
Abstract
Pre-exposure prophylaxis (PrEP) prevents HIV contraction in HIV-negative individuals. Despite higher risks, uptake is low among young men who have sex with men (YMSM). This study investigates barriers to PrEP uptake in U.K. YMSM, where treatment has recently been approved within services. Semi-structured interviews with 10 YMSM living in the United Kingdom were analyzed using data-driven reflexive thematic analysis. Analysis highlighted three principal barriers to PrEP uptake: lack of perceived necessity, lack of knowledge, and perceived acquisition discomfort. YMSM experience unique barriers to PrEP uptake. Recommendations for tackling barriers included implementation of an online application, alongside educational measures.
Due to the relatively recent rollout of pre-exposure prophylaxis (PrEP) in the United Kingdom, young men who have sex with men (YMSM) living in the country may experience unique barriers to PrEP uptake, resulting in low levels of PrEP use. These barriers must be investigated to determine how best to overcome them.
PrEP refers to any medication that prevents the contraction of disease in those not yet exposed to the disease-causing agent (Centers for Disease Control [CDC], 2020). However, PrEP has come to refer specifically to a pill that prevents HIV contraction in HIV-negative individuals (CDC, 2020). PrEP can be taken daily or on-demand a day before and for 2 days after sex, and when taken as prescribed is 99% effective at preventing HIV transmission (Buchbinder, 2018; Terrence Higgins Trust, 2020). PrEP is targeted at those at a high risk of HIV infection. Globally, men who have sex with men (MSM) are 28 times more likely to contract HIV, compared to those of the same gender identity and age (United Nations AIDS, 2022), with a quarter of MSM partaking in condomless sex (World Health Organization [WHO], 2012). Thus, this group is most frequently targeted for PrEP uptake (WHO, 2012). PrEP has been Food and Drug Administration (FDA) approved and distributed in the United States since 2012 (Hunt, 2019). However, National Health Service (NHS) England (2020) only started distributing PrEP for free to the public in October 2020, with the earliest U.K. NHS distribution of PrEP being in Scotland in 2017 (Christie, 2017). Furthermore, while the FDA has now approved the bimestrial pre-exposure injection Apretude for use as a prophylaxis in the United States, at the time of publication, Apretude is yet to be approved for such use in the United Kingdom (Tantibanchachai, 2021). Therefore, PrEP remains the only prophylactic HIV medicine publicly available in the United Kingdom.
While HIV is no longer a serious threat to life in the United Kingdom, a necessity still exists for MSM at a higher risk of HIV infection to take PrEP (Gee et al., 2019). In the United Kingdom, less than 1% of individuals with HIV die from complications related to AIDS, and the rate of new HIV infections has been consistently falling (Public Health England [PHE], 2019). Adherence to antiretroviral therapy (ART) suppresses viral load (i.e., HIV viral load becomes undetectable). HIV transmission cannot occur among sexual partners when a person living with HIV has an undetectable level of virus in their body. Thanks to effective adherence to ART, 97% of HIV-positive individuals living in the United Kingdom achieved an undetectable viral load (PHE, 2019). However, rates of HIV transmission in the United Kingdom are still relatively high among MSM, especially in London, whose residence made up 37% of all new HIV cases diagnosed in the United Kingdom in 2020 (Terrence Higgins Trust, 2022). Furthermore, one in 16 HIV-positive MSM are unaware of their HIV status (PHE, 2019). Without access to and adherence to ART, HIV can be fatal. Those who learn of a positive HIV status later in the disease process, relative to those diagnosed shortly after transmission, are at increased risk of death. Within the United Kingdom, 42% of HIV cases are diagnosed late in the disease process (Martin et al., 2021), decreasing the efficacy of ART and increasing the risk of death within a year of diagnosis tenfold (Sobrino-Vegas et al., 2016). Additionally, those who are unaware of their HIV-positive status and are not virally suppressed on ART may transmit HIV to their sexual partners. PrEP is one of the most successful ways to limit the transmission of HIV (Kessler et al., 2014) and avoid long-term health complications. Moreover, Keen et al. (2020) observed that PrEP use was associated with lower HIV anxiety among MSM at high risk of infection. Therefore, PrEP use is not only an effective method to reduce transmission but also a practical tool to diminish anxieties surrounding becoming HIV positive. As such, it is important to understand reasons why at-risk groups may not wish to utilize this multifunctional safety measure.
Despite the aforementioned risks, limited numbers of MSM are taking PrEP. The recency of the U.K. NHS rollout suggests that PrEP is likely being underconsumed in the United Kingdom, and limited data exist for the frequency of PrEP in the United Kingdom. Within the United States, only 35% of high-risk MSM take PrEP, and PrEP uptake is particularly low for 18- to 24-year-olds (Finlayson et al., 2019). This suggests that MSM experience barriers that prevent them from taking PrEP. A review of the existing literature on PrEP uptake helps elucidate some potential barriers to PrEP uptake from many different MSM samples.
Potential Barriers to PrEP Uptake
The stigma surrounding PrEP repeatedly appears as a key barrier to uptake across studies. Research examining 25 online articles and 28 online posts found beliefs and attitudes toward PrEP to be the most frequently reported barrier to PrEP uptake for MSM (Hannaford et al., 2018). A large proportion of attitudes revolved around the stigmatization of PrEP users as promiscuous, suggesting that a fear of being labeled as promiscuous prevents a proportion of MSM from taking PrEP (Hannaford et al., 2018). However, the observational nature of Hannaford et al. (2018) prevented researchers from actively investigating the cognitions underlying this stigma. Dubov et al. (2018) overcame this limitation by using qualitative interviews to obtain first-hand accounts of the stigmatizations experienced by 43 PrEP-using MSM. This study observed that much of the promiscuity-based stigmatization experienced was built upon stigma surrounding HIV (Dubov et al., 2018). PrEP users claimed many MSM believed that those who contracted HIV deserved it for acting promiscuously and that PrEP was, therefore, a tool that permitted sexual irresponsibility without the deserved consequences (Dubov et al., 2018). The stigmatization of promiscuity among MSM, from other MSM, is frequently attributed to internalized homophobia (see Sietins et al., 2020; Tan, 2019). This may suggest that by encouraging the stigmatization of PrEP, internalized homophobia born from the societal stigma surrounding same-sex sexual relations can act as a significant barrier to PrEP uptake.
Another frequently reported barrier to PrEP uptake considered in research to date is associated with the known and perceived side effects of taking PrEP. Young et al. (2014) observed that while PrEP is reported as having very few negative side effects, the fear of potential negative side effects and perceived longer-term negative outcomes (beyond what might be reported or understood at this stage) act as a significant barrier to PrEP uptake for MSM. Accounting for the age of participants, Jaspal and Daramilas (2016) observed that it is specifically older MSM that distrust PrEP’s side effects, due to the observed severe side effects of previous HIV treatments, such as zidovudine. Therefore, while distrust of PrEP’s side effects may act as a barrier to uptake for MSM, this distrust may be stronger for certain MSM subcommunities due to past experiences, and as such further research is needed.
