
Abstract
This study quantitatively assessed adults’ mental health and overall wellbeing over time during the first 16 months of the pandemic in Ontario, Canada. A total of 2,188 participants participated in the study and completed online questionnaires at three time points (baseline—April–July 2020; time 2—July–August 2020; and time 3—July–August 2021), which included demographic questions, the Mental Health Inventory (MHI), and the Personal Wellbeing Index-Adult (PWI-A). One-way repeated-measures ANOVAs revealed a statistically significant increase over time in participants’ mental health (MHI), as well as a significant decrease in their satisfaction with their standard of living, physical health, mental health, personal relationships, safety, community-connectedness, future security, and spirituality/religion (PWI-A). While participants’ mental health improved, their mean scores indicated the presence of mental health disorders. Generally speaking, over the first 16 months of the pandemic, the self-reported mental health of Ontario adults improved, while their perceived wellbeing declined.
Introduction
The COVID-19 pandemic has created individual and systemic issues that have challenged the mental health of citizens (Fitzpatrick et al., 2020). At an individual level, the pandemic has caused insecurity, confusion, emotional isolation, and stigma, whereas communities have suffered from economic loss, challenges related to work and school closures, and inadequate resources for testing, treatment, and protection (Pfefferbaum & North, 2020). Such challenges may lead to distress or psychiatric conditions, as well as unhealthy behaviors (Pfefferbaum & North, 2020). In response to the COVID-19 pandemic, the Ontario provincial government mandated various protections to mitigate the spread of the virus (Government of Ontario, 2022), which have been acknowledged as disrupting everyday activities and routines of citizens (Di Sebastiano et al., 2020). Such disruptions have been implicated in the pandemic’s impact on people’s mental health and wellbeing (Khan et al., 2020; Meyer et al., 2020). In addition to the range of health consequences from contracting COVID-19, researchers have also attributed individuals’ mental health challenges to pandemic-related financial strain and unemployment, housing and food insecurity, lack of childcare, and disproportionate and gendered caregiving (Canadian Human Rights Commission, 2020; Van Lancker & Parolin, 2020). The mental health consequences of the COVID-19 pandemic are being recognized as a growing “wave” (Babaian, 2020; Tseng, 2020), with the number of people impacted expected to increase over time (Douglas et al., 2020; Haynes et al., 2020).
In Canada, there is growing concern for the mental health and wellbeing of individuals (Angus Reid Institute, 2020; Capaldi et al., 2021; Jenkins et al., 2021). Specifically, during the early stages of the pandemic (April 2020), 50% of Canadian adults (aged 18+) reported that their mental health had declined, and over 40% of them described being worried and/or anxious because of the pandemic (Angus Reid Institute, 2020). Jenkins et al. (2021) conducted a cross-sectional online survey study in May 2020 to investigate the impact of the pandemic on the mental health of adults in Canada (Mage = 49.1 years; N = 3,000). The authors found that 38.2% of participants reported a deterioration in their mental health since the onset of the COVID-19 pandemic, and those with pre-existing mental health conditions were significantly more vulnerable (Jenkins et al., 2021). Women were significantly more likely to report a deterioration of their mental health than men (44% compared to 32%, respectively; Jenkins et al., 2021). Moreover, respondents noted experiencing anxiety/worry (46%), stress (37%), loneliness/isolation (30%), depression (23%), as well as feelings of loneliness/isolation (27%), and sadness (23%; Jenkins et al., 2021). Contributing to their poor mental health were several pandemic-related stresses, including loved ones getting sick, financial strain, and job loss (Jenkins et al., 2021). While some participants indicated that they were not coping well, others employed various strategies, including exercise (59%), connecting with loved ones (56%), and maintaining a healthy lifestyle (43%; Jenkins et al., 2021). Additionally, Capaldi et al. (2021) used cross-sectional data from January 2 to December 24, 2019 (pre-pandemic; N = 57,034) and from September 11 to December 4, 2020 (during the pandemic; N = 11,324) to compare Canadian adults’ (18+ years) mental health, community belonging, and life satisfaction. Despite the fact that over half of the participants reported positive mental health, the authors found that, compared to pre-pandemic, significantly fewer participants reported high levels of positive mental health during the early pandemic (60% in 2020 compared to 67% in 2019; Capaldi et al., 2021). In 2020, 64% of participants reported feeling high levels of community belonging, which was significantly lower than what was reported in 2019 (68.4%; Capaldi et al., 2021). Moreover, on a scale from 0 to 10, the average life satisfaction of Canadian adults was 7.19 in 2020, which was significantly lower than that reported in 2019 (M = 8.08; Capaldi et al., 2021). When the authors categorized their data by province, it was clear that the findings from Ontario were consistent with those at the national level, such that there were statistically significant differences in participants’ mental health, community belonging, and life satisfaction between 2019 and 2020, with fewer participants reporting favorable health characteristics (Capaldi et al., 2021).
