
Abstract
In patients with locally advanced rectal cancer, neoadjuvant radiotherapy or chemoradiotherapy followed by total mesorectal excision as a standard of care. We aimed to explore the number, size, germinal centers, extracapsular invasion of lymph nodes (LN), and their impact on overall survival and disease free survival. Furthermore we also investigated the characteristics of lymph nodes in patients who received neoadjuvant therapy and those who underwent surgery between 2011 and 2018. The count and measurement of lymph nodes was assessed by careful visual inspection and manual palpation. The predictive cut-off value of the lymph node ratio (LNR) was determined based on the receiver operating characteristic (ROC), method and the survival outcomes based on Kaplan-Meier curves. We found that the size and the number of lymph nodes decreased significantly after neoadjuvant treatment. The mean LN for patients who received neoadjuvant therapy was 12.68 ± 6.69 and for patients who did not receive neoadjuvant therapy was 16.29 ± 5.61 (P = .012). The average size for patients who received neoadjuvant therapy followed by surgery was 3.30 ± 1.10 versus 4.22 ± 1.18 mm for control group (surgery only) (P < .001), an LNR of 0.13 (sensitivity: 86%, specificity: 47%, AUC: 60%, 95% CI, 0.41%-0.76%) predicted recurrence and metastasis. Presence of lymph nodes with germinal centers was significantly associated with absence of vascular invasion, nodal tumor deposits, distant metastasis, and lower age group (<50 years). However there was no association seen between overall survival and relapse free, total number of lymph nodes enlarged and extracapsular invasion in positive nodes.
Finally there is no association between lymph nodes with germinal centers and tumor response after neoadjuvant treatment in locally advanced rectal cancer.
Introduction
Rectal cancer (RC) occupies an important place in the prevalence and incidence of gastrointestinal tract cancers. 1 The management of patients with locally advanced rectal cancer (LARC) has improved in the last decade with neadjuvant traitement including chemotherapy and radiotherapy followed by total mesorectal excision. Nevertheless the rate of local recurrence is still around 5% and the risk of metastatic recurrence which is about 30%. 2 In particular, neoadjuvant chemoradiation therapy (nCRT) has significantly decreased local recurrence but with no significant improvements in survival. 3 The status of lymph nodes (LNs) in LARC is considered a critical prognostic factor in its current treatment. 4 In addition, metastatic status of LN predicts survival outcomes in patients with colorectal cancer and is widely used for prognostic stratification.5,6 According to the American Joint Committee on Cancer (AJCC eighth edition), 12 LNs are required to identify regional metastatic LNs to avoid underestimation of staging and false negative reporting of lymph node involvement due to insufficient sampling.7,8 Importantly, many factors can significantly influence LN dissection from rectal resections including characteristics of patients such as sex, age and body mass index, tumor characteristics (anatomical site, histological type, and grade), surgeon skills, and nCRT. 7
Lymph Node Ratio (LNR) has been considered as a method of prognosis prediction in stage III colorectal (CRC) patients. 9 The precision of LNR as prognostic was proven in several studies in addition to the AJCC/UICC N grade.9,10
The impact of nCRT on LN status and survival is still controversial in LARC. Few studies have investigated the effects of nCRT on LN characteristics including their size and number as well as associated histological changes.
The germinal center (GC) is a T-dependent antibody response in which plasma cells secrete high affinity antibodies and memory B cells are formed. 11
In addition to LN status, extracapsular LN invasion (ECLNI) is another factor that has recently emerged and may predict outcomes in various solid cancers.12,13 ECLNI is defined as a mass of invasive cancer cells that exceed the LN capsule into the surrounding perinodal fatty tissue and was not considered until now by the TNM classification for a detailed classification. 14
In this perspective, our study aimed to, compare the number and size of LNs collected from LARC patients who received nCRT or preoperative radiation therapy alone to the number and size of LNs recovered from a group who didn’t receive any neoadjuvant treatment, to establish the effectiveness, as well as the prognostic value, of LNR in predicting survival outcome of RC patients undergoing neoadjuvant therapy. We also focus on the prognostic value of ECLNI and the effects of nCRT on the number of germinal centers evaluated on the LNs and their association with survival outcomes for the first time in a Moroccan population.
Patients and Methods
We enrolled in this study 149 patients with rectal adenocarcinoma diagnosed in the pathology department from January 2011 to October 2018 at HASSAN II University Center.
