
Abstract
Aim:
We aimed to show the immunohistochemical expression of programmed death ligand 1 (PD-L1) in laryngeal squamous cell carcinomas (SCCs).
Materials and methods:
The study includes 52 laryngeal SCC cases that underwent surgical resection. Immunohistochemical staining of PD-L1 (Clone 22C3) was applied to the sections obtained from paraffin blocks. Combined Positive Score (CPS) was evaluated as described in manuals. Tumor Proportion Score (TPS) was assessed by the percentage of positive tumor cells which were designated as positive if ⩾1% of the tumor cells showed membranous staining.
Results:
There were 35 cases (67.3%) having CPS < 1 and 17 cases (32.7%) having CPS ⩾ 1. There was no relationship between CPS, TPS, and the clinicopathological data.
Conclusion:
Further studies with a large number of advanced-stage cases are needed.
Introduction
Researches in immunology resulted in finding new pathways in carcinogenesis and treatment options targeting tumor response rather than the tumor itself have been developed. Programmed cell death protein-1(PD-1)/programmed death ligand-1 (PD-L1) pathway, which is one of the immune checkpoints for T-cell response, allows the tumor cells to escape from host defense. Programmed cell death protein-1 is expressed on the surface of activated T-cells, B-cells, monocytes, natural killer cells, dendritic cells, and tumor-infiltrating lymphocytes. Programmed cell death protein-1 binds 2 ligands: PD-L1 and PD-L2, members of the B7 family. Programmed cell death protein-1/PD-L1 complex inhibits T-cell activity that has an important role in limiting normal immune response and preventing autoimmunity. Tumor cells may also produce PD-L1, therefore inhibit T-cell response and immune response against the tumor. 1 Physiologically, PD-L1 is expressed in low levels in parenchymal cells such as pancreatic islet cells, hematopoietic and endothelial cells, while highly expressed in tissue macrophages, placenta, liver, lung, and tonsils. Apart from this physiological expression, PD-L1 expression is seen particularly in malignancies such as non-small-cell lung carcinoma (NSCLC), malignant melanoma, renal cell carcinoma, hepatocellular carcinoma, esophageal and pancreatic cancer, and bladder cancer. It is proved that survival is inversely related to PD-L1 expression. 2
Principally, inhibition of PD-1/PD-L1 binding eliminates inhibition of the immune system. Immune checkpoint inhibitors aim to activate the immune system and provide an effective response to the tumor.
Currently, the largest series of immune checkpoint inhibitors have been reported for NSCLCs, transitional epithelial cell carcinomas of the bladder, renal cell carcinomas, and malignant melanomas. Current studies conducted on different tumor types, showed that high PD-L1 expression status is generally associated with poor prognosis and short survival. 2
In recent studies, high PD-L1 expression has been found in head and neck squamous cell carcinomas (HNSCCs). 3 It has been reported that these cases showed poor clinical course, and PD-1/PD-L1 inhibitors might be used as early treatment options.
The number of studies for the evaluation of PD-L1 expression in laryngeal SCCs is limited in English literature. In this study, we aimed to evaluate immunohistochemical PD-L1 expression, both using Combined Positive Score (CPS) and Tumor Proportion Score (TPS), in laryngeal SCC, its relationship with prognosis and clinical data, while comparing our results with the previous publications.
Materials and Methods
The study included 52 laryngeal SCC cases diagnosed between January 2014 and August 2016 that underwent surgical resection. The surgical procedure, stage information, and survival data were retrieved from the Department of Ear Nose Throat database. Fifty-two patients eligible for the following criteria were included in the study: (1) treatment with curative intent, (2) a histological diagnosis of squamous cell carcinoma of the conventional type, excluding cases of spindle cell, verrucous, adenosquamous, basaloid, and undifferentiated SCC; and (3) having no another primary tumor. We obtained written informed consent forms from the patients.
Tissue microarray construction
Haematoxylin–eosin (H&E)-stained slides from tissue blocks had been re-evaluated for tumor type, marked for tissue microarray (TMA) construction. 4 Tissue microarrays (approx. 5 tumors per TMA block) were constructed with 5 tissue cylinders of 2.5-mm diameter per tumor.