The deterioration of mental health and wellbeing of adults living in Canada during the pandemic is not an isolated phenomenon, as international researchers have reported similar findings globally (e.g., O’Connor et al., 2021; White & Van Der Boor, 2020; Xiong et al., 2020). Specifically, O’Connor et al. (2021) investigated the mental health and wellbeing of adults (N = 3,077; 18+ years) during the first 6 weeks of lockdown in the United Kingdom (UK; March 31–May 11, 2020). The authors surveyed participants and concluded that rates of suicidal ideation increased during the initial weeks of the lockdown, and one in four participants reported experiencing moderate to severe levels of depression (O’Connor et al., 2021). Similarly, White and Van Der Boor (2020) assessed the mental health and wellbeing of 600 adults (M age = 36.75) in the United Kingdom during the initial lockdown (March 31–April 13, 2020) and found that participants who self-isolated prior to the lockdown due to COVID-19 symptoms, as well as those who felt more isolated in general, experienced poor mental health compared to those who did not isolate (White & Van Der Boor, 2020). Specifically, participants reported significantly higher levels of anxiety and depression, as well as lower levels of wellbeing and quality of life than those who did not self-isolate (White & Van Der Boor, 2020). Moreover, Xiong et al. (2020) conducted a systematic review (N = 19 studies) to explore the impact of COVID-19 on the psychological outcomes of individuals. The authors concluded that individuals in various countries (i.e., China, Spain, Italy, Iran, the United States, Turkey, Nepal, and Denmark) reported concerning rates of depression (14.6%–48.3%), post-traumatic stress disorder (7%–53.8%), anxiety (6.33%–50.9%), psychological distress (34.43%–38%), and stress (8.1%–81.9%) during the COVID-19 pandemic (Xiong et al., 2020).
It is evident, based on the data presented, that the COVID-19 pandemic has impacted the mental health and wellbeing of people around the world, including adults in Canada during the early waves of the pandemic; however, no data have been reported on changes in Ontario adults’ mental health at different time points during the pandemic. The aforementioned studies lacked the ability to detect changes in characteristics over time. As such, the current study fills this gap, given its longitudinal nature and the fact that the timeframe spans the first 16 months of the pandemic in Ontario, Canada. Moreover, it is important to investigate the mental health and wellbeing of adults at a provincial level as public health protection mandates are provincially determined. As previously indicated, the COVID-19 pandemic has the potential to create a secondary crisis—one of psychological distress and “mental health system spillover” (Choi et al., 2020, p. 340). Given the mental health concerns reported to date, it is plausible that more individuals with poor mental health will need support than previously (pre-pandemic), thus creating a system “spillover” and, in turn, placing additional strain on the mental health system (Choi et al., 2020). Being able to anticipate the extent in which spillover might occur and overwhelm existing access to mental health services and resources can help to buffer against the short- and long-term harm to adults’ mental health and aid in understanding the resource investments that need to be prioritized in order to support citizens during uncertain times (Choi et al., 2020). To this end, the purpose of this article was to quantitatively assess adults’ mental health and overall wellbeing over time during the first 16 months of the pandemic in Ontario, Canada.
Methods
Study Design
This article is a part of a longitudinal survey-based study titled Health Outcomes for adults during and following the COVID-19 PandEmic (HOPE), which aims to quantitatively assess the impact of the COVID-19 pandemic on several lifestyle-related health behaviors, including physical activity, sedentary behavior, sleep, dietary intake, prosocial behavior, mental health, and wellbeing. The current article reports on participants’ mental health and wellbeing using data collected from April 24, 2020 to August 30, 2021. A more fulsome description of the methods (i.e., study design, study procedures, recruitment, measures, data analysis) for this research have been detailed elsewhere (Shillington et al., 2021, 2022a, 2022b).
