79.
Self-Rated Physical Health
Self-rated physical health was measured using the standard single-item measure modified to read, “In general, my PHYSICAL health is. . .,” on a scale of 1 (poor), 2 (fair), 3 (good), 4 (very good), or 5 (excellent) (Vaez & Laflamme, 2003).
Self-Rated Psychological Health
Self-rated psychological health was measured using the standard single-item measure modified to read, “In general, my PSYCHOLOGICAL health is. . .,” on a scale of 1 (poor), 2 (fair), 3 (good), 4 (very good), or 5 (excellent). This valid measure of psychological well-being is distinct from self-rated physical health (Vaez & Laflamme, 2003).
Procedure
Study procedures were approved by the Bellarmine University Institutional Review Board. Participants were recruited over email for a study on personality characteristics and health. Due to the COVID-19 pandemic, data collection occurred online via two slightly different methods. In the first group, participants (n = 165) joined a Microsoft Teams meetings of up to 20 other participants. Cameras and microphones were muted for the study. A female research assistant described the study procedures and participants provided informed consent electronically. Then, participants received a link to the survey via the Microsoft Teams chat function and completed the research materials. For the second group (n = 182), the recruitment email contained a link to the same survey. After providing informed consent electronically, participants completed all research materials at their leisure within 2 weeks of receiving the email. Other variables (e.g., self-compassion) included as filler items are not reported herein.
Results
All data were analyzed using the SPSS Statistical Package v28.0. First, to test for possible differences between the two participant groups who completed the study in different ways, independent-samples t-tests were run (coding: first group = 1 and second group = 2). No differences emerged on self-surveillance, t(345) = −0.99, p = .32, body responsiveness, t(345) = 0.03, p = .97, self-rated physical health, t(345) = 0.41, p = .68, or BMI, t(345) = −1.11, p = .27. However, the participant groups did differ significantly on body shame, t(345) = −3.52, p < .01, group 1, M = 2.71, SD = 0.95, group 2, M = 3.07, SD = 0.95, and self-rated psychological health, t(345) = 2.05, p < .05, group 1, M = 2.79, SD = 1.03, group 2, M = 2.56, SD = 1.04,. Thus, although these two participant groups were collapsed across for analyses, participant group was controlled for in the mediation models.
To test the relationship between self-surveillance and self-rated health, as well as the first two hypotheses, bivariate correlations were run for women and men separately. As in Baceviciene et al. (2022) but contrary to Rollero and De Piccoli (2015), self-surveillance was negatively correlated with self-rated physical health for women, but unrelated for men. However, as expected for both women and men, (H2a) body shame correlated negatively with self-rated physical health, and (H2b) body responsiveness correlated positively with self-rated physical health. To test the next two hypotheses, bivariate correlations were run for the full sample (coding: 0 = women, 1 = men). As expected, (H2c) women had poorer self-rated health compared to men. Also as expected, (H2d) women had higher self-surveillance and body shame and lower body responsiveness compared to men. Correlations appear in Table 2.