Studies suggest MSM do not feel comfortable obtaining PrEP from medical settings. In the United States, Patel et al. (2018) observed that nearly half of MSM seeking PrEP were rejected by their primary healthcare provider (PCP), with 52% of rejections attributed to the PCP’s perception that it is not their responsibility to prescribe PrEP, 21% being attributed to PCP lack of knowledge of PrEP, and 10% attributed to the PCP’s discomfort prescribing it. As such, feelings of discomfort surrounding obtaining PrEP from medical settings may often be attributed to a rational fear of rejection based on past experiences (Calabrese et al., 2017). Further discomfort experienced by MSM in medical settings may also be the product of fears and concerns surrounding judgment of their lifestyle. According to Hannaford et al. (2018), MSM feared that their frequency of sexual encounters would receive negative judgments from healthcare professionals. Online posts, such as those analyzed by Hannaford et al. (2018), can also be theorized as acting as barriers to PrEP uptake themselves, as posts detailing negative experiences with healthcare providers on the Internet may produce or affirm the aforementioned fears surrounding obtaining PrEP, leading to a reciprocal cause and effect relationship. This is particularly damaging to YMSM, who frequently use the Internet as a source of queer (and sexual health) information (Ross et al., 2018). Therefore, discomfort in medical settings acts as a barrier to PrEP uptake partially due to fears of judgmental and uninformed healthcare providers, a large proportion of which is multiplied by online posts related to PrEP, consequently affecting YMSM significantly more. However, despite these barriers to PrEP uptake, many MSM have successfully acquired PrEP. Therefore, facilitators to PrEP uptake must also exist.
Potential Facilitators to PrEP Uptake
A common facilitator to PrEP uptake, from the reviewed literature, is the frequency of unprotected sex in the MSM community. Survey research revealed that having unprotected anal sex with more than five partners in the past year significantly increased an individual’s willingness to take PrEP (Frankis et al., 2016), and as such, it is theorized that frequent unprotected sex is a key facilitator to PrEP uptake. Research has shown YMSM have more unprotected sex compared to MSM in general and, consequently, should be more willing to take PrEP (Frankis et al., 2016; Gray et al., 2020). Despite Frankis et al. (2016) observing that 18- to 25-year-olds were most willing to take PrEP, data show that this age category has one of the lowest levels of PrEP uptake (Finlayson et al., 2019). Thus, frequent sex without a condom may be too simple an explanation of why MSM are motivated to take PrEP. A cross-sectional Internet-based survey of 4956 MSM observed that MSM who perceived themselves at higher risk of HIV infection had an increased interest in PrEP acquisition (Krakower et al., 2012). This may suggest that only YMSM who understand that frequent unprotected sex increases their risk of HIV infection are motivated to obtain PrEP. Furthermore, interviews with 13 PrEP-using MSM observed that MSM claimed to take PrEP to increase intimacy with their sexual partners via condomless sex and to reduce the anxiety of contracting HIV (Harrington et al., 2020). Harrington et al. (2020) thus elucidate that PrEP uptake in MSM communities is facilitated by more than solely a desire to have condomless sex. While YMSM were most willing to take PrEP, their more limited conceptualization of the benefits of PrEP may have prevented them from becoming motivated enough to acquire PrEP. Equally, a theorized lack of knowledge and concern for the risks of unprotected sex, potentially a product of the scarcity of HIV education in schools (Raifman et al., 2018), may affect YMSM’s motivation to obtain PrEP, despite their higher incidence of unprotected sex. Alternatively, other unique barriers to YMSM obtaining PrEP may prevent uptake, regardless of motivation.
PrEP Uptake in YMSM in the Context of the United Kingdom
Existing literature suggests that age is an important factor affecting barriers to PrEP uptake experienced by MSM. As noted, US YMSM have one of the lowest PrEP uptake rates. Furthermore, while PrEP has been made routinely available at differing times throughout the four nations of the United Kingdom (in 2017 in Scotland and in 2020 in Wales, Northern Ireland, and England), the rollout of PrEP in all nations of the United Kingdom has occurred relatively recently, compared to the United States (Terrence Higgins Trust, 2021). Therefore, due to the recency of the NHS rollout, it can be assumed that levels of PrEP uptake are even lower for YMSM in the United Kingdom. Furthermore, an individual’s age and country of residence may interact to produce distinct cultural obstacles, and it is, therefore, essential to investigate the barriers to PrEP uptake experienced by YMSM living in the United Kingdom.
YMSM, defined here as MSM aged between 18 and 24, have very little first-hand experience with the severity of HIV. Thanks to highly active ART, the mortality rate from HIV dropped significantly between 1995 and 1998 and has remained relatively low since (Croxford et al., 2017). Furthermore, the United Kingdom has experienced significantly fewer AIDS-related deaths compared to the United States, even once population differences are accounted for (Bourne et al., 2012). Therefore, YMSM in the United Kingdom are unlikely to have first-hand experiences with the deadliness of HIV. This could have a wide range of effects; for example, it could affect how serious a threat YMSM in the United Kingdom perceive HIV to be, along with how much they stigmatize it and how much knowledge they have about it.
While PrEP is free in the United States as part of the Ready, Set, PrEP program, and some free testing programs are available in certain states, lab tests and clinic visits necessary to obtain a prescription may not be free or easily accessible to everyone (CDC, 2022; Enos, 2019). This is a barrier to PrEP uptake for MSM in the United States, especially YMSM, who are less likely to have a steady income stream and may not have the same level of control over their daily lives as older adults (Pérez-Figueroa et al., 2015). However, as PrEP is completely free on the NHS in the United Kingdom, this financial barrier is removed. Still, obtaining PrEP from the NHS may present unique barriers for YMSM. At the time of writing, PrEP is only available in the United Kingdom from sexual health clinics (Robinson, 2021), which may pose a physical barrier for those who do not live near such clinics. This logistical barrier could be overcome by allowing general practitioners (GPs) to prescribe PrEP, an idea proposed by the United Kingdom government when they doubled the national funding for PrEP in March 2021 (Robinson, 2021). However, despite this provision, unique barriers to PrEP uptake for YMSM may still exist in the United Kingdom. Unlike those privately insured in the United States, with some possibility of additional freedom of choice for healthcare providers based on publicly available information (e.g., extent to which a provider publicizes being queer-friendly), MSM in the United Kingdom cannot be certain that their GP is amicable toward and knowledgeable about queer issues. Healthcare provision in the United Kingdom typically involves being registered to a doctor’s practice, which one may have a choice over based on proximity. However, it is often not possible to check the areas of expertise of a clinician (GP) prior to a visit, and appointments are often made based on which GP is available, due to scarcity of appointments (Guthrie, 2002). Discomfort in medical settings frequently reported by MSM (Patel et al., 2018) is probably compounded for YMSM, as young people often report being too embarrassed and worried to talk to their GP about medical issues (Morrison, 2014). Furthermore, YMSM obtaining PrEP are likely to have embraced their sexuality more recently and, thus, are potentially less comfortable discussing their sexual identity, and associated activities, within medical settings (McDavitt & Mutchler, 2014). Therefore, YMSM living in the United Kingdom may feel particularly uncomfortable obtaining PrEP from medical settings.