Participants
Participants were recruited for the larger study via social media platforms and through community health centers, regional health units, and medical clinics. To be eligible for the study participants needed to be: (a) an Ontario resident, (b) between the ages of 30 and 59 years at baseline, as individuals within this age range are most at-risk for development of chronic conditions (World Health Organization, 2005), and (c) able to read and write in English.
Study Procedures
Data collection occurred at three time points: (a) baseline/time 1 (T1; April 24–July 13, 2020); (b) time 2 (T2; July 29–August 30, 2020); and time 3 (T3; July 29–August 30, 2021). Recruitment and T1 data collection occurred simultaneously; upon clicking the link in the study advertisement, interested Ontario adults were directed to an online survey, via Qualtrics, which included the letter of information, eligibility questions, consent, and the T1 questionnaires (inclusive of demographics, the Mental Health Inventory-5 [MHI-5; Berwick et al., 1991], and the Personal Wellbeing Index-Adult [PWI-A; International Wellbeing Group, 2013]). At subsequent time points, the same questionnaires were administered, with the exception of the demographic items. Most demographic questions were only asked at T1; however, some demographic questions were asked at each time point, as outlined in section “Measures.”
Measures
While The HOPE Study includes several measures, for the purpose of this article, only demographic questions and the mental health and wellbeing measures were included and are presented below. For full measure details, see Shillington et al. (2021).
Demographics
The T1 demographic questionnaire included questions pertaining to participants’ age, sex, gender, ethnicity, geographic location, employment status, income, education attainment, marital status, COVID-19 diagnosis (at any time point), and presence of mental health conditions (mental illness, mood/anxiety disorders, and schizophrenia; consistent with Statistics Canada’s prevalence of chronic diseases among Canadian adults; Government of Canada, 2019). The T2 and T3 demographics questionnaires included questions pertaining to the extent to which participants’ incomes may have changed over the pandemic, employment status, COVID-19 diagnosis (at any time point), and presence of mental health conditions.
Mental Health Inventory-5
The MHI-5 (Berwick et al., 1991) was previously validated and is used to measure mental health status using five items that focus on positive affect (n = 2), anxiety (n = 1), depression (n = 1), and behavioral/emotional control (n = 1), respectively. Participants were asked the extent to which each statement was true on a Likert scale of 1 (all of the time) to 6 (none of the time). Higher scores indicated better mental health. The MHI-5 does not have a pre-determined cut-score; however, researchers have suggested that scores 76 or below is indictive of a mental disorder (Kelly et al., 2008). As such, this cut score will be used to interpret findings in the current study.
Personal Wellbeing Index-Adult
The PWI-A (International Wellbeing Group, 2013) was previously validated and measures subjective wellbeing using seven items that correspond to quality of life domains including: (a) standard of living, (b) health 1 , (c) achievement in life, (d) relationships, (e) safety, (f) community-connectedness, and (g) future security. It also includes two additional (optional) items: (a) satisfaction with life as a whole and (b) spirituality/religion. Participants were asked to indicate how satisfied they felt in each of the domains, as well as the additional items, on a Likert scale of 0 (no satisfaction at all) to 10 (completely satisfied), whereby higher scores indicated better wellbeing.
Data Analysis
A series of one-way repeated measures ANOVAs were conducted in SPSS to determine whether statistically significant differences existed in participants’ mental health (one item) and wellbeing (nine items), respectively, throughout the COVID-19 pandemic (T1–T3). To correct for multiple comparison bias in post hoc analyses, a Bonferroni correction was applied. Multiple imputation was used to handle missing data and maintain sample size. Thus, all participants (N = 2,188) were included in the analyses, and all data analyses were completed in IBM SPSS (version 28.0.1.1).