Bivariate Correlations for Study 2 Variables
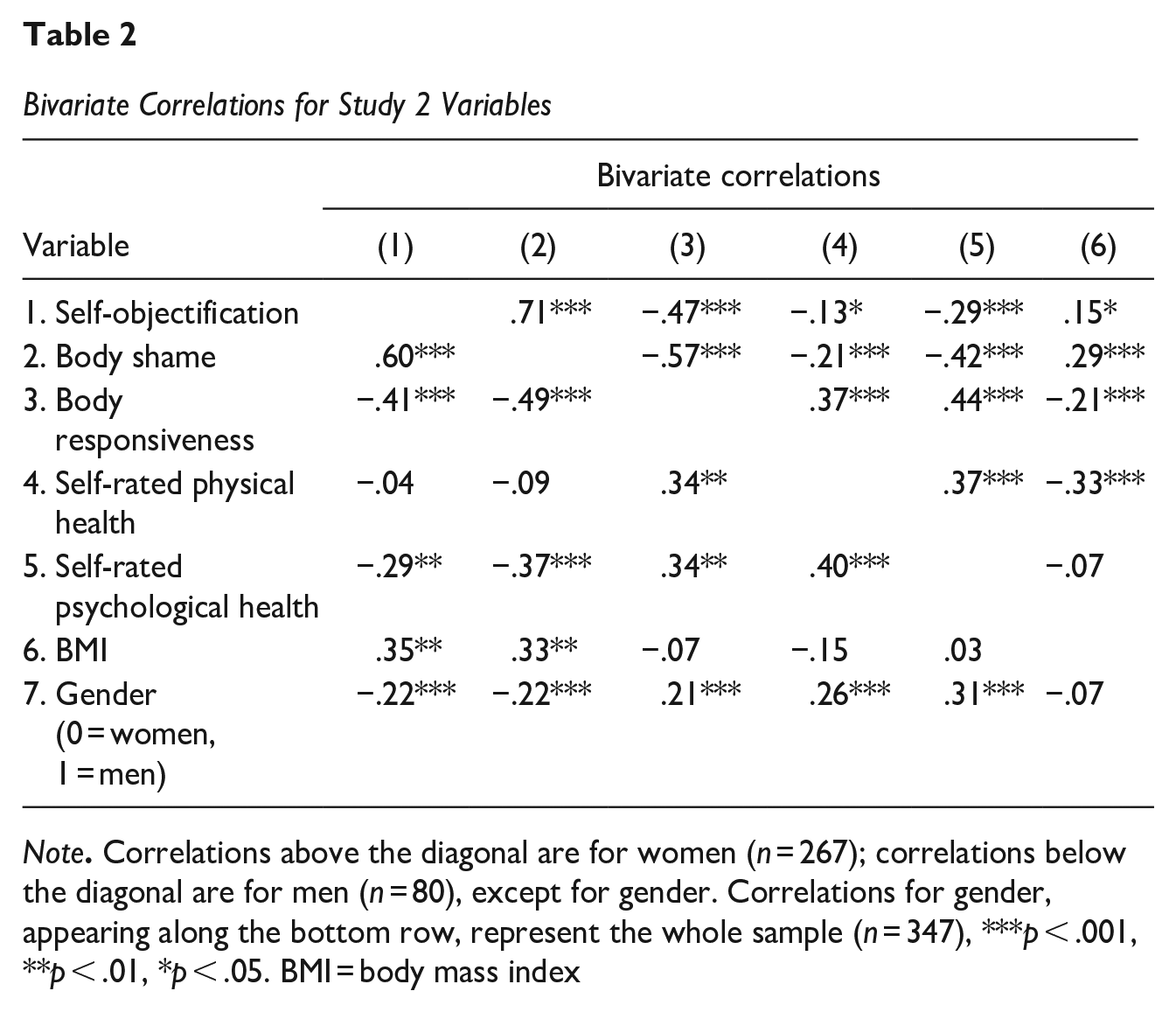
Note. Correlations above the diagonal are for women (n = 267); correlations below the diagonal are for men (n = 80), except for gender. Correlations for gender, appearing along the bottom row, represent the whole sample (n = 347), ***p < .001, **p < .01, *p < .05. BMI = body mass index
To test the final hypothesis, a serial mediation model was run using the PROCESS macro for SPSS v4.0 (Hayes, 2022; model 6, 5,000 bootstraps, 95% CI). Gender was entered as the predictor, self-surveillance as the first mediator, body shame as the second mediator, body responsiveness as the third mediator, and self-rated physical health as the outcome. BMI, self-rated psychological health, and participant group were entered as covariates. Supporting the final hypothesis, (H2e) self-surveillance, body shame, and body responsiveness produced a significant indirect effect between gender and self-rated physical health, −0.06 (SE = 0.02), 95% CI [−0.10, −0.03]. Specifically, women reported greater self-surveillance, which in turn predicted higher body shame, which in turn predicted lower body responsiveness, which ultimately predicted lower self-rated physical health. These results appear in Figure 2. Both BMI, b = −0.05, p < .001, and self-rated psychological health, b = 0.36, p < .001 predicted self-rated health in the full model. Participant group, however, did not predict self-rated physical health, b = 0.01, p = .93, suggesting that these results were not likely due to the different data collection methods.