Finally, the quality of sexual education that YMSM in the United Kingdom receive may differ markedly from that of MSM in the United States and older MSM in the United Kingdom. As of March 2017, sexual education became compulsory within all schools in England (Sellgren, 2017). While this new compulsory sexual education would not have affected the current cohort of YMSM, it does reflect a more liberal approach toward sexual education in the United Kingdom, which may have provided YMSM in the United Kingdom with some sexual health knowledge. Conversely, due to the recent NHS rollout of PrEP, YMSM in the United Kingdom may have garnered less knowledge about PrEP from the media, compared to YMSM in the United States, for whom PrEP has been commercially available since 2012 (Enos, 2019). These levels of sexual health and PrEP-specific knowledge may have diverse effects on barriers to PrEP uptake, ranging from an increase in trust in PrEP to a decrease in stigmatization of PrEP users.
The Current Study
YMSM in the United Kingdom occupy a unique, understudied culture that may generate specific barriers, as well as facilitators, to PrEP uptake. This qualitative interview study was, therefore, formulated with the aim of evidencing the most prevalent of these barriers expressed by YMSM living in the United Kingdom. This study seeks to formulate interventions and recommendations for healthcare providers to encourage a larger uptake of PrEP in this at-risk community, as well as to consider future avenues for research in this vital area. A qualitative approach was considered most appropriate due to the underresearched nature of this topic and a need to explore what and how barriers and facilitators to PrEP uptake are experienced (Silverman, 2022). As such, the primary research question was, “What are the principal barriers to PrEP uptake experienced by YMSM living in the United Kingdom?”
Method
Participants
Interview participants were required to be between 18 and 24 years old, living in the United Kingdom, and identify as MSM. To ensure a comprehensive conversation about PrEP, participants were required to have some knowledge of PrEP. To guarantee participants met these criteria, a short pre-interview survey was administered to all participants asking whether they had some preexisting knowledge of the drug PrEP, what it does, and who should take it. Other than these inclusion requirements, no further sampling approaches were utilized, and individuals were invited to take part successively. In total, 10 YMSM were recruited through volunteer sampling, utilizing relevant gatekeepers (e.g., lesbian, gay, bisexual, and transgender [LGBT+] university societies). Age ranged from 18 to 22 years (M = 19.9, SD = 1.14). Additional demographic details can be seen in Table 1.
Demographic Characteristics of the Interview Participants
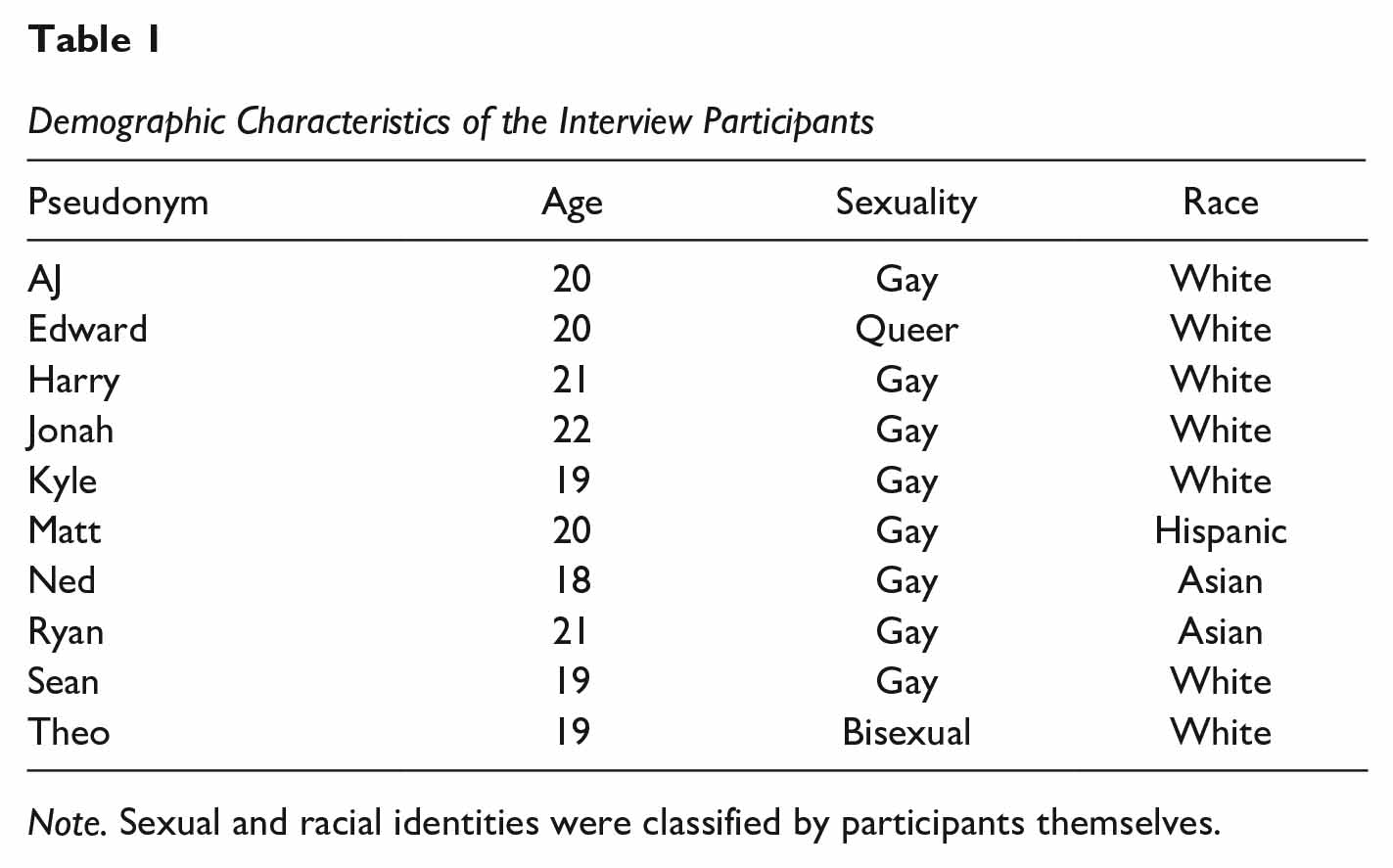
Note. Sexual and racial identities were classified by participants themselves.