Results
Demographics
A total of 2,188 participants (Mage = 43.15 years; SD = 8.82) participated in The HOPE Study. Most participants identified as female (n = 1,743; 89.55%) and were of European origins (n = 1,789; 91.55%). At T1, 1,162 (59.22%) participants were employed full-time, 1,220 (62.18%) participants had an annual household income of $80,000 or greater, and 32 (1.63%) participants identified as having had COVID-19. Most participants in the study were married, common law, or engaged (n = 1,535; 78.20%) and had a university undergraduate degree or higher (n = 1,123; 57.21%). At T1, 6.85% (n = 150) of participants identified as having a mental illness, and 24.04% (n = 526) of them reported having mood/anxiety disorders. The prevalence of participants reporting mental illness at T2 and T3 was 3.24% (n = 71) and 3.56% (n = 78), respectively. The prevalence of mood/anxiety disorders at T2 was 11.06% (n = 242), and at T3, it was 9.60% (n = 210). No participants reported having schizophrenia at any time point. Moreover, when asked the extent to which their income had changed since T1 at T2, 78.38% (n = 678) of participants reported that their income had stayed the same, whereas at T3, 54.80% (n = 428) of them reported that it stayed the same. At T2, 16 participants (1.86%) had tested positive or suspected themselves to have COVID-19, whereas at T3, this number rose to 25 (3.20%). Moreover, at T2, 503 participants were employed full-time (58.15%), whereas at T3, 62.61% (n = 489) of them were employed full-time. For full demographic details, see Shillington, Yates et al. (2023).
Mental Health
A one-way repeated measures ANOVA revealed a statistically significant difference in participants’ mental health over time, F(1.95,4,275.02) = 34.22, p ≤ .001, η2p = .015. Post hoc tests revealed a statistically significant increase in participants’ mental health scores from T1 to T2 (Mdifference = −2.42, p ≤ .001, 95% confident interval (CI) = −3.37 to −1.46) and from T1 to T3 (Mdifference = −3.44, p ≤ .001, 95% CI = −4.45 to −2.42). The mean scores for participants’ mental health at each time point were 60.21, 62.63, and 63.65, respectively, indicating presence of a mental disorder, see Table 1.
