
Abstract

Osteoid osteoma is a benign bone tumor that is characteristically more common in children and young adults and presents with severe pain that worsens at night and decreases with use of nonsteroidal anti-inflammatory drugs (NSAIDs). A characteristic radiological feature is the nidus, a round or oval radiolucent area with surrounding sclerotic bone. 4,12 The tumor commonly occurs in the cortex of the diaphysis or metaphysis of a long bone such as the femur and tibia. The literature contains reports of intra- or juxta-articular osteoid osteoma in the knee, elbow, hip, and ankle joints. 1,3,6,10,11,16,17 Although the traditional surgical route for osteoid osteoma has been open excision of the lesion, less invasive surgeries, such as computed tomography (CT)-guided radiofrequency ablation (RF) and arthroscopic excision, have been reported to have good prognoses, especially for tumors in the intra- or juxta-articular regions. 1,3,6,10,11,16,17
In this case report, we describe a young athlete with juxta-articular osteoid osteoma in the calcaneus, a rare location for this variety of tumor. In this case, excision of the osteoma was performed with subtalar arthroscopy, and the patient was able to achieve early return to athletic activity. This report describes the successful outcome of arthroscopic excision of an osteoma and aims to add to the literature by providing a reference for future athletes and their physicians when considering treatment options in similar cases.
Case Presentation
Written informed consent was obtained from the patient for publication of this case report, including the images. A 17-year-old male athlete who belonged to the soccer club of his high school visited a nearby orthopaedic clinic due to severe left hindfoot pain without history of trauma. Plain radiographs of the left ankle joint revealed no abnormal findings. NSAIDs decreased the left hindfoot pain, but the symptoms persisted and would worsen at night. Six months after the onset of symptoms, he was referred to our institution for further examination and treatment. There was no significant medical or family history. Numerical rating scale assessment revealed a night pain score of 8 out of 10 points. Range of motion in the left ankle joint was restricted (right/left: dorsiflexion, 20°/10°; plantarflexion, 40°/35°; inversion, 30°/20°; and eversion, 10°/5°). Slight swelling and localized heat on the left sinus tarsi were noted. Furthermore, tenderness was reported with the swelling. Blood examination findings were within normal limits. Plain radiographs of the left ankle joint revealed no osseous lesion (Figure 1).

Left ankle joint radiographs. (A) Anteroposterior and (B) lateral views showing no osseous lesion.
T2-weighted magnetic resonance imaging (MRI) showed a low-intensity oval area in the juxta-articular region of the posterior facet, and this lesion was surrounded by a highly enhanced area on gadolinium-enhanced MRI (Figure 2). In addition, the CT scan showed a calcification within an oval radiolucent lesion, which was surrounded by sclerotic bone in the juxta-articular region of the posterior facet (Figure 3).

(A) Sagittal T2-weighted magnetic resonance imaging (MRI) scan showing a low-intensity oval area in the juxta-articular region of the posterior facet (arrow), and (B) gadolinium-enhanced MRI scan showing this area surrounded by a highly enhanced area.

Left ankle joint computed tomography scan. (A) Sagittal and (B) coronal views showing a calcification within an oval radiolucent lesion surrounded by sclerotic bone in the juxta-articular region of the posterior facet at the same region as that seen on magnetic resonance imaging.
Given the patient’s age, medical history, and physical and radiological findings, we strongly suspected this lesion to be a juxta-articular osteoid osteoma in the calcaneus. As such, surgery by means of subtalar arthroscopy was planned. The operation was performed through use of a pneumatic tourniquet (280 mm Hg) with the patient under spinal lumbar anesthesia and placed in the right lateral position. A sinus tarsi portal, which was above the sinus tarsi region, and an anterolateral portal, which was approximately 15 mm anterior to the sinus tarsi portal, were used for subtalar arthroscopic surgery (Figure 4). A 2.7-mm arthroscope with a 30° angle was introduced through the sinus tarsi portal, while a 3.5-mm motorized shaver was introduced through the anterolateral portal. The lateral capsular tissue of the subtalar joint was first resected until the juxta-articular lateral wall of the calcaneus was exposed. Then, the lesion was identified through arthroscopic viewing (Figure 5).

