
Abstract
Hepatoid adenocarcinoma is a rare type of extrahepatic adenocarcinoma with glandular and hepatocyte differenciation. The tumor can occur in many organs, generally in the stomach, the location of the lung being extremely rare. Despite poor prognosis and few effective treatment options, a timely and accurate histopathological diagnosis is key to optimal clinical management for long-term survival. Given the few reports published to characterized hepatoid adenocarcinoma, the emergence of any new case will contribute to improve understanding of the disease. Very few reports have been published to characterize hepatoid adenocarcinoma cytologically or even histologically. The aim of this work is to focus on the anatomoclinical characteristics of this rare entity. We present a retrospective study of 2 cases of pulmonary hepatoid adenocarcinoma confirmed by histological and immunohistochemical study.
Background
Hepatoid adenocarcinoma (HAL) is a rare entity, occurring mainly in the gastrointestinal tract, the lung accounts for approximately only 5% of all hepatoid adenocarcinoma reported. Due to its non-specific symptoms, HAL diagnostic is based on histopathological and immunohistochemical findings. Spotting cancer early increases the chances of survival, which remain gloomy because of the delayed diagnosis at advanced stages of the disease.
Case Report
Our first patient was a 70-year-old man with a 37-pack-year smoking history who was referred for evaluation of a suspicious lung nodule. CT scan revealed a lung mass in the upper lobe measuring 5 cm. CT-guided biopsy was made and showed large infiltration by a carcinomatous process with trabecular architecture. Cancers cells were large and showed atypical cytonuclear nuclei with large foci of tumor necrosis (Figure 1).

First case: Infiltration by a carcinomatous process with trabecular architecture with large cancers cells and atypical cytonuclear nuclei (hematoxylin and eosin stain X20).
Immunohistochemical study showed a positive stain for hepatocyte antibody and granular cytoplasmic stain for TTF1 (Figure 2). It was negative for CK7 and CK20 antibodies (Figure 3).
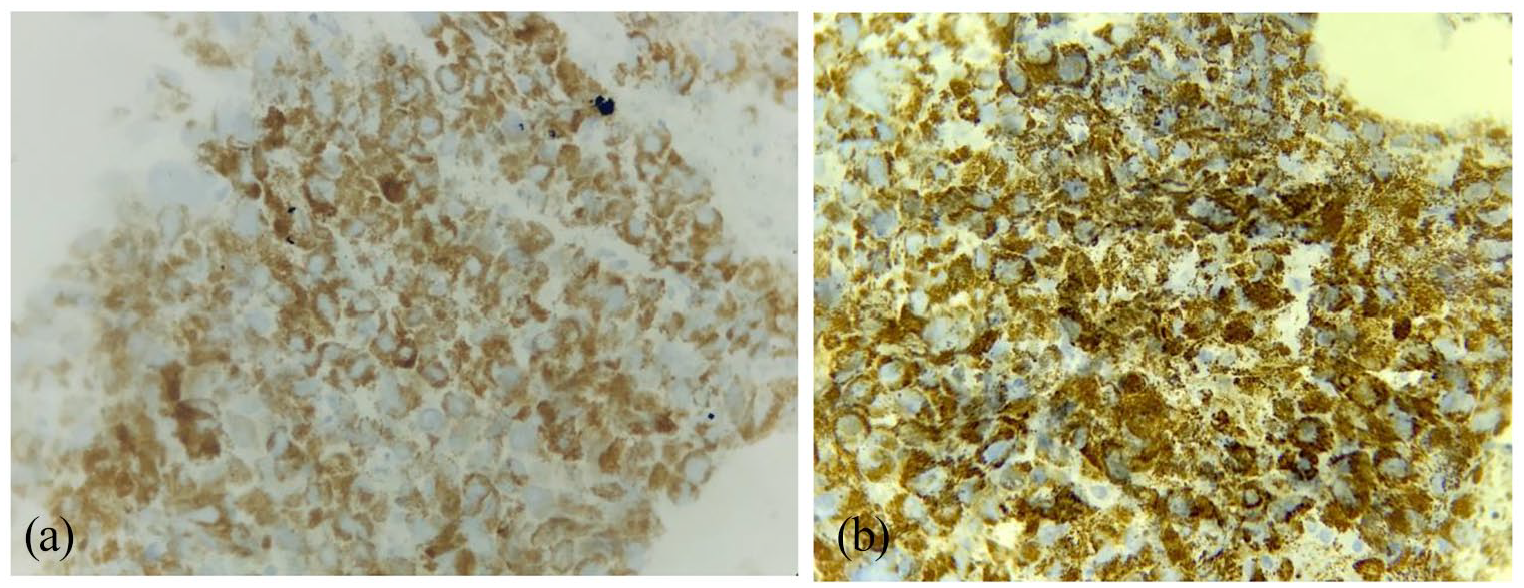
First case: positive granular cytoplasmic staining with TTF1 (a) and hepatocyte (b).