Patients underwent long-course radiotherapy (45 Gy in 5 weeks) associated with concomitant chemotherapy (5-fluorouracil in continuous infusion), or exclusive radiotherapy (39 Gy/3 fractions), followed by anterior resection or abdominoperineal excision indicated when the tumor involved the anal sphincter.
Data registered included demographic details, neoadjuvant treatment details, type and results of surgery, pathology reports, in addition to cancer outcome (local recurrence, metastasis, and survival).
As a control group, we followed the same procedure on 21 additional patients who did not receive neoadjuvant treatment and underwent only surgery.
Ethics statements
The local ethics committee of the Faculty of Medicine and Pharmacy of Fez and Hassan II University Hospital approved the study protocol under reference number 26/1; and carried out in accordance with the ethical standards of the Declaration of Helsinki. Informed consents were also obtained from all patients.
Macroscopic and histological evaluation
After neoadjuvant treatment, all samples were sent to the department of pathology fresh or fixed in 10% formalin.
The gross examination was performed by a senior pathologist specialized in digestive pathology. Before cutting, the mesorectum was inked to assess the circumferential margin. After fixation, residual tumor and lymph nodes were totally included. 15 Rectal carcinomas were classified according to the eighth edition of the tumor node metastasis classification system. Histological types were limited to adenocarcinoma, mucinous adenocarcinoma, and signet ring cell carcinoma.
The patients were divided into 2 groups according to tumor regression: responders group corresponding to complete and nearly complete regression (Dworak et al 16 3 and 4), and non-responders corresponding to moderate, minimal, and no regression (Dworak 0, 1, and 2). In addition, we examined tumors for vascular, perineural invasions, circumferential resection margin, and lymph node metastasis.
Procedure for counting and measurement of lymph nodes
Lymph node dissection was carefully performed by palpation of the mesorectum to ensure that as many lymph nodes as possible were taken. After examination each LN was dissected with the largest diameters, and placed in a cassette. Specimens were fixed (formalin 10%) and finely cut to secure a microscopic section after paraffin blocs. Hematoxylin-eosin staining was used to analyze the status of the lymph nodes involved. The largest axis of each retrieved LN was measured macroscopically in glass slides, and the total number was counted.
Lymph Node Ratio (LNR) was defined as the ratio between the number of positive lymph nodes and the number of total lymph nodes examined. 9 In addition, we examined LN for number of germinal centers and capsular invasion for positive LNs.
Statistical analysis
The Chi- square or Fisher test statistic was calculated for categorical variables, and the student t-test was used to compare quantitative variables. The correlation between the number of LN and germinal centers was calculated using the spearman test. The receiver operating characteristic curve (ROC) analysis was used to determine, in continuous variables, such as LNR, the value corresponding with the highest accuracy to predict the outcome. The relapse-free survival time (RFS) and overall survival time (OS) were calculated using the Kaplan-Meier method. A P value <.05 was considered statistically significant. For all statistical analysis, we used SPSS 21 (Statistical Package for social sciences).
Results
Demographic characteristics
One hundred forty-nine patient’s data were available for analysis. (Table 1) summarizes the clinicopathological features of the patient database. The average age was 56.38 years and ranged between 22 and 88 years, 53% were women and 47% were men. The adenocarcinoma was diagnosed in 145 patients (97.3%), and 4 (2.7%) cases as signet ring cell carcinoma. Seventy-three tumors were in the lower third of the rectum, 65 were placed in the middle third, and 11 were in the upper rectum. Forty-seven (31.5%) patients underwent exclusive radiation versus 102 (69.6%) who had received chemoradiotherapy in neoadjuvant treatment.
Clinicopathological characteristics of study population.

⋆not evaluated.
The surgical procedure consisted of 33 (22.1%) abdominoperineal resections and 116 (77.9%) low anterior resections. One hundred forty-one (94.6%) patients achieved complete histopathological resection (R0) and 8 (5.4%) cases had positive status (R+). Additionally, the circumferential resection margins were free of tumors with a minimum distance of greater than or equal to 2 mm. Tumor regression grading showed a complete pathological regression of the primary tumor in 25 (16.8) patients.
Characteristics of lymph nodes
A total number of 1889 were recovered (mean, 12.68 nodes per patient; range, 1-40; median 12) from 149 patients. Forty-seven patients had a total of 156 metastatic LN (mean, 1.05; range, 0-13; median, 0.01), and 102 patients had a total of 1733 negatives LN.
