
Abstract
Aim/objective:
Assess agreement between light microscopy and direct immunofluorescence (DIF) for histopathologic evaluation of oral lichen planus (OLP).
Methods:
Records evaluated included 60 OLP, 16 lichenoid mucositis (LM), and 56 non-OLP/non-LM cases. Cases had both light microscopic and DIF evaluations. Histopathologic parameters of OLP included: (1) hydropic degeneration of the basal cell layer, (2) band-like lymphocytic infiltrate immediately subjacent to the epithelium, and (3) presence of Civatte bodies. Two calibrated examiners independently assessed light microscopic features. Examiners reviewed cases with discordant diagnoses to determine a consensus diagnosis. Intra-rater reliability (IRR), sensitivity, specificity, positive, and negative predictive values (PPV and NPV) were determined.
Results:
Of 132 patients, 72.7% were female, average age 61.9 (SD = 13.8). Most common sites were gingiva (37.9%), buccal mucosa (37.1%), and tongue (7.6%). IRR was 0.74 (95% CI: 0.40, 1.00) for the consensus diagnosis and 0.73 (95% CI: 0.39, 1.00) and 0.34 (95% CI: −0.03, 0.72) for the 2 examiners. Comparing consensus and definitive diagnoses: sensitivity of light microscopy: 0.32 (95% CI: 0.20, 0.45); specificity: 0.88 (95% CI: 0.78, 0.94); PPV: 0.68 (95% CI: 0.48, 0.84), and NPV: 0.61 (95% CI: 0.51, 0.70).
Conclusion:
Light microscopy alone is not a viable alternative to adjunctive DIF for diagnosis of OLP lesions.
Introduction
Lichen planus (LP) is an immunologically-mediated chronic inflammatory mucocutaneous disorder. It typically occurs in middle-aged and older patients with a 1.4:1 female to male ratio. 1 Prevalence in the general population is approximately 1% to 2%.2,3 Oral lichen planus (OLP) presents most commonly as reticular or erosive lesions. With involvement of the dorsal tongue, lichen planus appears as a white non-wipeable plaque resembling leukoplakia.
Oral lesions occur most commonly in the absence of skin lesions. Reticular LP is the most common oral presentation of the disease consisting of white non-wipeable Wickham striae. Reticular LP may also present with an annular or lace-like pattern. Erosive LP presents clinically as erythematous or ulcerative lesions with peripheral Wickham striae. It may also present as generalized gingival erythema, clinically appearing as a desquamative gingivitis. 4 Intraorally, the most common sites of involvement include the buccal mucosa, tongue, and gingiva. Both oral and cutaneous lichen planus present as multiple lesions with a bilateral and symmetric distribution.
The clinical differential diagnosis includes oral lichenoid drug reactions (OLDR), oral lichenoid contact lesions (OLCL) as a result of degenerating amalgam restorations or cinnamon, mucous membrane (cicatricial) pemphigoid, pemphigus vulgaris, systemic lupus erythematosus, acute and chronic graft versus host disease (GVHD), leukoplakia, chronic ulcerative stomatitis, lichen sclerosus, and squamous cell carcinoma.5 -7 The diagnosis of classic reticular OLP can often be made based on the clinical appearance of the lesions. Definitive diagnosis of other forms of OLP typically requires histopathologic assessment via routine hematoxylin and eosin light microscopy, often in conjunction with direct immunofluorescence (DIF), in addition to the clinical presentation.
The pathogenesis of OLP is considered to be that of a T-cell-mediated chronic inflammatory disorder of unknown etiology involving destruction of basal keratinocytes via apoptosis. 1 Most of the T-cells noted within the lymphocytic infiltrate involving the superficial lamina propria and adjacent basal epithelium are activated CD8+ cells.8 -12 The co-localization of CD8+ T-cells with apoptotic keratinocytes in the lesions of OLP is highly suggestive of their role in the pathogenesis of this disease.12,13
The concept of malignant transformation of OLP is controversial within the literature.14 -17 The reported annual rate of malignant transformation of OLP is between 0.2% and 0.5%.6,18 When patients are first diagnosed they should initially be monitored at 3 to 6 months intervals. Follow-ups may be performed annually if the disease remains stable and lesions respond appropriately to therapy.