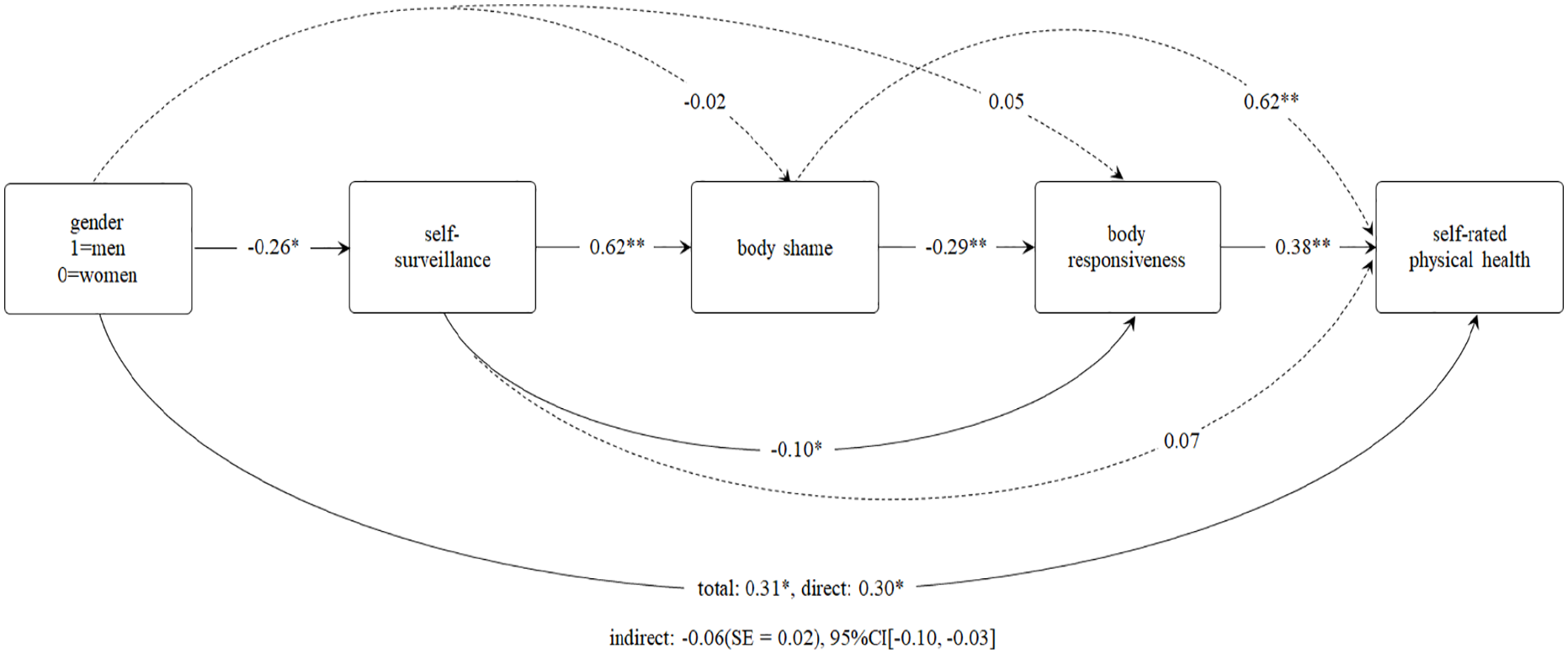
Serial Mediation of the Relationship Between Gender and Self-Rated Health
Discussion
The current investigation tested whether self-surveillance was associated with poor self-rated health via the mechanisms of body shame and diminished awareness of internal bodily functions and whether these factors explained the gender difference in self-rated health observed in prior research. In study 1, undergraduate women completed self-report measures of self-surveillance, body shame, interoceptive awareness, and self-rated health, as well as covariates (BMI and eating disorder symptoms). In study 2, undergraduate women and men completed self-report measures of self-surveillance, body shame, body responsiveness, and self-rated physical health, as well as covariates (BMI and self-rated psychological health). The results support the three keys findings that align with the aims of the current investigation.