Data Collection
Interview questions were formulated based on background reading, with a particular focus on contentious points from previous research. Feedback on the appropriateness of questions was sought from within the researchers’ networks, which included members of the YMSM community. Interview questions discussed various aspects of PrEP knowledge, perceptions, and misconceptions. Interviews were conducted over Microsoft Teams (M duration = 27 min; SD = 11 min). Recordings were uploaded to a secure institutional research drive. After the interview, participants were sent a debrief sheet further outlining the study as well as links to support and to the researchers’ contact details. Recordings were transcribed, and names were anonymized using pseudonyms for use in quoted extracts. In aiming to be more transparent and open about data adequacy (see Vasileiou et al., 2018), the decision to cease data collection and proceed to analysis was based on several factors: the researchers’ previous experience with similar projects, reflections on the more sensitive nature of our topic (i.e., increased recruiting challenges), project time constraints, the richness of interview data, and perceptions of data sufficiency. As such, the number of interviews conducted was considered appropriate when comparable recurring insights were observed by researchers in later interviews (Kelly, 2010) and when the data corpus was viewed as sufficient to warrant detailed understanding when considering the proposed analysis and research question (Braun et al., 2023). Ethical approval for this study was granted by the author’s institutional ethics committee (code: UG 20-088). The interview schedule used to guide data collection is available as supplementary material. Given the vulnerable nature of the participant group and associated ethical restraints, transcript data cannot be made available (see Prosser et al., 2022, for a detailed discussion of open data practices in qualitative research).
Analytic Approach
Data were analyzed utilizing reflexive thematic analysis (Braun & Clarke, 2019). Data were coded and assessed via a process of continual reflection, considering assumptions, and actively engaging with the data in an organic and evolving way, in order to provide an in-depth analysis of the perspectives given (Braun & Clarke, 2021). Coding took a primarily semantic approach, exploring specific surface meanings from participant accounts. This allowed focus on data specifically informing barriers to PrEP uptake, with the aim of identifying barriers consciously perceived to be blocking PrEP uptake. However, subconscious cognitive processes, such as state shame, 1 can present unique barriers to PrEP uptake. Therefore, where necessary, a latent approach was also utilized, requiring a more interpretive take on the underlying meaning of some accounts, exploring concealed ideologies or assumptions that inform or produce the semantic content in the data (Byrne, 2022). Codes were assigned to meaningful units of data, and similar descriptors were collated to form candidate themes. These stages were conducted by the first author of this paper. No specific software was used for coding, with the researcher keeping detailed notes for their codes within the original transcript data. In collaboration with the second author, themes were reviewed by identifying reinforcers and contradictors within the data, to ensure that they were the most pertinent themes in relation to the research question. Analysis was data-driven (inductive), approaching the data without a preconceived framework in mind (Willig, 2022), since the research itself examines a unique subgroup of MSM. This was approached from a critical realist viewpoint, identifying responses as indicative of barriers to PrEP uptake that objectively exist within a participant’s environment but also reflecting how certain responses were treated as techniques utilized to construct participant realities that also pose barriers to PrEP uptake. This acknowledges that participant truths may be a product of the wider social world around them. An analysis log was kept during the coding and theme development process, noting candidate themes, subcategories, codes, and associated data extracts, allowing the researchers to reflect on and return to aspects of the data and analytic outcomes in line with the iterative process of reflexive thematic analysis. This log is available to view as Supplemental Material.
Reflections
Positions of both researchers and participants should be noted. This does not invalidate the research but simply provides context to interviews and analytic processes. Reflexivity is central to reflexive thematic analysis, acknowledging that knowledge is never free of researcher influence, both in terms of analysis and study design (Braun et al., 2023). Both researchers are MSM, which may impact the analytic claims made. The primary investigator, who was responsible for the study design and conducting interviews, was also a part of the YMSM community. Interviews were, therefore, formulated based on personal experiences of PrEP-perceptions within the U.K. YMSM community as well as existing research in this area. This permitted an interview more focused on the principal unique barriers to PrEP uptake specifically experienced by this community but is in no way an exhaustive account of all the barriers experienced by YMSM in the United Kingdom. In carrying out the interviews, a YMSM identity arguably may have elicited more open and honest responses from participants, as participants likely felt more comfortable talking to a member of their community (Knapik, 2006). From the participant’s perspective, it should be noted that one participant had a parent who was a sex therapist, one was a medic interested in queer health, and another involved in equality matters at their university. 2 These participants were likely to have more knowledge about PrEP compared to most YMSM. However, this additionally allowed a more nuanced analysis of barriers from a range of YMSM living in the United Kingdom.
Results
Our reflexive thematic analysis generated three core themes related to principal barriers to PrEP uptake for YMSM in the United Kingdom. They were (a) perceived necessity of PrEP, (b) knowledge about PrEP, and (c) perceived comfort of acquiring PrEP. These themes will now be outlined in-depth, reporting participant accounts from interview transcript data to evidence our interpretations.
Perceived Necessity of PrEP
A key barrier to PrEP uptake for many participants was a perceived lack of necessity to take PrEP, attributable to three principal perceptions. First, participants often seemed to have a narrow conceptualization of PrEP and its benefits. Second, participants perceived other methods of protection as suitable enough to nullify PrEP consumption. Finally, certain participants did not view PrEP as necessary for them in their current lifestyle.
Starting with the narrow conceptualization of PrEP, many framed PrEP solely as a tool that reduces the risk of contracting HIV in individuals already having high-risk sex: Pre-exposure prophylaxis. . . can be taken, if you’re kind of, worried that you’re, I guess involved in the kind of high-risk behaviors that means you’re more susceptible to catching HIV. So, it’s like a medication to take um yeah, I don’t know, um just as precautionary. . . and then high-risk in terms of sexual high-risk behaviors I guess yeah not using condoms. (Matt)
While correct, such statements unidirectionally limit the relationship between PrEP consumption and condomless sex. Participants viewed PrEP’s sole purpose as being a precautionary tool used to reduce the risk of HIV contraction during condomless sex. Very few participants expressed that PrEP can be a beneficiary tool that permits individuals to have condomless sex when they did not before. This perception is qualified by claims that PrEP use would not affect an individual’s frequency of condomless sex: It should be used with condoms like you know contraception as well, well not contraception. You know having safe sex as well you can’t just use it on its own, but I mean I think to be honest it seems like a lot of the gay community probably see PrEP as an alternative. (Matt)
Therefore, certain participants did not perceive PrEP to have any unique benefits, compared to condoms, for example, thus reducing the perceived necessity to take PrEP. Furthermore, even when participants did view PrEP as permitting more condomless sex, the subjective benefits of this were also extremely restricted: Therefore, I would move on to PrEP if I wanted to stop wearing a condom. I feel like that’s probably why I would start taking PrEP because otherwise I would be wearing a condom and then, I wouldn’t worry. (Harry)
While this participant does acknowledge that PrEP use would facilitate condomless sex, the benefits of this are restricted to not having to wear a condom. Participants in this study were unable to expand their conceptualization of the benefits of PrEP to include the emotional benefits of such an effective and convenient form of protection. This suggests that participants’ perceived necessity of PrEP was limited because they incorrectly believed that PrEP does not have any or many unique benefits, compared to other forms of protection.