As shown in (Figure 1) the number of metastatic LNs was significantly associated with the total number of dissected LNs (P = .001). The average size of the LN including none-metastatic and metastatic nodes recovered was 3.3 mm (range, 2-20; median, 3.2 mm).
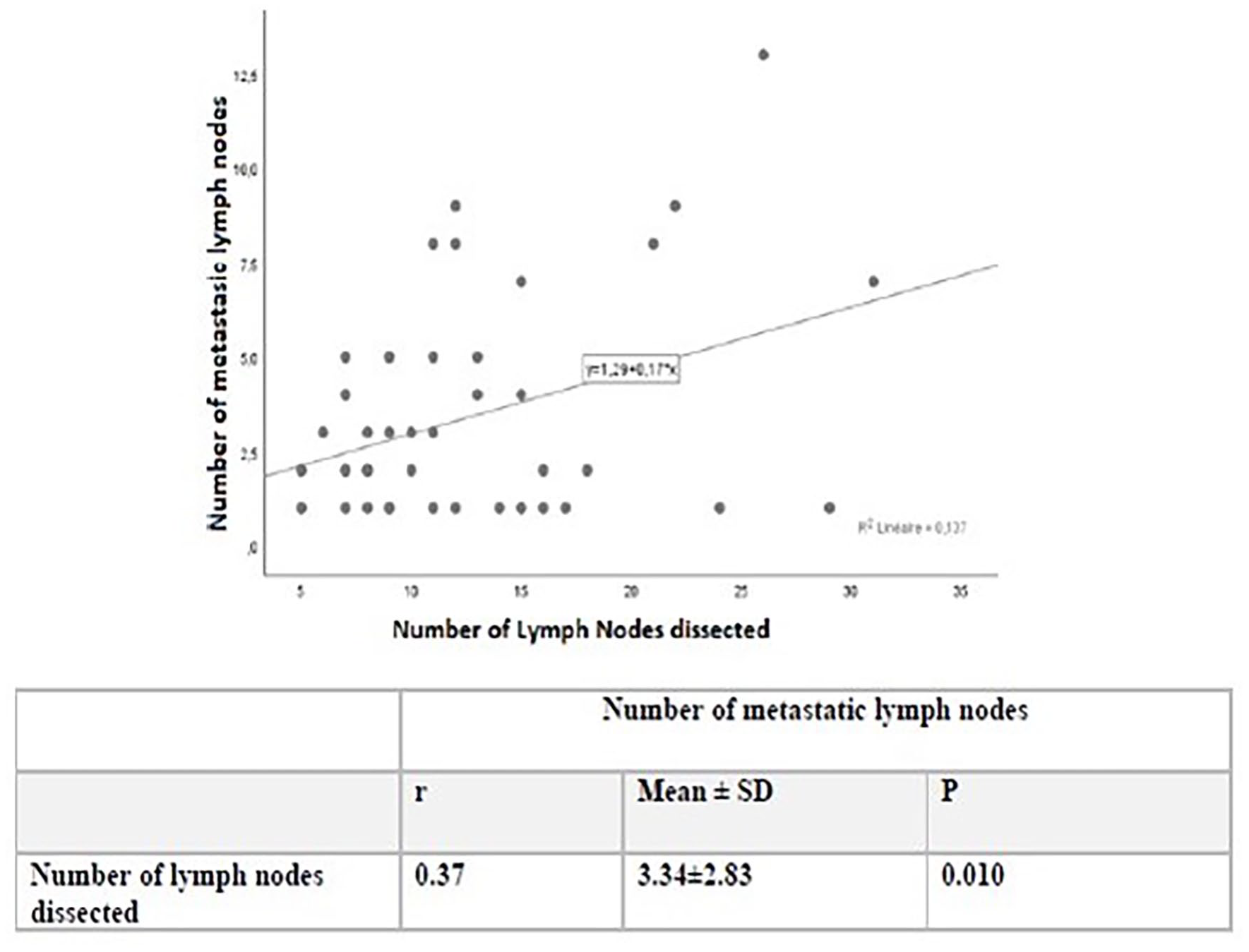
Relation between the number of lymph nodes dissected and the number of metastatic lymph nodes.