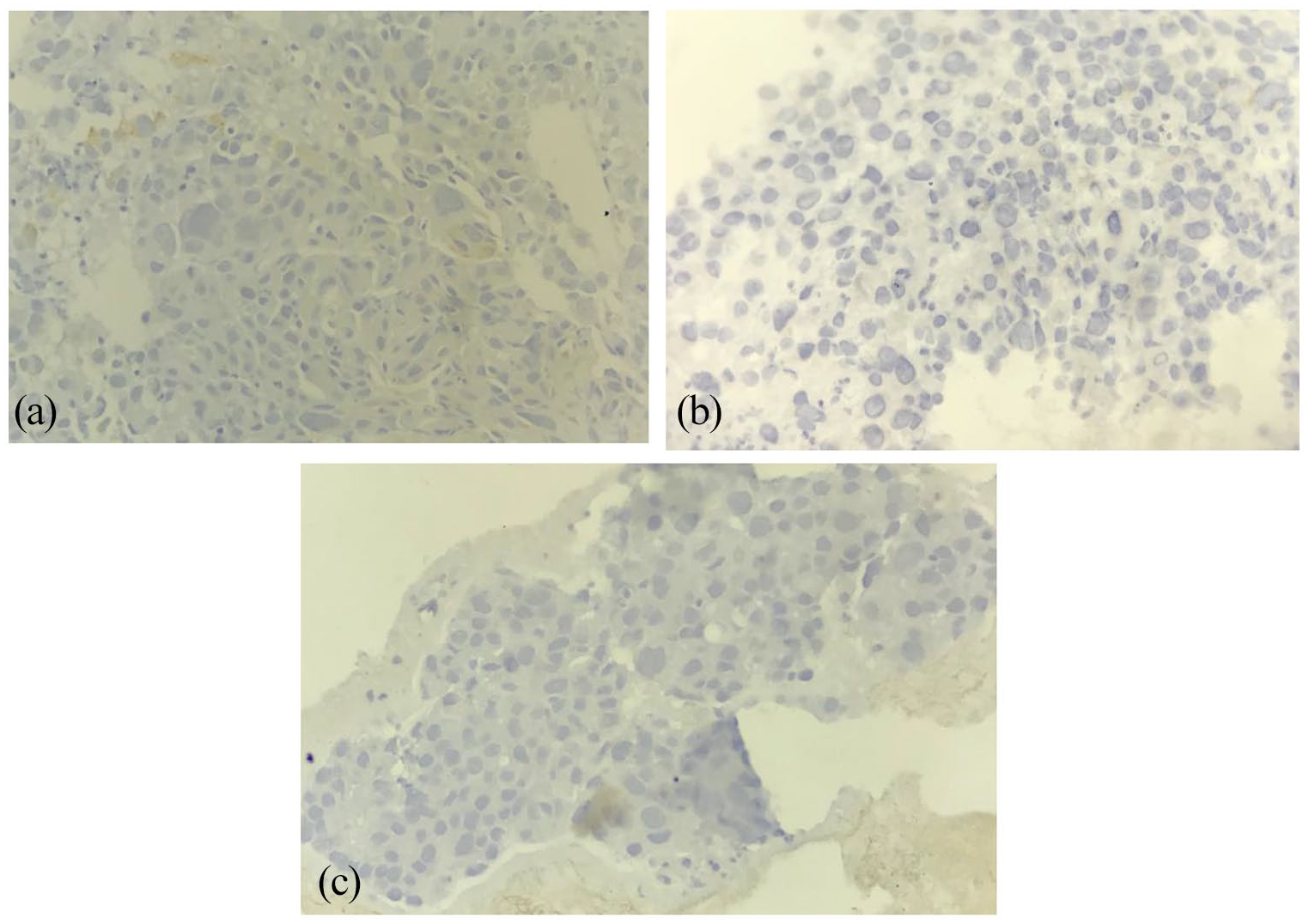
First case: negative staining with CK 7 (a), CK 20 (b), and p40 (c).
In the absence of a liver mass on imaging, the histological and immunohistochemical features of staining confirmed hepatoid adenocarcinoma of the lung.
The second patient was a 70-year-old man, old smoking, with a tuberculosis history. He was referred for evaluation of a right pulmonary apical process with invasion of the hilum.
Percutaneous biopsy respond to lung tissue infiltrated by an adenocarcinoma of acinary architecture composed by cylindrical cells, with abundant eosinophilic cytoplasm. The nuclei were anisocaryotic, and strongly nucleated (Figure 4).