It can, therefore, be maintained that the use of other forms of protection also reduces participants’ perceived necessity to take PrEP. The most popular contraception discussed among participants was a condom, as it was discerned as more universally effective than PrEP, since it could prevent the contraction of multiple sexually transmitted infections (STIs). However, considerations of HIV as a unique factor to consider in this regard were not considered: I always just engaged in safe sex so it’s like, do I need this added preventative measure if I’m already sort of like I’m doing what I should be doing to make sure that both me and my partner are safe. (Jonah) So maybe like the perception of me thinking that condoms are like more effective in the sense that it protects us from uh various diseases or like STIs. (Ned)
PrEP was, therefore, perceived as an added inconvenience that provides little extra protection when used in tandem with condoms or misperceived as a less effective HIV prevention method compared to condom use alone. Therefore, while individuals may view PrEP as unnecessary due to the perceived efficacy of condoms, for some individuals, this perceived lack of necessity may be based upon misinformation. Furthermore, in the absence of condoms, the utilization of other HIV risk-reduction strategies decreased the perceived necessity to take PrEP: [Talking about unprotected sex] Uh. It depends who it’s with. If it’s someone that I know that’s definitely not got any STIs then I don’t care; just fine if it’s someone that is more like a hookup then, I dunno it’s a bit. The next day I’ll be a bit like ohhhh maybe I shouldn’t have done that. (AJ)
As this extract demonstrates, some participants appeared to utilize serosorting, the procedure of selecting sexual partners based on their HIV status, to prevent themselves from contracting HIV, and many of these participants only felt comfortable doing so when having sex with acquaintances or friends of friends. This risk-reduction tool was viewed to alleviate the need for PrEP, if one can confidently trust the health status of a sexual partner. In relation to this, STI testing was also referred to as a protection technique, in the absence of condoms: [Referring to unprotected sex] normally like me now, I know that that’s risky behavior and it’s like almost like every single time you wake up in the morning you’re always like that was so stupid, but if I test every four weeks or whatever then everything’s fine (Matt)
What is suggested here does demonstrate good testing behavior; however, getting frequently tested is not itself an HIV prevention technique, as early detection of HIV does not lead to HIV eradication (McGarrity & Huebner, 2014). Therefore, individuals are apathetic to taking PrEP due to a range of different perceived HIV, and STI, prevention methods. However, the varying legitimacy of these techniques means that some reduce the perceived necessity of PrEP uptake in ways that put an individual’s sexual health at risk.
The use of alternative protection methods was not the only factor that altered YMSM’s perception of PrEP’s appropriateness in our sample, leading to a limited perceived necessity to take PrEP. There were also situational factors discussed that were seen to prevent the need for PrEP uptake, the most common being a monogamous relationship: I would think that it’s not necessary, like if I was if I will be in a stable relationship for a long term then there probably and then cos if we get tested and stuff then we probably do not have the need to take PrEP, like it would just be an extra step every day or like having to go to get PrEP even if it’s free. (Ned) At the time it was offered to me I was in a relationship; so, we were having unprotected sex, but it was only ever with each other, and we had been checked uh. (Kyle)
Participants often partook in informed serosorting, utilizing STI tests to ascertain their partner’s HIV status before engaging in unprotected sex with a romantic partner, thus reducing the perceived need to take PrEP. However, as noted by Kyle, there is a chance that infidelity from a partner could result in HIV transmission within a relationship. However, many participants in monogamous relationships did not seriously acknowledge the potentiality of infidelity and the associated increased risk of HIV infection. Therefore, while being in a monogamous relationship did limit the perceived appropriateness of PrEP, it may not reduce the risk of HIV contraction enough for this to be considered a justifiable barrier to PrEP uptake.
Therefore, the perception of PrEP’s benefits, the use of other contraceptive methods, and perceptions of PrEP as personally inappropriate all affect the perceived necessity of PrEP, thus acting as barriers to PrEP uptake. In considering a potential model to PrEP uptake, views on the necessity of PrEP in one’s lifestyle may constitute the first barrier to YMSM implementing PrEP use. However, regardless of the level of perceived necessity to take PrEP, many participants felt that they did not have the requisite knowledge to do so.
Knowledge About PrEP
Participants often lacked sufficient knowledge in several different areas relating to PrEP. This lack of knowledge often revolved around the characteristics of PrEP, the requirements to be eligible for PrEP, and the process of acquiring PrEP, all of which may reduce the likelihood of PrEP uptake for YMSM: I don’t I don’t know where I would get it like um like I don’t know; is that the sort of stuff you can get like over the counter at Asda or you know, like the medical center in uni. And then on top of that the lack of knowing and not knowing who to ask is then like another issue. How do you how do you Google that like what do you type. (Sean) I have the knowledge of it but then I didn’t know if I really needed it, like there wasn’t really advertisements or like actual people or like posters advertisements telling me that I probably need PrEP. (Ned)
These differing gaps in knowledge produce unique barriers to PrEP uptake. For example, not knowing what online information about PrEP is true and what is false may create false negative perceptions surrounding PrEP that could prevent uptake. Furthermore, not knowing what the criteria for PrEP are could cause an individual to avoid going to acquire PrEP out of fear of getting rejected. And not knowing how to get PrEP and who to ask to resolve this issue could also act as a sizable barrier to PrEP uptake.
An explanation for this relative lack of knowledge can be theorized from accounts of the specialized websites utilized as sources of PrEP information by those who did have knowledge about PrEP: I think I’ve seen it on medical websites and also websites that talk about like news within like LGBT communities and things like that. (Theo) A lot of the times it’s like you need to collect small pieces of information from like all these like different like sources and then like piece together, but there’s no like one coherent thing that’s like here’s all the information you need to know. (Ryan)
Participants spoke about having to actively acquire and assemble information about PrEP from medical and LGBT+-specific websites. The effort required to actively assemble information from several sources to gain appropriate levels of knowledge was seen to limit a full understanding of PrEP and associated factors. One further knowledge base discussed was sexual education classes at school, which could be used to provide all YMSM with knowledge on PrEP. However, many participants claimed that their school education insufficiently informed them about PrEP and other LGBT+ sexual issues, beyond use of condoms and STI testing: In the same way that it’s sort of taught in schools like and like general safe sex stuff like use the condom use, go and get tested every so often, but there’s no I’ve never had anything about like oh you can try PrEP. Maybe like if that was implemented maybe it would raise more awareness and then, yeah, then it wouldn’t be like everyone’s burden to take it on themselves and be like PrEP what is it? (AJ) I mean like because you don’t get taught about gay sex in sex ed, so it’s like if you went to a sexual health clinic how are you meant to ask like if a certain pain is normal. (Sean)
Participants alluded to the fact that the sexual health education received at school was very heteronormative, mainly focusing on protection methods utilized by heterosexuals. This lack of education not only leaves YMSM without proper knowledge of PrEP, but also stigmatizes gay sex as an inappropriate discussion topic within school sexual health settings. This itself could also act as a barrier to PrEP uptake, as it ingrains the idea that gay sex should not be spoken about in public settings, such as GP clinics. It may also unfairly place the burden of learning about how to protect oneself on YMSM themselves, resulting in insufficient levels of knowledge about PrEP.