The Mental Health and Wellbeing of Ontario Adults During the First 16 Months of the COVID-19 Pandemic in Ontario, Canada
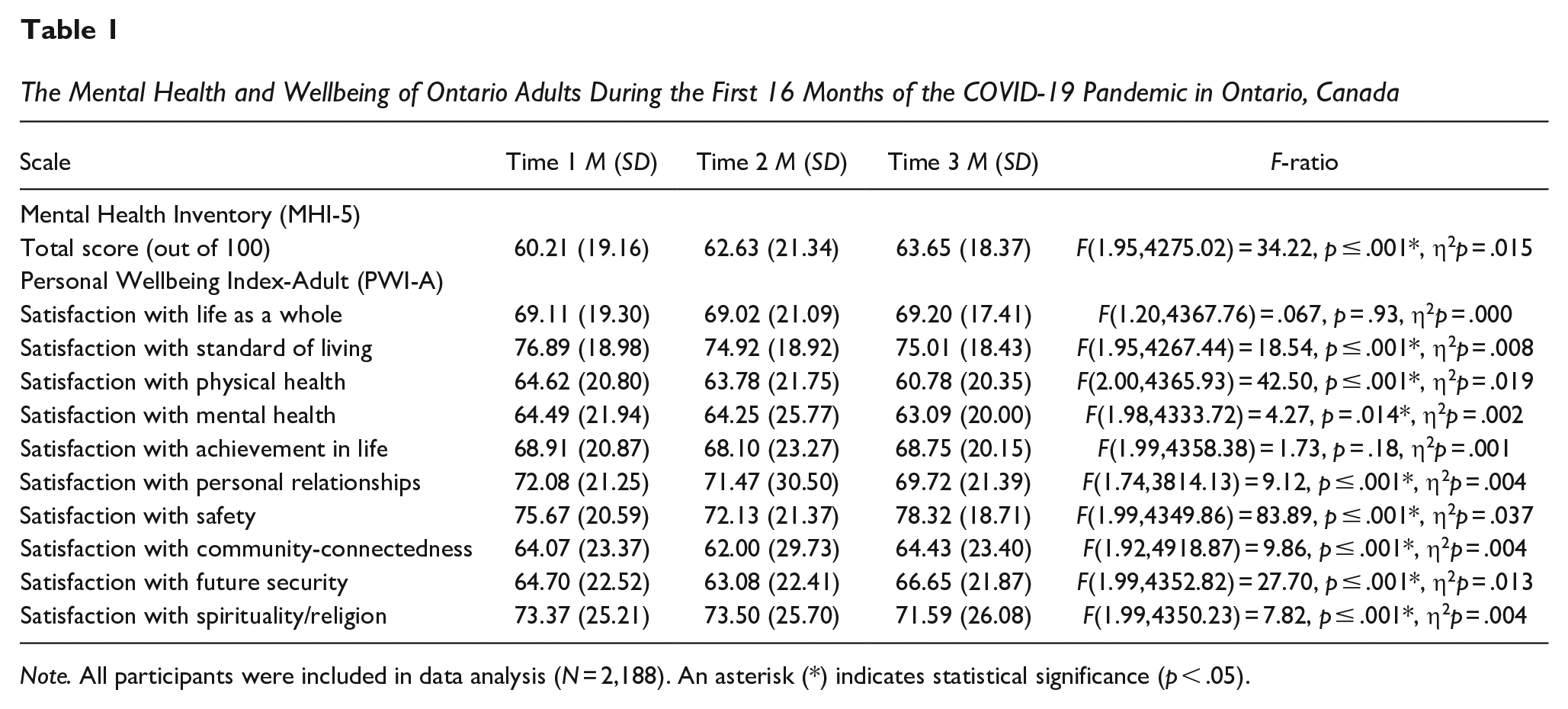
Note. All participants were included in data analysis (N = 2,188). An asterisk (*) indicates statistical significance (p < .05).
Wellbeing
There was no significant difference in participants’ satisfaction with their life as a whole, F(1.20,4367.76) = 0.067, p = .93, η2p = .000. There was a statistically significant difference in participants’ satisfaction with their standard of living over time, F(1.95,4267.44) = 18.54, p ≤ .001, η2p = .008. Post hoc testing revealed that participants’ satisfaction with their standard of living significantly decreased from T1 to T2 (Mdifference = 1.97, p ≤ .001, 95% CI = 1.13, 2.81) and from T1 to T3 (Mdifference = 1.88, p ≤ .001, 95% CI = 0.94, 2.82). A statistically significant difference was also found for participants’ satisfaction with their physical health over time F(2.00,4365.93) = 42.50, p ≤ .001, η2p = .019. Post hoc analyses revealed that participants’ satisfaction with their physical health decreased significantly from T1 to T3 (Mdifference = 3.84, p < .001, 95% CI = 2.77, 4.90) and from T2 to T3 (Mdifference = 3.00, p ≤ .001, 95% CI = 1.94, 4.05). There was also a significant difference in participants’ satisfaction with their mental health over time, F(1.98,4333.72) = 4.27, p = .014, η2p = .002, with post hoc tests showing that scores decreased significantly from T1 to T3 (Mdifference = 1.40, p ≤ .001, 95% CI = 0.23, 2.57). No statistically significant difference was found for participants’ satisfaction with their achievement in life, F(1.99,4358.38) = 1.73, p = .18, η2p = .001. There was a significant difference found for participants’ satisfaction with their personal relationships over time, F(1.74,3814.13) = 9.12, p ≤ .001, η2p = .004. Post hoc analysis revealed that participants’ satisfaction with their personal relationships decreased significantly from T1 to T3 (Mdifference = 2.35, p ≤ .001, 95% CI = 1.27, 3.44) and from T2 to T3 (Mdifference = 1.75, p = .019, 95% CI = 0.22, 3.28).