First, the current investigation confirmed the suspected inconsistency in the bivariate relationship between self-surveillance and self-rated health shown in prior literature (Baceviciene et al., 2022; Rollero & De Piccoli, 2015; Sveinsdóttir, 2017). In study 1, self-surveillance was unrelated to self-rated health in the sample of all female undergraduate participants and negatively correlated with self-rated health for female undergraduate participants in study 2. To be sure, it is possible that this inconsistent bivariate relationship across the two current samples was simply the result of Type 1 error. Indeed, the correlation between these two variables for female participants in study 2 would not be significant at a more conservative alpha (e.g., p < .01). However, such an inconsistent relationship supports the contention that self-surveillance may be associated with both good and bad health. This explanation aligns with the similar inconsistencies observed between self-surveillance and health behaviors, which are both harmful and beneficial (Ertl et al., 2022; Slater & Tiggemann, 2002). Therefore, continued studies are needed to clarify the nature of this relationship.
Second, the current investigation illuminates the importance of examining mechanisms in the relationship between self-surveillance and self-rated physical health, at least in a college population. In both studies, regardless of whether it was significant, the bivariate relationship between self-surveillance and self-rated physical health in these samples was consistently explained by body shame and diminished awareness of internal bodily states. Moreover, the order of these mediators is supported by other studies demonstrating that body shame and lowered internal awareness serially mediated the relationship between self-surveillance and health behaviors (Holmes & Johnson, 2017). Crucially, this investigation provides a preliminary extension of that model to self-rated physical health in college students. That is, self-surveillance, to the extent that it is associated with body shame and diminished internal awareness, may indeed impact physical self-rated health, at least in the college samples in the current studies. Given that these results emerged in an undergraduate population, it is reasonable to wonder whether these effects would be specific to or at least pronounced in a college population. The negative effects of self-surveillance have been shown reliably in college samples. A meta-analysis by Schaefer and Thompson (2018) found that these associations are similar in strength to those found in younger adolescents, but decrease as adulthood progresses. Therefore, future research may examine this model in age-diverse samples.
Third, the current investigation supports the idea that objectification theory may help to explain the persistent difference in self-rated health between female and male college students (Chen & Lucock, 2022; Vaez & Laflamme, 2003). Indeed, in study 2, undergraduate men self-reported better self-rated health compared to undergraduate women, and this gender difference was explained by factors identified by objectification theory (Fredrickson & Roberts, 1997). Specifically, undergraduate women were more likely to report self-surveillance and body shame, as well as low body responsiveness, all of which were related to these participants’ lower self-rated physical health. Moreover, this result was not explained by the gender difference in self-rated psychological health. Such a result may suggest that the relationships of self-surveillance and its sequelae to self-rated physical health in the current samples are not explained by self-surveillance’s well-established association with undergraduate women’s psychological health (Tiggemann & Williams, 2012). To be sure, the null bivariate relationship between self-surveillance and self-rated health in male participants may have arisen from Type II error, owing to the small number of men in the sample. However, this same result was also found in the large sample recruited by Baceviciene et al. (2022). Moreover, although the relationship between self-surveillance and body shame emerged for men as it has in other research (McKinley, 2011; Tiggemann & Kuring, 2004); nonetheless, the relationships of these variables to self-rated health may be too weak to detect in such a small sample, and future research should test this model using larger samples. Moreover, future research should test whether this model also explains the gender difference in self-rated health found in younger adolescents (Jerdén et al., 2011; Yoo & Jang, 2023) and middle-aged to older adults (McCullough, & Laurenceau, 2004; Rani et al., 2022).
Limitations
In addition to the limitations mentioned above, the results of the current project should be interpreted with the following caveats in mind. The sample in the current investigation consisted of young, mostly White undergraduates at a liberal arts institution. Some investigations have found that liberal arts college students report engaging in more beneficial health behaviors (Baldwin et al., 2017; Salameh et al., 2014), which may suggest that the current samples were healthier than college students at larger, public universities. Furthermore, although self-surveillance and its sequelae occur across race and ethnicity, sexuality, and age (Moradi & Huang, 2008), the associations of these factors with self-rated health may vary among these groups. Indeed, race and ethnicity, sexuality, and age have been associated with poor physical health (United States Center for Disease Control, 2013). For example, although both Black and White women experience self-surveillance (Moradi & Huang, 2008), Black women experience worse health than White women (Cummings & Braboy Jackson, 2008). This health disparity may occur because Black women also experience racial discrimination and a profound lack of access to healthcare (United States Center for Disease Control, 2013). Moreover, transgender and nonbinary people experience self-surveillance (Strübel et al., 2020) as well as the persistent denial of gender-affirming healthcare (Padula & Baker, 2017). These factors could eclipse the impact of self-surveillance and its sequelae on self-rated health in groups with intersecting marginalized identities. Recruiting from certain college populations may systematically exclude marginalized identities (Henry et al., 2011), such as was the case with the current investigation. Therefore, intentional recruitment of individuals from marginalized groups in order to test this model is recommended.