Therefore, many YMSM appear to have an insufficient level of PrEP-specific knowledge, and this could be attributed to the sexual health education received at school, which many participants claimed to be heteronormative and insufficient. In further considering a model for PrEP uptake here, initial considerations of whether PrEP is necessary for one’s lifestyle are followed by a need for understanding how PrEP works and where it can be accessed. Consequently, this leads YMSM to reflect on how they feel about acquiring PrEP.
Perceived Comfort of Acquiring PrEP
For participants who perceive the acquisition of PrEP to be necessary and have the requisite knowledge to do so, there was still potential for PrEP uptake to be prevented by how comfortable participants felt discussing their sexual health in medical settings. Perceptions of comfort were often affected by YMSM’s concerns about potential negative reactions from healthcare professionals: You’d like to always think that clinicians that you’re going to get are going to be very open and very um aware of LGBT health and that sort of thing but you never know, so I think yeah probably I’d go through with it up until the point that I actually am like in the waiting room, and I can imagine I’d be a bit nervous to actually meet the GP and kind of gage what they’re how comfortable they are about talking about you know LGBT health and PrEP. (Matt) The institution itself, like you don’t want to go to like the NHS and like be completely like you know disregarded, so it depends on also like their working culture and how they treat the individual because if, if I had a bad experience, I’ll be more inclined to not do that again. (Ryan)
Within these extracts, the fear of being judged by medical professionals produced anxiety for YMSM. This fear of being judged may be a product of concerns surrounding the ingrained homophobia of clinicians, which may be perceived to be more prevalent in older clinicians, of which GPs are a large proportion. As stated by one individual, Ryan, if he were to feel judged within a clinical setting while trying to obtain PrEP, this may prevent him from visiting sexual health medical settings in the future, which could be particularly damaging if he ever experiences serious sexual health issues. Furthermore, even if individuals do not perceive that a clinician will have a negative reaction to conversations about gay sex, there are still anxieties that the clinician will not have the requisite knowledge to prescribe PrEP. This concern was mainly articulated by participants such as Matt, in relation to GPs. This concern is based on the perception that GPs are not taught to cater to gay sexual health issues and will, thus, create an uncomfortable environment during PrEP consultations. However, this was not a view shared by all: I have experience with going and talking to doctors and you know talking to them about things that might be quite uncomfortable, um. So, yeah, in a way it would make it easier um and, in a way, obviously because I’m not like typical it might make it harder because places like Tavistock that’s what they do that’s their function whereas um in general you know the we are a smaller part of the population, so general STI places and GPs don’t have as much experience or anything. (Edward)
As a transgender man, Edward did not fear judgment within medical settings. This was due to the frequency with which he had experienced such conversations, specifically surrounding his gender identity, thus removing this barrier to PrEP uptake. However, he expressed significantly more concern that the GP would not have enough knowledge about PrEP to be able to confidently prescribe it to a transgender individual. Therefore, while these anxieties surrounding visiting a medical setting can affect all YMSM, it may affect certain subpopulations within this community significantly more.
Furthermore, even if an individual does not have any emotional concerns about obtaining PrEP from medical settings, their comfort can still be exacerbated by the inconvenience of having to visit said setting: Accessibility is probably going to be my number one; like, I know it’s bad but if I can’t do it on like with the medical center here. I don’t really fancy traveling all the way down to town just to pick up a tablet that I probably won’t even you know put to good use ummm for a while um, so and like I don’t know it’s just a matter of laziness, I guess. (Sean) At this point probably just convenience and access? It’s like is it the sort of thing that I need to go through a long process for? Or is it the sort of thing that I can just pop into like either my local clinic or like any other sort of health service and just be like, hey, I need PrEP; can I have some. (Jonah)
Linked to motivation, individuals seemed to perceive the inconvenience of visiting a medical setting to obtain PrEP to outweigh the benefit that PrEP uptake would confer. This is particularly a barrier for obtaining PrEP from an STI clinic, instead of a GP, as visiting an STI clinic generally requires more excursion or visiting an environment less familiar to the individual. Therefore, the perceived convenience of doing so can affect motivation to acquire PrEP and act as a barrier to PrEP uptake. Obtaining PrEP from a GP may circumvent this obstacle of inconvenience, in terms of both physical effort and, therefore, time required to obtain PrEP. Although, as previously mentioned, the GP presents unique obstacles that increase the perceived discomfort of obtaining PrEP from this medical setting. Participants were receptive to using video e-consultations as an alternative method of PrEP acquisition, due to the perceived low levels of discomfort: We’ve been doing a lot of consultations with patients online, and it has, yeah, I think it does. I don’t know it can it can sometimes be less awkward because you aren’t face to face. Maybe, yeah, actually having the conversation like this might make it less awkward. Being like this makes it less hard for me cos you could you quickly you close the consultation online you’re kind of out of that space and environment you can just get on with your day. Whereas being in person with them and they say something awkward, and you just have to sort of sit there and then leave awkwardly it’s a lot more, intense. (Matt)
When asked, many participants expressed that being able to obtain PrEP online would alleviate much of the discomfort associated with obtaining PrEP and make the process more convenient. Matt specifically claimed that an online PrEP service would also allow individuals to exit more easily if the situation became awkward or anxiety-inducing. Therefore, the perceived comfort of obtaining PrEP from a medical setting acts as a significant barrier to PrEP uptake, due to feelings of anxiety and perceptions of inconvenience. Online methods of PrEP delivery were viewed positively as one way to help to alleviate this barrier. Taking the outlined themes into account, the perceived comfort of acquiring PrEP signifies the final barrier in our model of PrEP uptake. The model (shown in Figure 1) theorizes how our three identified barriers for PrEP uptake interact with each other to form a cascade. YMSM in the United Kingdom must first perceive PrEP to be necessary, have the requisite knowledge about it, and finally feel comfortable acquiring PrEP from a medical setting to eventually obtain PrEP. At each barrier, a proportion of YMSM will be prevented from taking PrEP, and therefore, the number of YMSM will decrease as one moves down the model cascade. However, each step does not occur independently, and certain steps may interact to reinforce barriers. Represented in pathway 1 not having the requisite knowledge about PrEP can impact how necessary individuals perceive PrEP to be. Represented in pathway 2 how inconvenient YMSM perceive acquiring PrEP to be could also potentially influence individuals to alter their thinking in terms of perceived necessity.