There was a statistically significant difference in participants’ satisfaction with their safety over time, F(1.99,4349.86) = 83.89, p ≤ .001, η2p = .037, with post hoc analysis showing that scores decreased from T1 to T2 (Mdifference = 3.54, p ≤ .001, 95% CI = 2.44, 4.65) and increased from T1 to T3 (Mdifference = −2.64, p ≤ .001, 95% CI = −3.82 to −1.47) and T2 to T3 (Mdifference = −6.19, p ≤ .001, 95% CI = −7.36 to −5.01). There was a statistically significant difference in participants’ satisfaction with their community-connectedness over time, F(1.92,4,918.87) = 9.86, p ≤ .001, η2p = .004. Post hoc analysis revealed that participants’ satisfaction with their community-connectedness decreased significantly from T1 to T2 (Mdifference = 2.075, p = .002, 95% CI = 0.59, 3.56) and increased from T2 to T3 (Mdifference = −2.43, p ≤ .001, 95% CI = −3.92, −0.939). There was a statistically significant difference in participants’ satisfaction with their future security over time, F(1.99,4,352.82) = 27.70, p ≤ .001, η2p = .013. Post hoc analysis revealed that participants’ satisfaction with their future security significantly decreased from T1 to T2 (Mdifference = 1.63, p = .002, 95% CI = 0.48, 2.77) and increased from T1 to T3 (Mdifference = −1.94, p ≤ .001, 95% CI = −3.13, −0.76) and T2 to T3 (Mdifference = −3.57, p ≤ .001, 95% CI = −4.69 to −2.45). There was a statistically significant difference in participants’ satisfaction with their spirituality/religion over time, F(1.99,4350.23) = 7.82, p ≤ .001, η2p = .004. Post hoc analysis revealed that participants’ satisfaction with their spirituality/religion decreased significantly from T1 to T3 (Mdifference = 1.78, p = .003, 95% CI = 0.47, 3.09) and from T2 to T3 (Mdifference = 1.91, p = .002, 95% CI = 0.59, 3.23). The means, standard deviations (SDs), and the F-ratios of the one-way repeated measures ANOVAs for the wellbeing scale, and the respective subscales separated by time can be found in Table 1.
Discussion
The purpose of this article was to quantitatively assess adults’ mental health and overall wellbeing over time during the first 16 months of the pandemic in Ontario, Canada (April 2020–August 2021). Interestingly, results showed that participants’ self-reported mental health increased significantly over time, whereas their satisfaction with their mental health significantly decreased. Similarly, participants’ satisfaction with their personal relationships decreased significantly over the course of the pandemic, whereas their satisfaction with community-connectedness decreased from April to August 2020 and increased from August 2020 to August 2021. Participants’ satisfaction with their safety and future security decreased from April to August 2020, but increased from April 2020 to August 2021, respectively.
It is surprising that participants’ self-reported mental health improved over time, as many authors have reported that the pandemic has negatively impacted the mental health of various populations (e.g., Amendola et al., 2021; Jenkins et al., 2021; O’Connor et al., 2021; Passos et al., 2020; White & Van Der Boor, 2020). This said, participants’ improvement in mental health is consistent with what they reported in their demographic information, as the percentage of individuals who reported experiencing a mental illness and/or mood/anxiety disorder(s) declined over time. However, findings from the PWI-A revealed that participants’ satisfaction with their mental health significantly decreased over time. While this appears inconsistent with the mental health improvements noted above, it is possible that while self-reported diagnosable mental health disorders reduced over time, those experiencing challenging levels of stress throughout these 16 months of the pandemic might have felt more run-down or fatigued by the end of the study, but not to the point of experiencing a disorder. It is also worth noting that while the number of participants who reported experiencing a mental illness and/or mood/anxiety disorder(s) declined over time, it is plausible that the reported decline is due to participant attrition and is not indicative of improved mental health conditions. Additionally, even though participants’ mental health scores improved over time, at every time point participants’ average scores were still below the cut-off of 76, indicative of the presence of mental disorders (Kelly et al., 2008). The presence of mental health conditions during the pandemic aligns with work conducted by Amendola et al. (2021). Specifically, the authors explored the impact of the COVID-19 pandemic on the mental health of Italian adults (N = 299) during the early stages of the pandemic (i.e., after a month of isolation due to COVID-19; Amendola et al., 2021). The authors concluded that females reported higher symptoms of depression and anxiety, compared to males (Amendola et al., 2021). This finding is worth noting as 90% of participants in the current study identified as female. Similarly, Passos et al. (2020) investigated the mental health of adults in Portugal and Brazil (N = 550) during the COVID-19 pandemic (May 27–July 8, 2020) and found that the frequency of mental health conditions was considerably higher than pre-COVID-19 levels. Moreover, Chandola et al. (2020) explored whether there was an increase in prevalence and incidence of mental disorders among adults (N = 17,761) living in the United Kingdom during the first months of lockdown due to the COVID-19 pandemic. The authors concluded that 29% of adults who did not report a mental disorder pre-pandemic experienced a mental disorder during the early stages of the COVID-19 pandemic (April 2020; Chandola et al., 2020).