The number of 12 LN was achieved in 79 patients (53%) versus 70 patients (47%) with fewer than 12 LN retrieved. Table 1 summarizes the clinicopathological and lymph node characteristics of the patients in the control group. 10.17 LNs were dissected from patients with recurrence versus 12.90 LNs in group without recurrence (P = .015) (Table 2).
Association between clinicopathological characteristics and the number of LN.
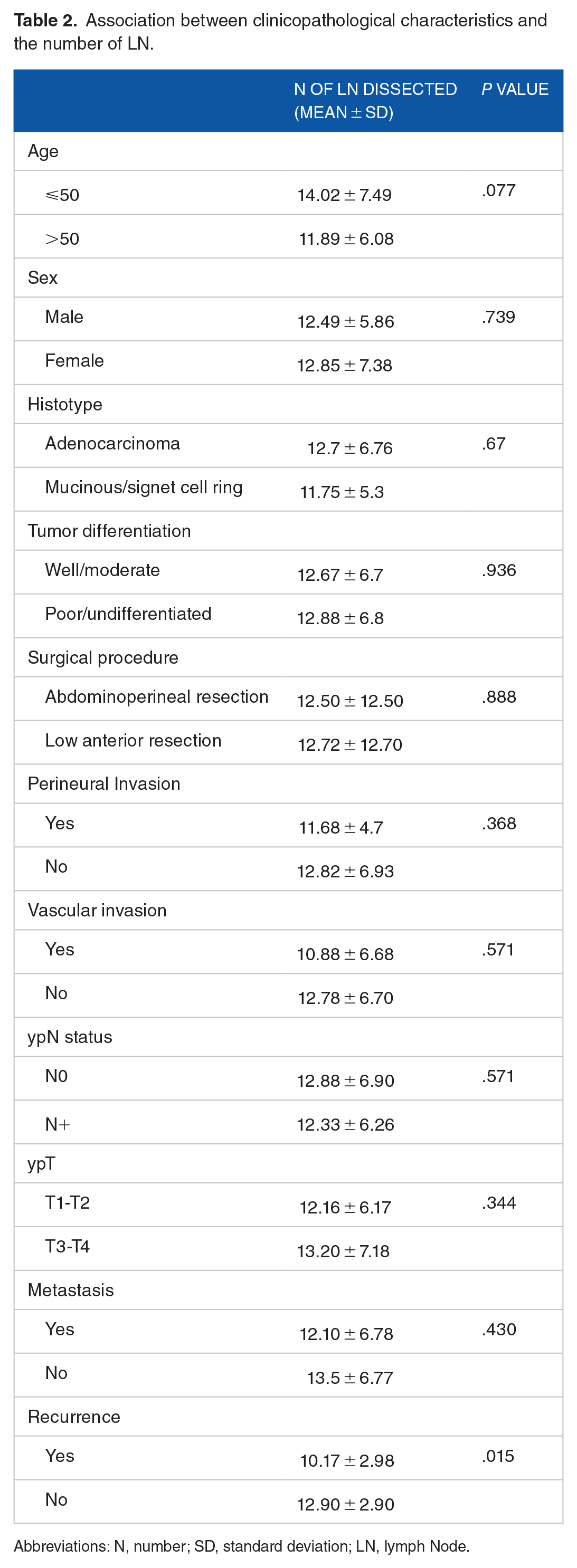
Abbreviations: N, number; SD, standard deviation; LN, lymph Node.
The mean number of LNs examined was 12.68 and 16.29 in the study group and the control group, respectively, which had statistical difference (P = .012) (Table 1).
Furthermore, the mean size of the LNs was 3.30 mm in the study group versus 4.22 mm in the control group (P < .001). In total, 77 (51.7%) patients in the study group and 20 (95.2%) patients in the control group, respectively, has been recovered 12 LNs (P <.001 (Table 1)).
The metastatic LN rate according to LN size comparing patients in study group and control group was illustrated in Figure 2. Both groups had approximately the same rate in LN measuring 2 and 5 mm, while the metastatic rate was 33, 3% in LN measuring 8 mm in the study group versus 0% in the same size of the control group. The curves are almost identical in size under 5 mm, while they are different beyond 5 mm.

Rate of metastatic LN according to LN size comparing patients in study group and control group.