Another limitation relates to the differences between the two groups of participants in study 2. For this study, two datasets were combined to test hypotheses, one collected in person prior to the COVID-19 pandemic (group 1) and the other collected online during social distancing practices common in the COVID-19 pandemic (group 2). Collapsing across these samples, of course, increased sample size, thus providing a more powerful test of the hypothesized model. Moreover, for the most part, these groups did not differ on the variables of interest. However, the groups did differ such that the mid-pandemic group reported significantly more body shame and poorer self-rated psychological health than the pre-pandemic group. This result tracks with research demonstrating negative changes in body image (Schneider et al., 2023) and psychological health (Buizza et al., 2022) over the course of the pandemic, as well as research linking body shame and poor psychological health (Tiggemann & Williams, 2012). Regardless, the models held when controlling for participants group, suggesting that these differences between the groups did not contribute to the associations demonstrated in the model in study 2.
Finally, perhaps the most important limitation of the current investigation concerns the cross-sectional nature of the data. Serial mediation models conducted on cross-sectional data may inflate effects (Maxwell & Cole, 2007). Moreover, as it is collected at a single time point, cross-sectional data cannot provide evidence of the temporal precedence of any of the relationships within the model. Therefore, causation among the links in the model should not be inferred from the results of the present investigation alone. Nonetheless, several features of the current investigation’s model encourage confidence in its validity and its potential to inspire future work. First, the model in the current investigation is based on a well-supported model demonstrating that the serial combination of self-surveillance, followed by body shame, followed by poor internal awareness is associated with poor health behaviors (Augustus-Horvath & Tylka, 2009; Holmes & Johnson, 2017; Tylka & Hill, 2004; Watson et al., 2013). Second, the extension of this model to self-rated health in the current investigation replicated across the two studies herein. Third, prior research supports the directionality of individual links within the model. For example, experimental increases in self-surveillance-related states like self-objectification is associated with subsequent increases in body shame (Dimas et al., 2021; Fredrickson et al., 1998; Hebl et al., 2004), and experimentally induced body shame is associated with subsequent decreases in body responsiveness (Lamont, 2021). Furthermore, longitudinal and experimental evidence suggests that low internal awareness is associated with future decreases in physical health outcomes (Courtois et al., 2015; Lamont, 2015; Landsman-Dijkstra et al., 2004; Zucker et al. 2017). Nevertheless, the current model would benefit from future tests, particularly those using longitudinal analysis to examine the development of these variables over time. The results of the current investigation provide a crucial foundation for such work.
Implications and Future Directions
The findings of the current investigation support a novel explanation for the gender difference in self-rated health between women and men, at least in college women at a liberal arts university. Moreover, they suggest that the associations among self-surveillance, body shame, and low internal awareness of objectifying culture as outlined in objectification theory (Fredrickson & Roberts, 1997) may be more insidious than previously thought, extending past psychological health and health behaviors into the realm of physical health outcomes. To be sure, many factors may be expected to converge to determine an individual’s self-rated health, including biological, social, and psychological factors. Moreover, the power of any one factor to influence self-rated health likely varies in strength. Indeed, any effects of self-surveillance and its sequelae on self-rated health may be small. Nevertheless, even small effects in health promotion and prevention research have been shown to have large real-world implications (National Institutes of Health, n.d.). Thus, identifying a path via which self-surveillance may be associated with self-rated health may inform health promotion as well as the prevention of poor health behaviors and outcomes, particularly for women.