It is worth noting that the available data regarding individuals’ mental health during the COVID-19 pandemic is primarily cross-sectional and occurred during the early stages. The current study is among one of the first to report longitudinal data. Thus, in order to compare the mental health of Ontario adults to other populations, more research is needed. The contrast between study findings may also be attributed to the difference in public health protection mandates among countries, as well as demographic characteristics. For context, data collection at time points 1 and 2 occurred during the first wave of the pandemic, wherein Ontario was primarily in a lockdown (e.g., closure of schools, businesses, and non-essential services), and COVID-19 case counts were high (Ontario COVID-19 Science Advisory Table, 2021). At time 3, the province had re-opened with mask and vaccination requirements, and indoor services with larger numbers of people resumed (Government of Ontario, 2021). It is thus plausible that at the beginning of the pandemic (i.e., during times 1 and 2), participants might have experienced poorer mental health due to the unknowns, fears, and the novelty of the pandemic, compared to 1-year follow-up. As time progressed, it is not surprising that participants’ mental health status improved as individuals learned more about safety precaution that could be taken to avoid COVID-19 infection. Furthermore, it is possible that the improvement in Ontario adults’ mental health was positively associated with the public health mandates lifting, such that over time the Ontario government gradually removed protections, allowing people to return to a new “normal,” despite concurrently rising case numbers (Ontario COVID-19 Science Advisory Table, 2021). By lifting the mandates, it is possible that individuals perceived COVID-19 was significantly less concerning despite little data available on community transmission to support this decision (Manuel et al., 2021). It is thus possible that people no longer perceived COVID-19 to be a threat, which could aid in explaining their improvement in mental health. This interpretation aligns with the Normalization Process Theory, which suggests that “practices become routinely embedded–or normalized–in social contexts as the result of people working, individually and collectively, to enact them” (May et al., 2009, p. 2). It is thus plausible that over time, public health protections might have become normalized and therefore, COVID-19 was perceived as less of a threat to participants’ mental health. It is also important to situate the findings of the current study in the context of participant demographics. Specifically, the study sample primarily consisted of White women of high socioeconomic status and thus, the mental health of Ontario adults of different genders, ethnicities, and low socioeconomic status is largely unknown. This information is important, especially considering international researchers have found that the COVID-19 pandemic has negatively impacted the mental health of men (Park & Yu, 2022), sexual and gender minority populations (Moore et al., 2021), and ethnic minorities (Smith et al., 2020), with minority populations being disproportionately affected (Moore et al., 2021). Moreover, Chung et al. (2021) explored whether the mental health and wellbeing of adults who were socioeconomically disadvantaged was worse than those of high socioeconomic status. The authors concluded that socioeconomic inequality, specifically in relation to mental health and wellbeing, was exacerbated by individual’s financial concerns during the pandemic (Chung et al., 2021). It is advised that further research be conducted to explore the impact of the pandemic on the mental health of minority populations in Ontario.
Participants’ satisfaction with their personal relationships significantly decreased over time, while their satisfaction with community-connectedness decreased during the initial stages of the pandemic and increased 1-year follow-up. There is little available data on how the pandemic might impact one’s personal relationships broadly. However, Pietromonaco and Overall (2022) suggested that separation, isolation, and loss as a result of the COVID-19 pandemic might negatively impact couples’ relationships. Thus, it is possible that due to pandemic-induced stressors, participants’ personal relationships were strained over the course of the pandemic. Additionally, in the study conducted by White and Van Der Boor (2020), the authors concluded that participants who experienced community-connectedness during the early stages of the pandemic had lower levels of depression symptoms. Similarly, in the current study, participants’ satisfaction with community connectedness increased from August 2020 to August 2021, whereas the prevalence of mood/anxiety disorders appeared to decrease.
It is also worth noting that during the timeframe in which data were collected, several changes to public health guidelines occurred, including the introduction of COVID-19 vaccines. During the pandemic, many people consulted the Internet and social media for health information, which presented concerns regarding the legitimacy of information and sparked an anti-vaccination movement, contributing to vaccine hesitancy (Puri et al., 2020). This movement created divisiveness among many (Djuric, 2022), potentially impacting the personal relationships of participants in the current study. In a pre-pandemic study conducted by Gunaratne et al. (2019), the authors explored the anti-vaccination discourse on Twitter and suggested that pro- and anti-vaccine content naturally separate into distinct communities, amalgamating like-minded individuals. Thus, it is not surprising that participants’ satisfaction with community-connectedness increased while their personal relationships decreased, as it is possible that participants felt a part of their respective communities.