Illustration showing the location of the portals.

Arthroscopic view showing juxta-articular lateral wall of the calcaneus exposed after capsular tissue excision.
The lesion could easily be identified because the joint surface of the lesion was covered with infiltrated, red-colored synovium. In addition, the lateral wall near the lesion was fragile. After identification under arthroscopic viewing, the C-arm was used to confirm that the arthroscope was located at exactly the site of the osteoid osteoma. Then, the lesion was excised by use of a motorized shaver and forceps until normal cancellous bone was exposed (Figure 6). Finally, the curetted floor of the lesion was cauterized with a radio knife (Figure 7).

Arthroscopic view showing excision of the lesion via a motorized shaver.

Arthroscopic view showing the floor of the curetted lesion after cauterization by means of a radio knife.
Histological examination of the surgical specimen showed immature trabeculae with calcification, surrounded by typical osteoblasts and accompanied by vascularization of surrounding tissues. These findings led to a definitive diagnosis of osteoid osteoma (Figure 8).
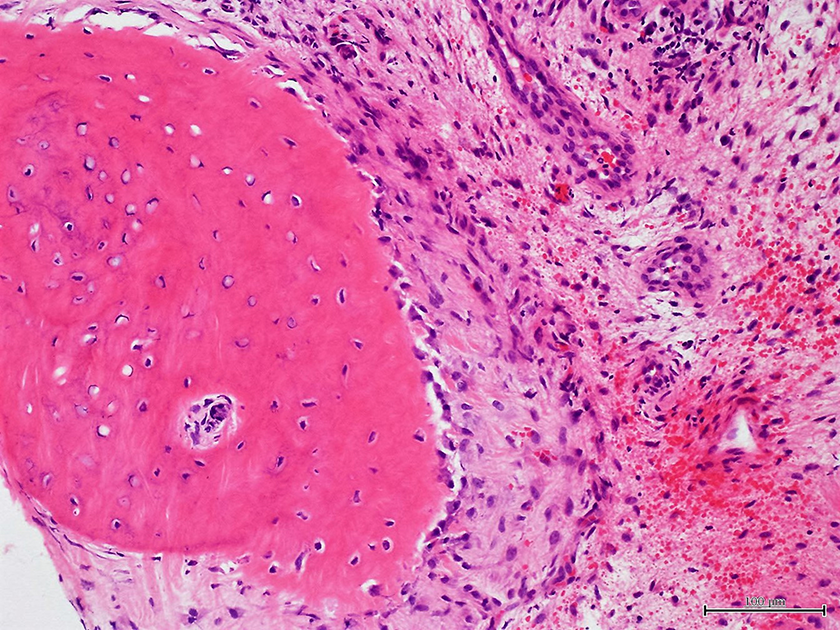
Histological results showing immature trabeculae with calcification, surrounded by typical osteoblasts and accompanied by vascularization of surrounding tissues.
After surgery, no immobilization was used. The patient experienced immediate relief of the severe left hindfoot pain and was able to walk without any support the next day. At 2 weeks after surgery, the swelling and localized heat around the sinus tarsi lesion disappeared and the patient was permitted to start jogging. At 4 weeks after surgery, he was able to resume soccer. At 2 years after surgery, he had no complaints regarding the left foot. At this same point, physical examination revealed no tenderness or restriction of range of motion in the foot and ankle. The patient was a member of the soccer team at his university and enjoyed playing without any symptoms. The Japanese Society for Surgery of the Foot score was improved from 61 points preoperatively to 100 points postoperatively.
Discussion
Osteoid osteoma is a benign bone tumor accounting for approximately 10% of all benign tumors. 4,12 This tumor often arises at the diaphysis or metaphysis of long bones such as the femur and tibia. 4,12 Osteoid osteoma in short bones such as tarsal bones is rare. Its occurrence in the calcaneus has been reported in 2.7% of all osteoid osteomas. 8 Although intra- or juxta-articular osteoid osteoma is not common, cases in the knee, elbow, hip, and ankle joints have been reported. 1,3,6,10,11,15,16 In these reports, some authors suggested that the low incidence may be due to low suspicion for intra- or juxta-articular osteoid osteomas based on clinical features, because patients often report joint pain, restricted joint range of motion, and joint swelling, which mimic the features of arthritis. 1,6,17,19 Furthermore, difficulty in identifying the nidus, which is a characteristic radiographic feature of osteoid osteoma, seems to delay the diagnosis of intra- or juxta-articular osteoid osteoma. 18 In the present case, the symptoms were similar to arthritis and the characteristic radiographic feature of osteoid osteoma was absent, which might have prevented the practitioner who first examined the patient from suspecting intra- or juxta-articular osteoid osteoma. Based on the patient’s age and medical history, as well as physical and radiological findings, we strongly suspected osteoid osteoma and decided to perform surgery.
