
Abstract
Background:
Only one article described ankle varus as a typical symptom in the late stage of the intra-articular osteoid osteoma of the calcaneus. And the red-brown color of synovial fluid in the affected joint hasn’t been reported. This report shows a patient with intra-articular osteoid osteoma of the calcaneus who had the 2 above symptoms.
Case presentation:
A 39-year-old man had left ankle pain and the diagnosis was delayed for 20 months. At the late stage, the ankle was gradually varus. In our hospital, the withdrawal of the subtalar joint gave a red-brown synovial fluid. Together with the typical lesion on MRI, the diagnosis of intra-articular osteoid osteoma of the calcaneus was made. An open operation was performed for treatment. In the procedure, the red-brown synovial fluid was exuded. A specimen was harvested for biopsy confirming osteoid osteoma.
Conclusions:
It is still essential that intra-articular calcaneal osteoid osteoma should be considered in patients with prolonged pain and varus of the ankle. The red-brown synovial may be used as a finding for diagnosis.
Introduction
The juxta-articular or intra-articular site of calcaneus osteoid osteoma was considered scarce, 1 and almost all papers related to the disease were case reports. There were only some small case series of osteoid osteomas around the ankle in which the maximal sample of calcaneus osteoid osteoma was 6 cases. 2 Besides swelling, nocturnal pain, and sensitivity to NSAIDs, reports didn’t describe other symptoms of calcaneus juxta-articular or intra-articular osteoid osteoma, even in case series reports or systemic reviews.2,3 There was only a case report in which the ankle varus was considered a symptom in the late stage of intra-articular calcaneus osteoid osteoma. 4 Another symptom that hasn’t been mentioned yet in any report may be the change of synovial fluid color from yellowish to red-brown. In this paper, we report a calcaneal intra-articular osteoid osteoma in which the patient had these 2 symptoms.
Case Presentation
A 39-year-old man presented with a 20-month history of severe nocturnal pain in the left ankle and difficulty walking with no history of trauma. The patient was treated at local hospitals with some pain relief medications such as acetaminophen and NSAIDs. The pain was lessened but recurrent when medicines were stopped. In the sixth month of the disease, after a magnetic resonance imaging (MRI) was performed, the patient was admitted to a hospital with a diagnosis “narrow of the anterior chamber of the ankle”! An arthroscopy was performed to debride the ankle joint but the situation was still unchanged. Four months after the arthroscopy procedure, an aspiration at the tenderness site was made, and the specimens were sent for a tuberculosis test and biopsy with negative results. The second MRI was performed 6 months later, but there was no confirmed diagnosis yet. Besides the severe pain in the ankle at night, the patient revealed the foot was gradually medially deviated, and walking was difficult. Twenty months after the beginning of the disease, the patient came to our hospital. At the admission, the left ankle was in a medium varus position, the left foot was medially deviated along with normal dorsi-plantarflexion, contrary to the right ankle was normal. Swelling and tenderness were located anteroinferior to the left lateral malleolar without redness or high temperature (Figure 1). A new MRI was performed and an intra-articular and typical lesion of osteoid osteoma in the calcaneus was seen in the lateral side and at the anterior rim of the posterior facet of the calcaneus (Figure 2).

The left ankle was medium varus with swelling anteroinferior to the lateral malleolar (arrow).

The MRI of the left ankle. A typical lesion of osteoid osteoma in the calcaneus was seen (arrows) on the lateral side (A) and at the anterior rim of the posterior facet (B).
The subtalar joint was aspirated with a puncture at the place anteroinferior to the lateral malleolar, getting a little fluid in a red-brown color. For treatment, an open procedure was made with a lateral incision going to the subtalar joint. At the opening of the joint, an amount of red-brown synovial fluid was exuded (Figure 3).

Fluid in red-brown color was exuded when the subtalar joint was opened (arrow).
The lesion was removed with a curette and a piece of tissue was sent for microscopic examination. A little bit of synovial fluid was sent for microbiologic analysis. The defect was left without any graft. After the joint was carefully lavaged, the wound was closed. Microscopic pathology confirmed an osteoid osteoma with irregular trabeculae of woven bone rimmed by a single layer of osteoblasts and scattered osteoclasts (Figure 4). The microbiology test gave a negative result. Five months after the operation, the ankle varus disappeared, and the patient has returned to normal activities pain-free (Figure 5). For now, the patient is very happy and consented to the publication of his disease.
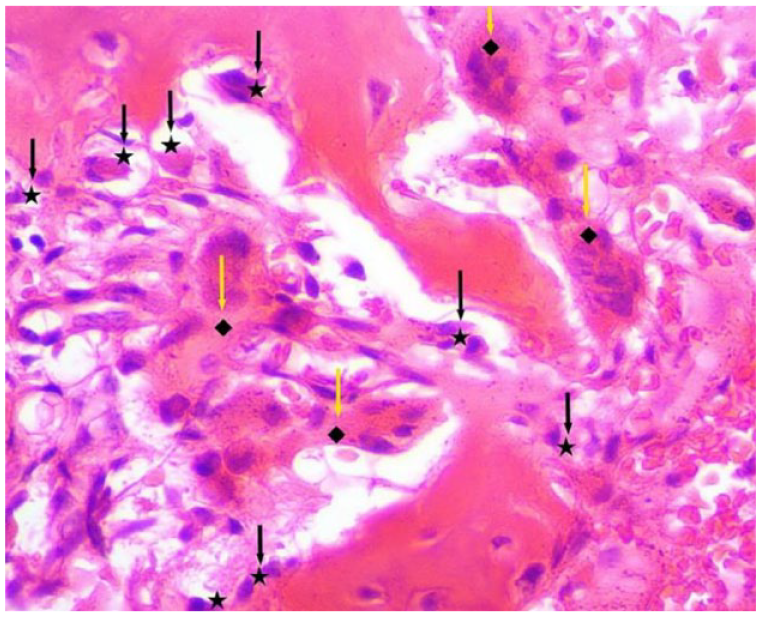
The micropathology image of the lesion. Each trabecula of woven bone was rimmed by a single layer of osteoblasts (black arrows) and scattered osteoclasts (yellow arrows).