Histopathologic features of OLP include hydropic degeneration of the basal cell layer, Civatte (colloid) body formation, sawtooth-shaped epithelial rete ridges, and a band-like lymphocytic infiltrate immediately subjacent to the epithelium (Figures 1, 2, 3a, and 4a). Variable degrees of hyperkeratosis and epithelial atrophy may also be observed. Differentiating among OLP and other lichenoid lesions with light microscopy may be accomplished by noting the nature of the inflammatory infiltrate, its extent within the deeper lamina propria, and the presence of perivascular infiltrates. However, submission of tissue for DIF is often necessary to obtain a definitive diagnosis to distinguish lichen planus from other lesions that may be included in the differential diagnosis. The most common DIF finding in OLP is the deposition of fibrinogen/fibrin along the basement membrane zone (BMZ), often in conjunction with IgM in association with Civatte bodies (Figures 3b and 4b). Less commonly, C3 may be noted along the BMZ, in addition to IgA in association with Civatte bodies. 19

Oral lichen planus high-power H&E photomicrograph (200×).

Oral lichen planus medium-power H&E photomicrograph (100×).

(a) Oral lichen planus medium-power H&E photomicrograph (100×) and (b) oral lichen planus medium-power DIF photomicrograph (100×) fibrin positive.

(a) Oral lichen planus high-power H&E photomicrograph (200×) and (b) oral lichen planus high-power DIF photomicrograph (200×) fibrin positive.
In our experience from specimens submitted to the UNMC Oral Pathology Biopsy Service, direct immunofluorescence evaluation of suspected OLP lesions has been in more standard use since approximately 2013. Antibodies against IgG, IgM, C3, and fibrinogen/fibrin are commonly utilized for DIF testing. 19 The cost of analyzing a biopsy specimen with DIF is significantly more when compared to light microscopy. This is especially a concern for patients who lack health insurance coverage. The purpose of this study was to evaluate the agreement between light microscopy and direct immunofluorescence in cases having a clinical or working diagnosis of OLP. Our hypothesis was that the light microscopic diagnosis would be in agreement with the DIF results.
Materials and Methods
Records for evaluation included 60 OLP cases, 16 lichenoid mucositis (LM) cases, and 56 non-OLP/non-LM cases from the University of Nebraska Medical Center College of Dentistry (UNMC COD) oral pathology database. Each case came from a unique patient (ie, no patient contributed more than 1 case in this study). Cases were selected from 2013 through 2019, during which time DIF had been in more standard use in conjunction with light microscopy in the diagnosis of OLP. Cases were chosen based on the presence of both light microscopic and DIF evaluations and having a clinical or working diagnosis of OLP, as indicated by the submitting clinician on the biopsy request form. The light microscopic and DIF samples for each case were harvested at the same time. UNMC IRB approval was obtained (IRB #157-20-EP) prior to commencing this study. Written informed consent was waived by the UNMC IRB due to the retrospective nature of the study.
Parameters for the histopathologic diagnosis of OLP were determined based on a hybrid of the proposed criteria as indicated in table IV in Cheng et al. 20 The proposed histopathologic criteria by Cheng et al are based on the original and modified World Health Organization (WHO) diagnostic criteria. Histopathologic parameters included the following 3 criteria: (1) hydropic degeneration of the basal cell layer, (2) band-like lymphocytic infiltrate immediately adjacent to the epithelium, and (3) the presence of Civatte (colloid) bodies.
Two examiners: PG (board-certified oral pathologist) and BH (dental student trained by PG) were calibrated by reviewing a selection of slides prior to commencing the study. Slide numbers were randomly ordered by the statistician and labeled by an individual not directly involved with the study. The slides were independently reviewed and the presence of histopathologic features were reported on an Excel spreadsheet. If all 3 criteria were met, the diagnosis was OLP. If 1 or 2 of the criteria were met, the diagnosis was LM. If none of the criteria were met, the diagnosis was non-OLP/non-LM. Following completion of the individual ratings, examiners reviewed the cases and arrived at a consensus diagnosis for slides with discordant diagnoses. Two weeks after the original review, a subset of 20 random slides, designated by the statistician and labeled by an individual not involved with the study, were relabeled and rated independently to assess intra-rater reliability. A consensus diagnosis was again reached on any discordant diagnoses. Although BH (dental student) was calibrated by PG (board-certified oral pathologist), the aim of the study was not to assess the agreement between examiners, but rather to assess the agreement between light microscopy and DIF.