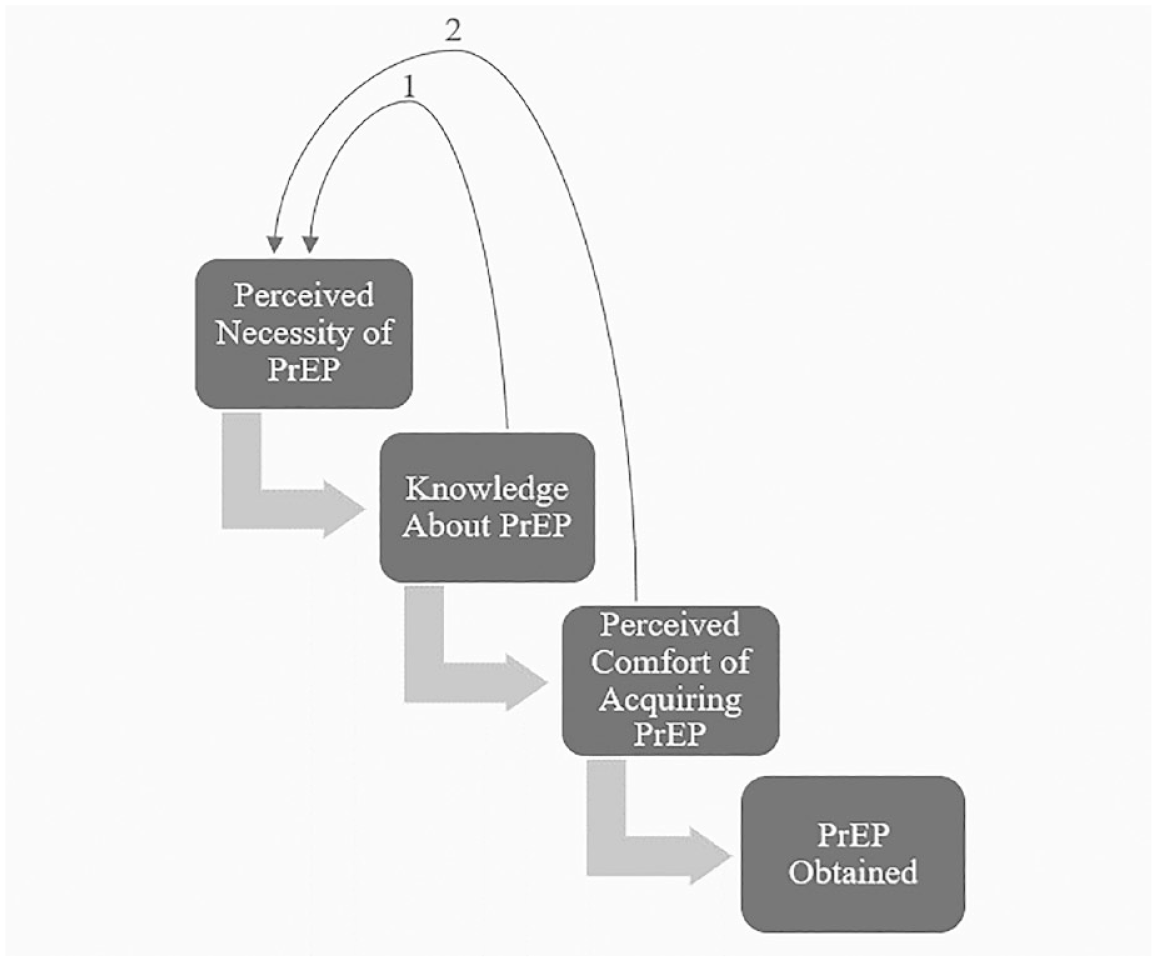
A Cascade Model Showing How the Identified Barriers to PrEP Uptake May Interact
Discussion
This study’s primary research question was, “What are the principal barriers to PrEP uptake experienced by YMSM living in the United Kingdom?” In considering this question, recommendations for both interventions and future research avenues are made. Three barriers were identified: perceived necessity to take PrEP, knowledge about PrEP, and perceived comfort of acquiring PrEP. Many from our sample of YMSM decided not to take PrEP due to feeling it unnecessary for their current situation, and this was often due to their narrower conceptualization of its effects. Several participants misperceived that there were no unique advantages to PrEP uptake, and those who did perceive there to be advantages, solely perceived these to be physical advantages associated with condomless sex. In Harrington et al.’s (2020) study, PrEP users expressed that condomless sex facilitated by PrEP reduced anxiety surrounding HIV contraction and increased intimacy with partners. No participants in our study communicated either of these benefits, suggesting that the necessity of PrEP was restricted more so by a narrow conceptualization of PrEP’s benefits. Being exposed to accounts of PrEP consumption from PrEP users, like those in Harrington et al. (2020), may help expand YMSM’s conceptualization of PrEP’s benefits and, therefore, necessity.
In our study, the perceived necessity of PrEP was also affected by beliefs surrounding PrEP’s inappropriateness, due to situational factors, such as being in a relationship and the utilization of other forms of protection. While certain necessity-limiting factors, such as condom use, produce better general sexual health compared to PrEP use alone, other alleged necessity-limiting factors that were discussed by participants, such as serosorting, increase the risk of HIV contraction (Fernández-Dávila et al., 2011). Young adults are more likely to have sexual relationships with people that they already know compared to older adults (Bradshaw et al., 2010), and as such, serosorting may be particularly popular within YMSM communities. However, despite feeling they can trust a partner’s health status in this regard, risks associated with potential infidelity still exist, false or misguided declarations (Denes & Speer, 2018). These approaches and attitudes must be acknowledged and challenged to reduce HIV transmission in the YMSM community. Even unprotected sex solely in committed relationships may increase the risk of HIV contraction enough to warrant PrEP consumption. A study by Sullivan et al. (2009) estimates that about 68% of new HIV infections come from a main sexual partner, a large proportion of which are partners in seemingly monogamous relationships. Therefore, while being in a monogamous relationship reduced participants’ perceived necessity to take PrEP, infidelity may increase the risk of HIV infection significantly enough to warrant PrEP consumption in this community. To eradicate these damaging misconceptions and to increase the perceived necessity of PrEP, YMSM must be provided with clear and accurate information on PrEP, HIV, and other contraceptive methods.
YMSM in our sample often lacked the requisite knowledge to acquire PrEP. Those who did have such knowledge had gained it from specialist, medical and LGBT+ websites. Thus, YMSM not actively involved in the LGBT+ community, or not openly gay, may be less likely to obtain PrEP-related information from these specific sources. It is also interesting to consider the level of knowledge of the HIV crisis in today’s YMSM community. As noted above, HIV no longer poses a serious risk to life in the United Kingdom. It may be that a lack of experience or knowledge in this area is why YMSM feel PrEP may be less applicable to their health management. Furthermore, YMSM with low levels of health literacy may struggle to comprehend PrEP-related information on medical websites. This is particularly damaging, as YMSM with low levels of health literacy are more likely to be of a low socioeconomic status and are statistically more likely to contract HIV (Gayles et al., 2016). Making PrEP part of the compulsory sexual education curriculum could eliminate this barrier, as well as combat shame surrounding conversations about gay sex within institutional settings (LaSala et al., 2016). Furthermore, to combat information inconsistencies and the need to search across multiple locations, which was discussed by our participants, support exists for a central and vetted authority to manage key PrEP information (e.g., via national health service or government strategy).