Table 3 summarizes the clinicopathological characteristics of patients who received neoadjuvant chemoradiotherapy and exclusive radiation therapy, 47 patients underwent neoadjuvant exclusive radiation, had an average age of 59.43 years, 102 patients underwent neoadjuvant chemoradiotherapy, had an average age of 54 years. Thirty-three (70.2%) of the patients with exclusive radiotherapy had been retrieved <12 LNs versus 46 (45.1%) of the patients with chemoradiotherapy (P = .005). Additionally, the average number of LNs recovered was significantly increased in patients with RT with 14.74 LNs per patients than in patients with nCRT of 11.73 per patient (P = .017). The number of LN with germinal centers was higher in patients with RT than in patients with nCRT, 8.87 versus 4.79, respectively (P < .001). The metastatic LN ratio was 0.06 in patients with RT and 0.10 in patients with nCRT without significance (P = .13).
Associations between germinatif centers in lymph nodes and clinicopathological characteristics.

Abbreviations: N, number; SD, standard deviation; LN, lymph nodes; GC, germinal centers; RCC, radiochemotherapy; RT, radiothérapy.
Number of germinal centers according to clinicopathological characteristics
Table 4 shows the relationship between clinicopathological factors and the number of retrieved LN. An age of less than 50 years, the absence of vascular invasion, negative LN, and the absence of metastasis were significantly associated with a greater number of LNs with germinal centers (Figure 3).
Univariate analysis for 5-year relapse-free survival (RFS) and overall survival (OS).

Abbreviations: RFS, relapse free survival; OS, overall survival; LN, lymph nodes.

Receiver operating characteristic (ROC) analysis to compare LNR lymph node ratio with survival outcome (cutoff 0.13), AUC 0.60, sensitivity 86%, specificity 47%.
A total of 47 stage III rectal cancers were enrolled in this study. The mean LNR was 0.29 ± 0.20 (range = 0.03-0.75; median = 0.25). The cutoff value assessed to predict patient outcome was LNR = 0.13, with 86% sensitivity and 47% specificity, the area under the curve (AUC) was estimated to be 60% (95% CI, 0.41-0.76%). Two LNR rankings were established according to the cutoff value. The first group of LNR1 < 0.13, and the second group of LNR2 0.13 were identified (Figure 4).

HESx 250: lymph node showing germinal centers.
Relapse-free survival for the LNR groups was 57.9% (HR, 5.24; 95% CI, 47.65%-68.2%), 49% (HR, 6.82; 95% CI, 35.69%-62.43%), (P = .089) for LNR1 and LNR2, respectively (Figure 5a).

Survival function: (a) relapse free survival (RFS) function according to LNR groups and (b) overall survival functions according to LNR groups.
The average OS time for the different LNR groups were 58.2% (HR, 4.3; 95% CI, 49.76%-66.63%), 61.08% (HR, 5.4; 95% CI, 50.38%-71.77%) (P = .27) for LNR1 and LNR2, respectively (Figure 5b).
Follow-up according to the number of LN and ECLNI
The average OS time was 70.49 months with a range of 66.30 to 74.68 months, and 5-years survival was 80% in our series. The average time RFS time was 60.57 months with a range of 54.79 to 66.34 months.
The average OS time was 69.79 months in patients with the number of LNs < 12, and 69.4 months in patients with the number of LN < 12
Univariate survival analysis according to clinicopathological characteristics showed an association between 5-year OS and the absence of positive LN, an ypT stage of T1 and T2, and the absence of vascular invasion (Table 5). RFS was associated with an ypT stage of T1, T2 (Figure 6a).
Multivariate analysis for 5-year overall survival.