Statistical Analysis
Descriptive statistics were provided for all variables of interest in this study, as means and standard deviations (SD), or counts and percentages. For both consensus and definitive diagnoses, the diagnosis was dichotomized as either being OLP or not OLP (ie, LM was counted in the not OLP group). For both inter- and intra-rater reliability, overall percent agreement and Cohen’s Kappa statistics with associated 95% confidence intervals (CI) were calculated. Assessment of the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and their associated 95% confidence intervals (95% CI) were calculated for the light microscopy consensus diagnoses, using the DIF results as the conclusive histopathologic diagnoses. In addition, overall accuracy was coded as matched if the 2 diagnoses matched, otherwise they were classified as a mismatch. To see if there were any differences in variables of interest between the match status groups (ie, consensus/DIF diagnoses matched vs mismatched), associations between categorical variables and match status were assessed using Chi-square tests, or Fisher’s exact tests when expected cell counts were low, and a t-test was used to assess differences in age between match status groups. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and clinical characteristics
Of the 132 cases, 72.7% were female and 27.3% were male with an average age of 61.9 years (SD = 13.8 years). For those patients whose race was reported (96/132), 97.9% were White and 2.1% were reported as other. The most common sites of involvement were the gingiva and buccal mucosa, representing 37.9% and 37.1% of the cases, respectively. The next most common sites were the tongue representing 7.6%, lip and vestibule at 5.3% each, palate at 3.8%, and alveolar mucosa representing 3.0% (Table 1).
Demographic and clinical characteristics.

Missing data not reported for 36 patients.
Inter- and intra-rater reliability