Importantly, the results of the current investigation suggest that whether self-surveillance is associated with self-rated health may depend on the mechanism examined. Indeed, self-surveillance may at times promote good self-rated physical health. According to Courtney and Goldenberg (2021), thinking about the corporeality of one’s own body evokes anxiety about death, paradoxically producing avoidance of health behaviors that involve examining the body (e.g., cancer screenings). Prioritizing the appearance of the body and ignoring its function may be a way of reducing the corporeality of the body, thus attenuating that anxiety and avoidance and promoting beneficial health behaviors and potentially positive health outcomes. Future research may examine the potentially positive effects of self-surveillance on self-rated health and other physical health outcomes.
Nevertheless, the current research, along with prior research, suggests body shame and low internal awareness as mechanisms by which self-surveillance may be associated with poor self-rated health. From a health promotion standpoint, this body of research identifies two points of attack in improving self-rated health: reducing body shame and improving internal awareness. Mindfulness-related interventions have promise in reducing body shame (Albertson et al., 2015) and/or improving internal awareness (Fischer et al., 2017). Moreover, such interventions have also been shown to be effective at preventing poor health behaviors (Roche et al., 2019) and promoting positive health outcomes (Creswell et al., 2019). Future research may test whether these interventions may interrupt the potential impact of self-surveillance on self-rated health by reducing body shame and improving internal awareness. Such studies may provide health practitioners with tools to promote health and to prevent poor health outcomes in patients.
Moreover, as the link between self-surveillance and poor health is likely complex, other mechanisms that promote poor self-rated health may be at play. Indeed, some of the poor health behaviors associated with self-surveillance may also tie these factors to poor self-rated health. Moreover, biological changes elicited by self-surveillance may also be associated with poor self-rated health. Experimental body image threat inductions have been shown to provoke acute cortisol production (Cloudt et al., 2014; Lamarche et al., 2014). Although this research has not measured self-surveillance specifically, the body image threat is similar to methods used to evoke self-surveillance-like states, in which participants model revealing clothing in front of a mirror (Fredrickson et al., 1998) or imagine doing so (Tiggemann & Andrew, 2012). Chronic exposure to situations that evoke acute cortisol responding may produce cortisol dysregulation or habitual malfunctioning of the cortisol response. As cortisol dysregulation may produce disease state (Sorrells et al., 2009), self-surveillance may be linked to self-rated health and other physical health outcomes via cortisol dysregulation. Future research may examine additional mechanisms by which self-surveillance may be associated with poor self-rated health.
In addition to mediating variables, the inconsistent bivariate relationship between self-objectification and self-rated health across the literature could also be explained by moderating variables. That is, instead of self-surveillance conceptually setting off processes which in turn may impact health, certain factors may create conditions under which the link between self-surveillance and self-rated health is exacerbated or attenuated. For example, a history of abuse in childhood has been associated with both self-surveillance (Holmes & Johnson, 2017) and poorer self-rated health (Felitti et al., 2019). Therefore, for individuals who have experienced childhood abuse, the relationship between self-surveillance and self-rated health may be intensified. On the other hand, social support, a well-known correlate of physical health (Uchino, 2006), has been associated with resilience to the negative effects of objectified body ideals (Jiao et al., 2022; Stice et al., 2001). Thus, it is possible that having a strong social support network may weaken the association between self-surveillance and self-rated health. Future research may also examine these and other potential moderators of this relationship.
Finally, although self-rated health is an important indicator of physical health in and of itself (Idler & Benyamini, 1997), future research may extend this model to examine objective measures of health as well. For example, in addition to poorer self-rated health, women also report more functional disability (van Oyen et al., 2013) and greater chronic disease morbidity (Case & Paxson, 2005) over their lifespans than do men. Furthermore, body shame has been shown to be associated with physical symptoms and increased infections via the mechanism of low body responsiveness (Lamont, 2015, 2019). If self-surveillance, by way of body shame and lower internal awareness, is associated with poor self-rated health, then these body image-related factors may be linked to objective measures of physical health as well. Future research may examine the current model with a variety of physical health-related outcomes.
Footnotes
Acknowledgements
The author expresses sincere gratitude to Abby Flynn and Lauren Dienes for their assistance with data collection on this project.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures performed herein were approved by the Bellarmine University Institutional Review Board.
Data Availability
Data associated with this study are available upon reasonable request from the author.