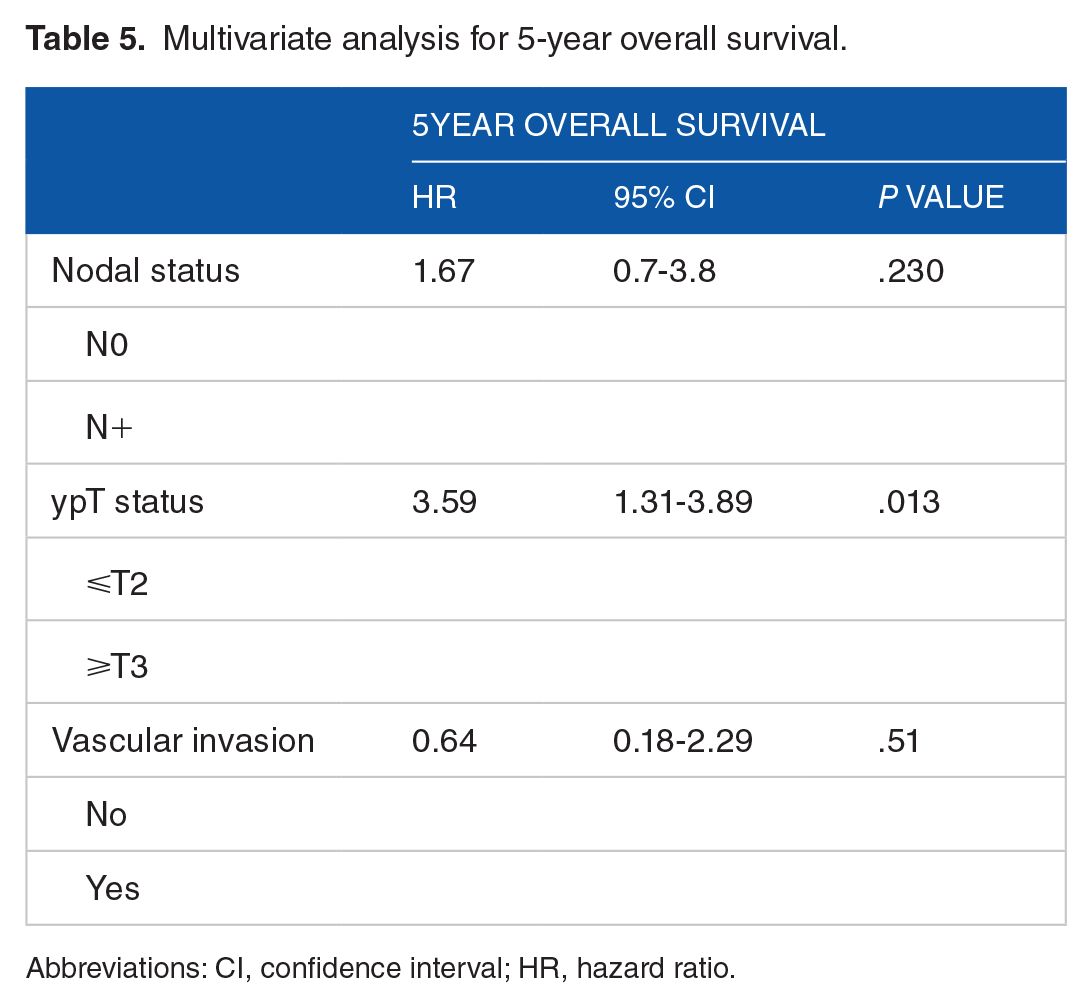
Abbreviations: CI, confidence interval; HR, hazard ratio.

Survival function: (a) overall survival according to number of LNs and (b) RFS according to ECLNI.
The average time of RFS according to ECLNI was 44.58 (25-63) months in patients with metastatic LN and had a positive ECLNI, and 61.27 (48-73) months in patients with metastatic LN did not have an ECLNI (Figure 6b).
Discussion
The important prognostic factor for rectal cancer in patients treated with neoadjuvant treatment is certainly lymph node status. 15 A minimum of 12 lymph nodes should be assessed for the appropriate staging of colorectal cancer, based on data for colon cancer Current guidelines recommendation, and have been extrapolated for use in rectal cancer. 6
In this study, we found that a significant decrease in the number of lymph nodes recovered was associated with neoadjuvant treatment administration, a mean of 12.68 LN was in patients receiving neoadjuvant treatment and 16.29 in those who did not. Miller et al 17 in a previous review concludes that we should anticipate to have a lower lymph node when patients receive neoadjuvant treatment. In fact, 12 or more nodes were evaluated in 51.7% of the patients with neoadjuvant therapy.
Importantly, however, we found that this increase in the number of lymph nodes did not lead to significant overestimation with patient survival. Globally, an average of 4 fewer nodes were assessable in the group treated with neoadjuvant therapy compared to the control group.
According to this study, we cannot disprove the hypothesis that neoadjuvant therapy decreases the number of lymph nodes in the rectal specimen like the previous review,16,18 although we detected moderately more LN in patients with neoadjuvant therapy than in other investigations.17,19 Govindarajan et al 20 found that the mean number of positive nodes was 1.1 per patient (median, one) in the surgery group and 0.4 (median, one) in the neoadjuvant therapy group. In our series, the mean number of positive nodes was 1.05 in the study group versus 0.95 (95% CI, −0.93 to −1.13; P = .84) in the control group.