The overall agreement between the 2 raters was 81.1%, and the kappa for inter-rater reliability was 0.54 (95% CI: 0.39, 0.69). The overall agreement of consensus diagnoses taken 2 weeks apart was 90%, and the associated kappa was 0.74 (95% CI: 0.40, 1.00). The percent agreement and associated kappa’s for the diagnoses taken 2 weeks apart for the individual raters were 90% (0.73; 95% CI: 0.39, 1.00) for PG (board-certified oral pathologist) and 75% (0.34; 95% CI: −0.03, 0.72) for BH (dental student).
Performance of light microscopy relative to DIF
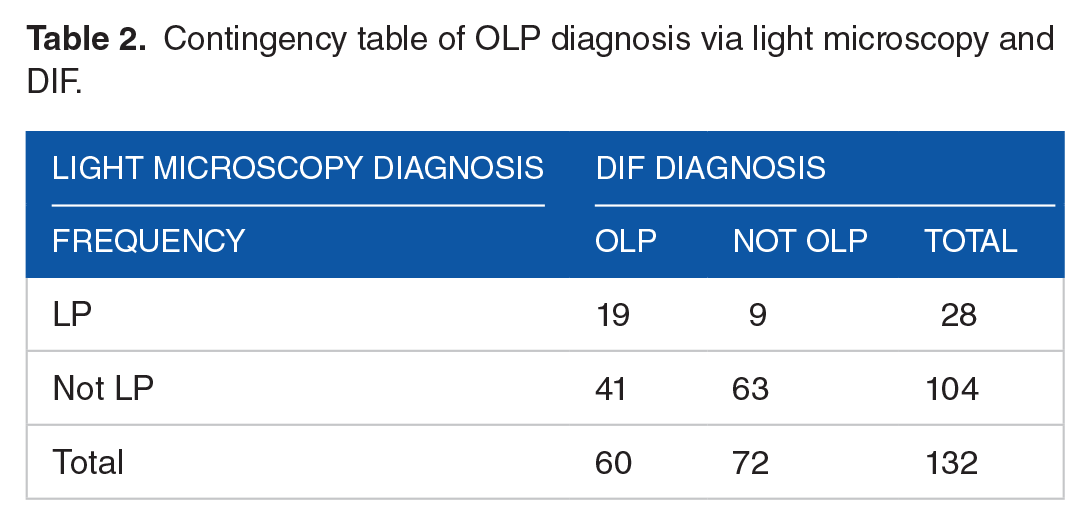
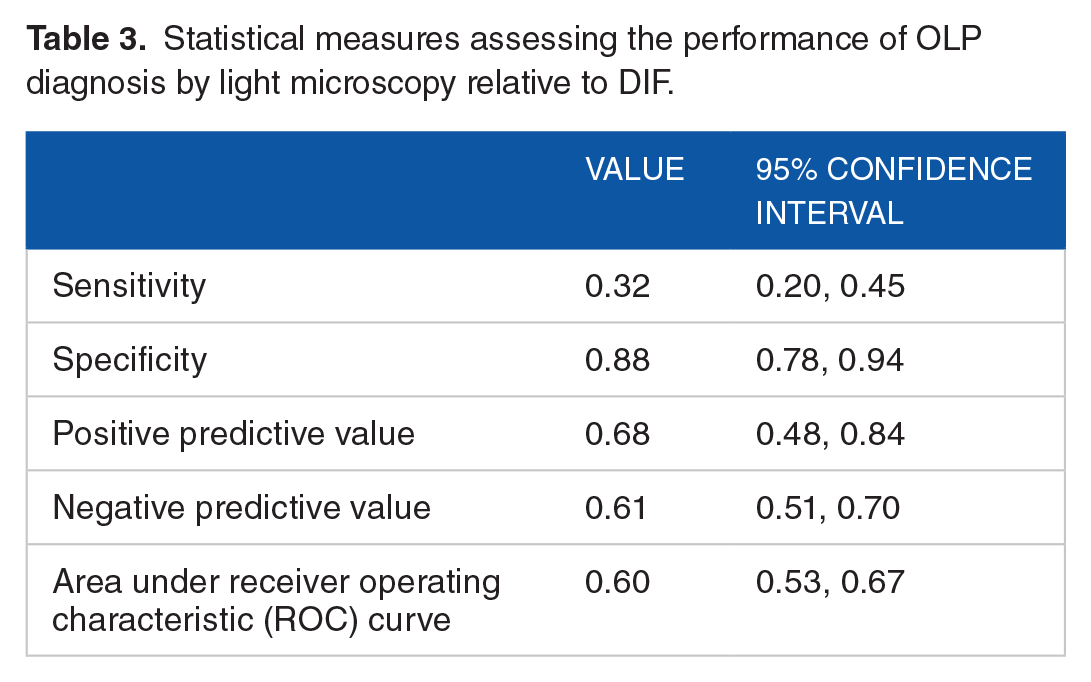
The DIF results were used as the conclusive histopathologic diagnosis when assessing the performance of the light microscopy derived consensus diagnoses. Overall, the consensus light microscopy and DIF diagnoses matched for 82 out of the 132 cases (62.1%). The sensitivity of light microscopy was 0.32, indicating 32% of cases with a definitive DIF diagnosis of OLP had a consensus diagnosis of LP via light microscopy. The specificity of light microscopy was 0.88. Therefore, 88% of cases with a definitive DIF diagnosis of not OLP had a consensus diagnosis of not OLP via light microscopy. The positive predictive value was 0.68, whereby 68% of cases with a consensus diagnosis of OLP had a definitive diagnosis of OLP with DIF. The negative predictive value was 0.61. Therefore, 61% of cases with a consensus diagnosis of not OLP had a definitive diagnosis of not OLP with DIF (Tables 2 and 3). The value of the area under the ROC curve was 0.60.
Contingency table of OLP diagnosis via light microscopy and DIF.
Statistical measures assessing the performance of OLP diagnosis by light microscopy relative to DIF.
To see if mismatches between the light microscopy and DIF diagnoses were associated with demographic or clinical characteristics, we assessed diagnosis match status with those variables of interest. No significant differences were noted between the match and mismatch groups for either age or gender. A significant difference between the match status groups was observed based on lesion location (P = .03). Specifically, the gingiva was the most common location in the match group (45.1%), whereas the buccal mucosa was the most common location in the mismatch group (42%; see Table 4).