While participants’ satisfaction with their safety and future security decreased from April to August 2020, it increased from April 2020 to August 2021. It is possible that while public health protections changed over time, some participants’ increased satisfaction in safety and future security was, in part, attributed to the release of COVID-19 vaccines. In a study conducted by Syan et al. (2021), the authors examined the extent to which Ontario adults (N = 1,367) were willing to receive the COVID-19 vaccine and found that 82.8% of their sample was willing, and 74.2% perceived the vaccine to be safe. Coincidental to this timeframe was the introduction and mass availability of COVID-19 vaccinations. Thus, it might be possible that participants’ satisfaction with their personal safety and future security in the current study was, in part, related to the introduction of vaccines. Additionally, it is reasonable that participants’ perception of safety and security related to COVID-19 improved over time as more evidence emerged and the public developed a better understanding of the realities of the viral illness. Specifically, Ioannidis et al. (2020) concluded that individuals younger than 65 years accounted for 4.5%–11.5% of all COVID-19 deaths in European countries and Canada. Furthermore, The OpenSAFELY Collaborative (2020) found that women are two times less likely to die from COVID-19 compared to men. This evidence highlights that risk of death due to COVID-19 is low in our sample, based on age and gender alone, potentially contributing to participants’ increased perception of safety and security.
Limitations and Future Directions
This study is not without limitations. First, although honesty demands (Bates, 1992) were employed in the surveys to reduce bias, the risk of social desirability bias remains, as all data were collected using self-report measures. Second, the PWI-A was slightly altered to specify satisfaction with mental and physical health, respectively, whereas the validated tool included one question on satisfaction with health as a whole. As such, the altered tool was not validated in the format as it was used. Such considerations need to be considered when scoring the tool, analyzing the data, and interpreting the findings. Third, the current study lacks generalizability, as the sample was predominately comprised of highly educated women of European origins in Ontario, Canada. Future studies are encouraged to stratify their sample by targeting groups of diverse ethnic origins and genders, in order to achieve greater diversity and representation among the population. Given that the pandemic disproportionately affected those of low socioeconomic status and marginalized groups (Mishra et al., 2021), efforts are needed to more effectively target these individuals in future research. One way to accomplish this might be through targeted and purposeful recruitment methods. Researchers of future studies might consider targeting members of specific groups on social media (e.g., Facebook groups dedicated to rural locations, minority groups, and diverse populations) to increase representation among their sample. Furthermore, the current study did not investigate the association between demographic variables and mental health, which is a limitation. However, since there is reason to believe that demographic variables are likely to be related to the outcome of interest—mental health—a decision tree analysis was conducted. The inclusion of this analysis was beyond the scope of the current article as the profiles generated were based on demographics and additional health outcomes from the larger HOPE study that were not applicable to the current article. As such, a subsequent manuscript is currently in preparation (Shillington, Guerrero, et al., 2023). Lastly, significant attrition existed between baseline and follow-up time points. It is possible that attrition was due to respondent burnout, as many COVID-19-reated studies were occurring during this timeframe. In an effort to help mitigate the impact of participants loss to follow-up, multiple imputation was employed to handle missing data. A total of 2,188 participants were included in all analyses.
Conclusion
The COVID-19 pandemic has significantly impacted the self-reported mental health and wellbeing of Ontario adults. Specifically, the mental health of Ontario adults reportedly improved over time, while their perceived wellbeing declined in several domains. Participants’ satisfaction with their standard of living, physical health, mental health, personal relationships, and spirituality/religion decreased from April 2020 to August 2021, whereas their satisfaction with community connectedness only decreased from April to August 2020. Moreover, participants’ satisfaction with their safety and future security increased over time. Findings from the current study can aid in understanding the long-term impacts that the pandemic has had on Ontario adults and should be taken into account when designing interventions targeting the mental health and wellbeing of Canadians.
Footnotes
Acknowledgements
We would like to thank the participants of this study, as well as Varsha Vasudevan and Nia Contini for the research support they provided for this project. Dr. Leigh Vanderloo was supported by a CIHR Fellowship Award at the time of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.