Feelings of shame partially explain the YMSM’s concerns in this study surrounding judgment in medical settings, for example, anxiety about disclosing one’s sexuality (Mccrone, 2018). Unlike previous studies, PrEP-specific stigmatization was not identified as a principal barrier to uptake here. However, stigmatization was present in shame surrounding participants’ LGBT+ identity, which can still work toward blocking PrEP uptake. This fear of judgment, alongside concerns about appropriate PrEP-specific knowledge from clinicians, may also be exasperated by beliefs clinicians could have some degree of ingrained homophobia. This belief could originate from the HIV crisis, in which many GPs refused to engage in conversations about HIV with their patients (Wao et al., 2016). In line with previous literature around young people’s concerns discussing mental issues with one’s GP (e.g., Morrison, 2014), some YMSM participants here felt uncomfortable obtaining PrEP from a GP, indicating that allowing GPs to prescribe PrEP, as is the plan with the new PrEP funding, may not increase PrEP uptake. Regardless, YMSM also expressed the inconvenience of visiting an STI clinic to obtain PrEP as a sizable barrier to uptake.
Limitations
When discussing applications of this study’s findings, it is important to acknowledge limitations. While this study benefitted from a diverse range of YMSM perspectives (including three non-White and one transgender individual), no Black YMSM were interviewed. Data collection was also influenced by geographical proximity, willingness to volunteer to take part, and the rigid timescale for this project. As such, our findings can only provide a snapshot of detail around PrEP uptake. Research suggests that Black YMSM are significantly less likely to take PrEP than their White counterparts and are also at an increased risk of HIV contraction (Hoyt et al., 2012). Future research needs to include perspectives from this high-risk community. To elicit in-depth conversations, this study required participants to already have some knowledge of PrEP, thus excluding a proportion of YMSM. For those YMSM unaware of PrEP, barriers may be more knowledge-based and less nuanced, as their lack of knowledge may make them less aware of some of the perceived issues associated with obtaining PrEP, such as the potential for judgment from a GP. As such, the sampling approach here only gathered perspectives from those who may have been more engaged in this domain. However, with widespread media coverage and increased funding, PrEP awareness will likely increase. Finally, while this qualitative study provided useful insights, the type of data obtained is not extensive enough to produce a concrete model. Our theoretical model must be quantitatively tested to assess whether removing these barriers increases PrEP uptake and whether the order in which these barriers are removed affects rates of increase. This could be done by examining whether certain vignettes or experimental stimuli aiming to tackle the perceived barriers will affect willingness to take PrEP (i.e., need, knowledge, and access).
Implications
Our findings provide useful insights into potential ways to disseminate information about and educate relevant groups about PrEP, for instance, being exposed to accounts from PrEP users around consumption and benefits beyond condom use only (e.g., further reduction in anxiety surrounding HIV contraction and increased partner intimacy). Furthermore, health information and education (e.g., in schools or via government programs) should consider justifications for PrEP being nonessential due to partner trust and disclosed sexual health status. Training could emphasize the importance of testing and protecting oneself and a partner should anything change (or be misjudged) during intimate relationships. In addition, education programs would do well to ensure they continue to increase awareness of what may count as at-risk behaviors. As noted earlier, making discussions around PrEP part of compulsory sex education in schools could eliminate health literacy barriers in the YMSM community and potentially help combat shame surrounding conversations about gay sex. Combating possible information inconsistencies across multiple sources supports the need for a central authority to manage key PrEP information (e.g., via national strategies). Such approaches would hopefully aid in relevant groups understanding where and how they can access help, support, and obtain a prescription. Comfort in knowing whether a healthcare provider was queer-friendly was discussed here and in previous findings. Programs that encourage acknowledgment of support in this regard, perhaps noted through membership to or completion of associated training, may help evidence appropriate knowledge and help reduce patient concerns.
To overcome the barriers illustrated in our model, we recommend the utilization of a dedicated online application for PrEP. This would ideally be nationally/centrally managed, since associated tests and prescriptions could be accessed by all and delivered uniformly, increasing efficiency and maintaining the quality of care (Zwaanswijk et al., 2011). This application could also facilitate e-consultation processes, potentially diminishing anxieties associated with acquiring PrEP discussed above. Research has already observed that access to at-home HIV testing kits increases the frequency of testing behavior (Katz et al., 2018), suggesting that at-home online PrEP consultations may similarly increase levels of PrEP uptake. The application could also provide useful data on PrEP use, with accurate and comprehensible information in one accessible platform. This may further help tackle certain myths or misinformation. Such an application could also benefit services such as the U.K. NHS financially, as patient information could be obtained via an online form, keeping consultations brief. Research by Now Healthcare Group (2019) suggests that utilizing telehealth applications throughout the NHS could save NHS England up to £7.5 billion annually.
Conclusions
In conclusion, this research provides important initial insights into the principal barriers to PrEP uptake experienced by the at-risk and underresearched YMSM community in the United Kingdom. A key contribution of this work lies in exploring perspectives from this specific geographic location and risk group and in the context of relative recency in PrEP availability to the community. The study highlights some of the unique barriers within this institutionalized context, associated with the national health system and the frequent use of GPs. The key dominant barriers identified (perceived necessity, knowledge, and perceived comfort) exemplify the unique obstacles present when YMSM in the United Kingdom consider acquiring PrEP. With the help of future research, these findings could lead to the implementation of a range of national-level changes, which aim to increase rates of PrEP uptake and reduce rates of HIV transmission.
Supplemental Material
sj-docx-1-prv-10.1177_26320770231199419 – Supplemental material for Barriers to PrEP Uptake in Young U.K. Men Who Have Sex With Men
Supplemental material, sj-docx-1-prv-10.1177_26320770231199419 for Barriers to PrEP Uptake in Young U.K. Men Who Have Sex With Men by Loukas Haggipavlou and Richard J. T. Hamshaw in Journal of Prevention and Health Promotion
Supplemental Material
sj-docx-2-prv-10.1177_26320770231199419 – Supplemental material for Barriers to PrEP Uptake in Young U.K. Men Who Have Sex With Men
Supplemental material, sj-docx-2-prv-10.1177_26320770231199419 for Barriers to PrEP Uptake in Young U.K. Men Who Have Sex With Men by Loukas Haggipavlou and Richard J. T. Hamshaw in Journal of Prevention and Health Promotion
Footnotes
Author Contributions
Both authors are sole contributors to this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Research resources have been made available as supplementary material. Full transcript data cannot be made available due to the vulnerable sample and associated ethical restraints.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.