Demographic and clinical characteristics by diagnosis match status.

P-value from independent samples test.
P-value from Chi-square test.
P-values from Fisher’s exact tests.
Discussion
Given the more common practice in recent years of the submission of tissue for DIF for the histopathologic diagnosis of OLP, this study assessed whether light microscopy could serve as an acceptable means of arriving at a definitive histopathologic diagnosis for oral lichen planus in the absence of DIF. The goal was to determine the accuracy of light microscopy when compared to the result obtained with DIF. Figures 3a, 3b, 4a, and 4b demonstrate examples where there is strong agreement between light microscopy and DIF. Each of the 132 cases included in the study had a clinical or working diagnosis of OLP as indicated by the submitting clinician on the biopsy request form. Given that OLP presents with periods of exacerbation and remission, for all of the cases included in our study, the light microscopic and DIF samples were harvested simultaneously. The light microscopic diagnosis was rendered by both observers based on a hybrid of the proposed criteria as indicated in table IV in Cheng et al. 20
The sensitivity of light microscopy in comparison to DIF was low (0.32), while the specificity was substantially higher (0.88). The positive and negative predictive values for light microscopy were moderate (0.68 and 0.61, respectively). Intra-rater reliability for the 2 examiners was quite variable, with kappas of 0.73 (PG) and 0.34 (BH). The large difference in intra-rater reliability, along with weak inter-rater reliability are expected given the divergent levels of histopathologic diagnostic experience between the 2 examiners. PG is a board-certified oral pathologist and BH was a dental student. The intra-rater reliability for the pathologist examiner is similar to a previous study regarding the histopathologic assessment of OLP. 21
A potential limitation of this study is that the specimen obtained for light microscopy may not have been a representative sample. This could be an explanation for the low sensitivity of light microscopy compared to DIF. Another possible explanation for the low sensitivity of light microscopy is that the patient may have been using corticosteroids at the time the biopsy was performed. The recommendation is that patients refrain from using corticosteroids for at least 2 weeks prior to obtaining a biopsy specimen. A tissue sample obtained within that 2-week period is likely to exhibit altered histopathology resulting in an inaccurate diagnosis. Another limitation of this study is that BH was a dental student who was calibrated by PG and, thus, the examiners were not independent. However, the primary aim of the study was not to assess agreement between examiners but, rather, to assess whether light microscopy could serve as an acceptable method to diagnose OLP in the absence of DIF. The assessment of inter- and intra-rater reliability was considered to be a secondary aim of the study. Although for those patients whose race was reported (96/132), 97.9% were White, this is typical of the demographics of the midwestern United States. Although oral lichen planus does not demonstrate a racial predilection, 22 we believe that our results demonstrate validity in conjunction with the racial composition of our patient population.
In conclusion, the findings of our study illustrate that light microscopy alone is not sufficient for the histopathologic diagnosis of OLP. This is supported by an area under the ROC curve value of 0.60. DIF in conjunction with light microscopy provides the opportunity to render the most accurate diagnosis in order to provide the most appropriate therapeutic regimen. Given the retrospective nature of our study, we were unable to ascertain the potential effects of corticosteroid use and biopsy site selection on the light microscopic and direct immunofluorescence samples. A prospective study could be designed to account for the above-mentioned variables.
Footnotes
Acknowledgements
We would like to thank Sandi Marlow-Lambert for her clerical assistance with the study and Dr. Dominick DiMaio for contributing the direct immunofluorescence photomicrographic images.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the University of Nebraska Medical Center College of Dentistry Student Research Fellowship FY21-01 and the F. Gene and Rosemary Dixon Endowed Chair in Dentistry (Jeffrey B. Payne, recipient).
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Note
This research was presented as an oral abstract at the 2022 AADOCR/CADR Annual Meeting & Exhibition.
Author Contributions
Blake T. Hansen: Investigation, Visualization, Writing- Original Draft Jeffrey B. Payne: Conceptualization, Methodology, Supervision, Writing - Review and Editing, Funding Acquisition Kaeli K. Samson: Formal Analysis, Validation, Writing - Review and Editing Peter J. Giannini: Conceptualization, Methodology, Supervision, Visualization, Investigation, Writing- Original Draft, Data Curation.