Several studies have reported surgical treatment for intra- or juxta-articular osteoid osteoma in the calcaneus with good results. 2,7,9,13,15,18,20 Although 4 case reports used traditional open surgery to manage this condition with good surgical results, 2,7,15,18 detecting this small lesion correctly during open surgery sometimes seems to be challenging, and this may cause incomplete excision. Wide, open excision of the lesion performed out of concern for incomplete excision may lead to delayed functional recovery due to the invasive procedure. This may not be favorable for a patient who desires early return to sport, as in the present case. Furthermore, wide excision of an intra- or juxta-articular osteoid osteoma causes injury to the normal joint cartilage and could lead to osteoarthritis of the affected joint in the future.
Instead of open surgery, the recent surgical trend for intra- or juxta-articular osteoid osteoma has been toward less invasive procedures, such as percutaneous RF and arthroscopic surgery. 9,13,20 Migues et al 13 reported on a patient who underwent percutaneous RF under CT guidance for osteoid osteoma in the calcaneus with no evidence of recurrence after 3 years. However, although this procedure is minimally invasive, it entails some problems. Special equipment is needed, such as an operating room equipped with a CT apparatus. Furthermore, it is difficult to obtain an intraoperative tumor specimen, which is necessary for definitive diagnosis of osteoid osteoma on histological examination. In addition, recurrence of symptoms due to incomplete ablation, eventually leading to additional open excision, has been reported with this procedure. 5
Several reports have revealed the effectiveness of arthroscopic surgery for intra- or juxta-articular osteoid osteoma in the hip, knee, and talocrural joints, 1,3,6,10,11,16,17 but to our knowledge, only 2 reports showed good surgical outcomes with subtalar arthroscopic surgery for this condition in the calcaneus. 9,20 Tauheed et al 20 first reported a case of juxta-articular osteoid osteoma in the calcaneus that was treated with subtalar arthroscopic excision with good surgical results. Those investigators noted that one advantage of this procedure is good visualization of the small lesion under the magnification of the arthroscope. However, their report emphasized the surgical procedure, and the clinical course of the patient after surgery was not described in detail. Jurina et al 9 reported the effectiveness of subtalar arthroscopic excision for intra-articular osteoid osteoma in the calcaneus. However, a good surgical outcome was confirmed for only the 8-month period after surgery. In the present case, subtalar arthroscopic excision of a juxta-articular osteoid osteoma made it possible for the patient to return to athletic activity 4 weeks after the surgery, and no recurrent symptoms had been noted at 2 years postsurgically. Thus, this report is the first to describe the clinical course after less invasive arthroscopic surgery for juxta-articular osteoid osteoma of the calcaneus in a young athlete, and it reveals the effectiveness of this surgical technique for achieving early return to athletic activity.
The major limitations of this case report are the lack of generalizability, the potential for overinterpretation, and the retrospective design. 14 Nevertheless, this case report suggests a new treatment option for cases of juxta-articular osteoid osteoma of the calcaneus in young athletes.
Conclusion
This report revealed the effectiveness of less invasive arthroscopic surgery for achieving early return to athletic activity in a young athlete with juxta-articular osteoid osteoma in the calcaneus. Further accumulation of cases and studies with a higher level of evidence are necessary to establish this procedure as the gold standard for intra- or juxta-articular osteoid osteoma in the calcaneus.
Footnotes
Final revision submitted March 11, 2020; accepted March 25, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.