Although, there was a considered reduction in the number of negative nodes, while the positives did not show a greater difference, this reflects the effect of neoadjuvant therapy on the downstaging of nodes. The effect of radiation therapy on lymphocyte destruction, stromal fibrosis, and high radiosensitivity of lymphoid tissue may explain the decrease in the number and size of negative lymph nodes, which may make their detection difficult.21,22
Like Gonen and Lu2,23 we demonstrated that the higher the number of positive LNs found, the higher the number of LNs examined.
Gonen et al proposed in a preview study 23 that the T stage can be a factor related to the number of LNs intended to be achieved. In the same study the authors find that 4 nodes can be sufficient to ensure 95% accuracy for nodal status in stage T124,25 and the probability of missing a positive node is present in 29.7% if 5 nodes are examined and drops to 13.6% when 12 nodes are examined. According to this previous suggestion of Gonen et al, we hypothesize that in our series the number of 12 or more nodes has been completed because of an increase in the number of patients with a T3 stage (48.3%). Furthermore, supplement factors related to performing surgical resection and optimal pathologic assessment process can explain the number of LNs assessed in our series, as demonstrated in previous review.23,26,27 In addition, the smaller number of LNs found in patients who received neoadjuvant chemoradiotherapy compared to those received exclusive radiation therapy can be explained by the effect of the total dose of radiation therapy. Rullier et al reported similar findings. 28
Furthermore, the LNs of the study group were significantly smaller than those of the control group.
Clearly, the size and number of lymph nodes are significantly reduced after neoadjuvant therapy, which can be related to the mechanism of apoptosis and involution. 18 The median diameter of the dissected lymph nodes was 3.2 mm and most (51%) were 0.3 cm in size like the previous review.29,30 This will make harvesting nodes difficult, but it seems that careful visual inspection and dissection by a dedicated pathologist can still uncover substantial numbers. Most metastatic lymph nodes, in the study and the control groups, were <5 mm in size. Similar in our study, previous study 28 demonstrates that most metastases LNs in colorectal cancer are found in lymph nodes diameter less than 5 mm. Metastatic LNs were larger than non-metastatic ones. The smaller size of the negative lymph nodes is probably caused by rapid apoptosis of lymphocytes in contrast to tumor cells. 30 For better prognosis, calculating LNR has been adopted as an alternative method, resulting from numerous difficulties related to lymph node retrieved.
Several studies had shown that patients with a tumor presented a higher immune reaction of this type had fewer tumor emboli (vascular, lymphatic, and peri-nerval) and had a lower incidence of recurrence, 31 our study confirmed, on the simple histological appearance of GC in LN, that the presence of more germinal centers in LN is correlated with the absence of vascular invasion, younger age, negative LN, and absence of metastasis.
Zhaomin et al found that the 5-year OS for LNY less than 12 and 12 or more in the neoadjuvant group were 72.6% and 78.2%, respectively, in our current study, we found that 70% of patients with LNY less than 12 had a 5-year OS of 79% and those with 12 or more had a 5-year OS of 81%, without significance association. Another study in the New York Cancer Center also showed that the number of nodes was not significantly associated with OS (HR, 0.99; 95% CI, 0.96-1.01).32,33 In the contrary, Lykke et al found that an LNY of at least 12 was independently associated with improved 5-year OS irrespective of neoadjuvant treatment.
Our study demonstrates that LNs retrieved is associated with neoadjuvant treatment. The number of lymph node yield decreased in the surgical specimen after preoperative therapy. 16 Fibrosis in lymph nodes and immune response exposed to radiation therapy represent the main factors related to the reduction of the number of nodes after neoadjuvant therapy, which results in difficult identification of nodes in the specimen. 31
Conclusions
In conclusion, our study reveals that pathologist vigilance and performance, as well as surgeon accuracy, remain the key to successful nodal staging and sufficient lymph node recovery after neoadjuvant treatment. Furthermore, we revealed that preoperative treatment significantly decreases the number of LNs yield than surgery procedure alone. Furthermore, we demonstrated that the size of recovered lymph nodes decreased significantly after neoadjuvant treatment.
The cutoff value of LNR = 0.13 in rectal cancer patients of stage III is the predictive threshold value of relapse in our series. Through the result of our trials, we observed an inter-relationship between a high number of germinal centers present in LN and an absence of vascular invasion, younger age, negative LN, and absence of metastasis.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.