Second case: (a) adenocarcinoma of acinary architecture composed by cylindrical cells, with abundant eosinophilic cytoplasm and (b) The nuclei were anisocaryotic, strongly nucleated and hyperchromatic.
The tumor showed positivity for hepatocyte antibody and nuclear and cytoplasmic stain for TTF1. It was negative for p63 antibody (Figure 5).

Second case: positive staining with TTF1 (a) and hepatocyte (b) and negative with p63 (c).
AFP dosage in both patients was negative, 6 ng/ml for the first patient, and 8 ng/ml for the second one.
The 2 patients underwent surgical resection ant were referred then to an oncology center for further management.
Discussion
Hepatoid adenocarcinoma is a rare and aggressive extrahepatic cancer characterized by morphological and functional similarities with hepatocellular carcinoma (CHC).
It usually originates in the gastrointestinal tract, the stomach being the organ most commonly affected (63%), but mat affect other organs like ovary (10%), lung (5%), uterus (4%), pancreas (4%), or bladder (4%). 1
In fact, HAL is an extremely rare localization with only 36 cases described on the electronic PUBMED database between January 1990 and February 2020.
Pathophysiologically, lung, liver and stomach all derive from the forget. Therefore, HAL may be caused by changes in differentiation, adenocarcinoma cells from the lung, differentiate into liver cells. 2
This tumor occurs mostly in middle-aged and elderly patients over 50 years old, with clear male predominance (92%) and chronic smokers. 3
Because of nonspecific clinical manifestations, the diagnosis is often made at an advanced stage of the disease (stage III or IV) leading to poor outcomes. In fact, this tumor is characterized by an aggressive clinical course, average life expectancy being between 7 months and 7 years in patients undergoing surgery, and 1 year survival rate of 55%. 4
Due to its wide-ranging presentations form, diagnostic and treatment are difficult.
Diagnostic criteria included high level of the alpha foeto protein (AFP), but it was demonstrated that this is not specific for HAL. 5
The new diagnostic criteria included that the tumor may only have characteristics of hepatoid adenocarcinoma or present components of typical papillary or acinar adenocarcinoma, sign and ring cells, or neuroendocrine carcinoma. Plus, the tumor most express immunohistochemical markers for hepatic differentiation; the expression of AFP not being required.2,6
However, eliminate hepatic metastasis is mandatory because it is the most common site for extrahepatic metastasis. It may require radiologic, morphologic and immunophenotypic correlation.
Therefore, our cases meet these criteria even if AFP expression is negative, showing histological characteristics of hepatoid adenocarcinoma and positivity for the hepatic cell specific marker.
The diagnosis mainly relies on the morphological characteristic and immunohistochemical specific markers.
Macroscopically, the tumor usually presents a bulky mass, with variable size, mostly more than 5 cm. The cut surface of the gross specimen is gray or gray brown with clear boundaries. 3
Histological examination shows large polygonal cancer cells, with granular eosinophilic or transparent rich cytoplasm, arranged in large sheets. The nuclear is large, centrally placed.
Non-hepatic like differentiation areas can be seen in adenoid and papillary structures.
Immunohistochemical study is paramount to make diagnosis of hepatoid adenocarcinoma and distinguish it from metastatic CHC. 7 Cancer cells show positive stain for primary pulmonary adenocarcinoma (TTF1), and CHC (HepPar1). CK18 is also expressed, CK7 is variably positive, and CK20 is negative.8,9
Due to the extremely low incidence and strong tumor heterogeneity, there is no standard treatment and few effective treatment options. Nodal and distant metastases are common at initial presentation and, as a result, the
Conclusion
HAL is a rare tumor with limited data concerning clinical presentation, management and outcomes. The finding of HAL pathological characteristics is important for the early diagnosis. It closely mimics CHC and can be misdiagnosed by both pathologists and clinicians.
As hepatoid adenocarcinoma is a very aggressive adenocarcinoma variant, an accurate and timely diagnosis is the key of optimal clinical management. Additional studies are needed to develop new treatments for this rare disease.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Kaoutar Znati in the management.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contribution
YL retrieved clinical information, wrote the manuscript and performed the literature review. KZ first identified this case, proposed the study and revised the manuscript for important intellectual content. AJ, FZ and ZB provided valuable insight during manuscript preparation.
Availability of Data and Materials
The raw data are available upon request to the following e-mail address:
Ethics Approval and Consent to Participate
This case report was approved by the Ethics Committee of Faculty of medicine and pharmacy Mohammed V University Rabat.
Additional patient consent for this retrospective study was not required.
Consent for Publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient. A copy of the consent form is available for review by the Editor of this journal.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.