Four months after the last operation, the left ankle is normal.
Discussion
Clinically, osteoid osteoma of the calcaneus shows symptoms like any other site. The pain was more intense and nocturnal. The pain can be temporarily resolved with nonsteroid anti-inflammatory drugs. 5
At the onset of the disease, the patient in this report had these signs, but they seem to be vague so local doctors neglected them. Severe pain and difficulty in walking persuaded the patient to go to a larger hospital. There, the symptoms were almost similar to what was classically described in the literature: nocturnal pain, swelling, and localized tenderness at the ankle.4-6 An MRI of the left ankle and some paraclinical tests were made, but none of the proper diagnoses were suggested. The MRI of this patient was made in the 16th month of the disease, but no osteoid osteoma was realized, although it was known that MRI could help diagnose in late-stage. 7 It was thought that unlike in long bone where the characteristic nidus with surrounding sclerosis is seen, in the foot bones, lesions happen in the cancellous bone or intra-articular location and don’t show the periosteal reaction which delays the diagnosis. Commonly, osteoid osteoma of the calcaneus can be misdiagnosed as mono-articular juvenile chronic arthritis, 1 subtalar arthritis,7,8 or subtalar sprain. 9 This patient was misdiagnosed as having a syndrome of “narrowing of the anterior ankle chamber,” an incorrect and strange diagnosis. This strongly suggested that the diagnosis of calcaneus osteoid osteoma was challenging. The ankle varus in calcaneus osteoid osteoma was described in a rare report by Okuda et al. 4 The patient of Okuda came to his institution in the late stage, after 21 months of the disease. Before calcaneus osteoid osteoma was diagnosed, the patient was misdiagnosed as an ankle sprain. Similarly, our patient presented at our hospital after 20 months of disease with a varus ankle and severe pain, also after a misdiagnosis. The ankle varus was in neutral dorsi- and plantarflexion. The cause may be the anterior tibialis and posterior tibialis muscles going into spasm and after a prolonged period of spasticity, the tendons become contracted. We suppose the contraction of the tibialis muscles causes varus because the varus is a pain-release position. The osteoid osteomas of our patient and Okuda’s patient were settled in the same place in the calcaneus. This suggested that the ankle varus is a symptom of calcaneal intra-articular osteoid osteoma in the late stage when the nidus was settled in the lateral side and at the anterior rim of the posterior facet. The management of osteoid osteoma includes open curettage, arthroscopic assisted surgery, or CT/ fluoroscopy guided radiofrequency ablation.6,9-11 However, we perform only an open procedure so that the lesion can be thoroughly curetted and the sample can be sent for microbiological and histopathological confirmation. When the subtalar joint was opened, the synovial fluid was not normally yellowish but red-brown, matching the preoperative withdrawal fluid. On gross examination, osteoid osteoma was brownish red, but no study described the color of synovial fluid in juxta or intra-articular osteoid osteoma. A retrograde review guessed that the osteoid osteoma was brownish-red, and it can impregnate the synovial fluid. In this case, the synovial fluid was sent for a microbiology test, but it was regretted that nothing was done to explain why the fluid was red-brown. Clinically, we think that the red-brown synovial fluid of the affected joint could be a symptom to diagnose intra-articular osteoid osteoma besides other symptoms.
Conclusions
The diagnosis of the osteoid osteoma of the calcaneus is still tricky, and it can be left out. It should be considered an osteoid osteoma if the pain is prolonged combined with ankle varus. This report suggests that the withdrawal of a red-brown fluid might be an additional symptom of intra-articular osteoid osteoma.
Footnotes
Acknowledgements
Not applicable
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Thi Cao: Conceived and designed the analysis, collect the data, write the manuscript and revisions.
Dat Ngo Quoc: Conceived and designed the analysis, contribute data and analysis tools, write the manuscript.
Availability of Supporting Data
Data and materials are available at the corresponding author.
Ethical Approval and Consent to participate
Not applicable.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.