Immunohistochemistry
The areas surrounded by inflammatory cell infiltration that best represent the tumor were selected. Immunohistochemical staining was performed using an automatic device (BenchMark XT IHK/ISH Staining Module, Ventana Medical Systems Ins., Medical Systems, Tucson, AZ, USA). Sections were obtained from the 10% paraffin blocks. Deparaffinization was performed using solutions, and they were rehydrated using a series of decreasing alcohol concentrations. Samples were kept in a 10 mmol/L buffered citrate solution for 30 min at 36°C. Afterward, primary PD-L1antibody (1/50 dilution, 30 min incubation, monoclonal mouse anti PD-L1 Clone 22C3, Dako North America, Inc., CA, USA) was applied to the slides. Due to our experience with this antibody and its compatibility with our devices, this brand and clone were chosen among the other commercial antibodies.
Immunohistochemical PD-L1 staining evaluation
The tonsil tissue was used as the control tissue and percentage rates were given. Necrotic areas were excluded from scoring. All slides were read by 2 experienced pathologists, 1 specialized in head & neck (N.C.) and 1 in lung (S.B.).
We evaluated CPS, recently described as a more reliable scoring method (AGILENT DAKO, PD-L1 IHC 22C3 pharmDx Interpretation Manual—HNSCC). Partial or complete linear membrane staining of viable tumor cells is considered as staining and included in the scoring. Any membranous and/or cytoplasmic staining of lymphocytes and macrophages within tumor nests and/or adjacent stroma is considered positive staining and included in the scoring. Combined Positive Score is defined by the number of PD-L1 staining cells (tumor cells, lymphocytes, and macrophages) divided by the total number of viable tumor cells, multiplied by 100. Programmed death ligand-1 expression scores are divided into 2 groups based on a CPS:
CPS < 1: No PD-L1 expression.
CPS ⩾ 1: PD-L1 expression.
Tumor Proportion Score was also evaluated. Tumor cell staining was assessed by the estimated percentage of positive tumor cells, and the samples were designated as “positive” cases if ⩾1% of the tumor cells were stained.
TPS < 1%: No PD-L1 expression.
TPS ⩾ 1%: PD-L1 expression.
Statistical analysis
Descriptive statistics were used to describe the data. Nonparametric data were compared using the chi-square test. The Kaplan-Meier method was used for survival analysis, and the log-rank test (Mantel–Cox) was performed to compare the survival curves between the groups. The confidence intervals were calculated at the 95% confidence level and differences at p < 0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 21.0.
Results
A total of 52 patients were eligible for the study, and their characteristics are summarized in Table 1. Median age at diagnosis was 67 (range: 34-78) years. All patients (100%) were male and smokers. Human papilloma virus (HPV) status was not evaluated. Five (9.6%), 12 (23.1%), 20 (38.5%), and 15 (28.8%) patients had stage II, stage III, stage IVA, and stage IVB disease, respectively. Distant metastasis or recurrence was not reported up to date. Therefore, statistical analysis was not performed.
Patient and tumor characteristics.

Abbreviations: CPS, Combined Positive Score; TPS, Tumor Proportion Score.
Twenty-one patients (40.3%) had no treatment, 24 patients (46.1%) received radiotherapy, 5 patients (9.6%) received radiotherapy plus chemotherapy, 1 patient (1.92%) received preoperative radiotherapy, and 1 patient (1.92%) received preoperative radiotherapy plus chemotherapy.
There were 35 cases (67.3%) having CPS < 1 and 17 cases (32.7%) having CPS ⩾ 1. The number of advanced-stage (Stage IVA-IVB) patients was 23 and 12, respectively. The median survival of CPS < 1 and the CPS ⩾ 1 group were 54.3 months and 50.3 months, respectively. No statistically significant difference was found between 2 groups (P = .413; Table 2).
Overall survival based on Combined Positive Score.


Abbreviation: CPS, Combined Positive Score.
Tumor Proportion Score of 9 cases was greater than or equal to 1 (17.3%) (Figures 1 and 2).
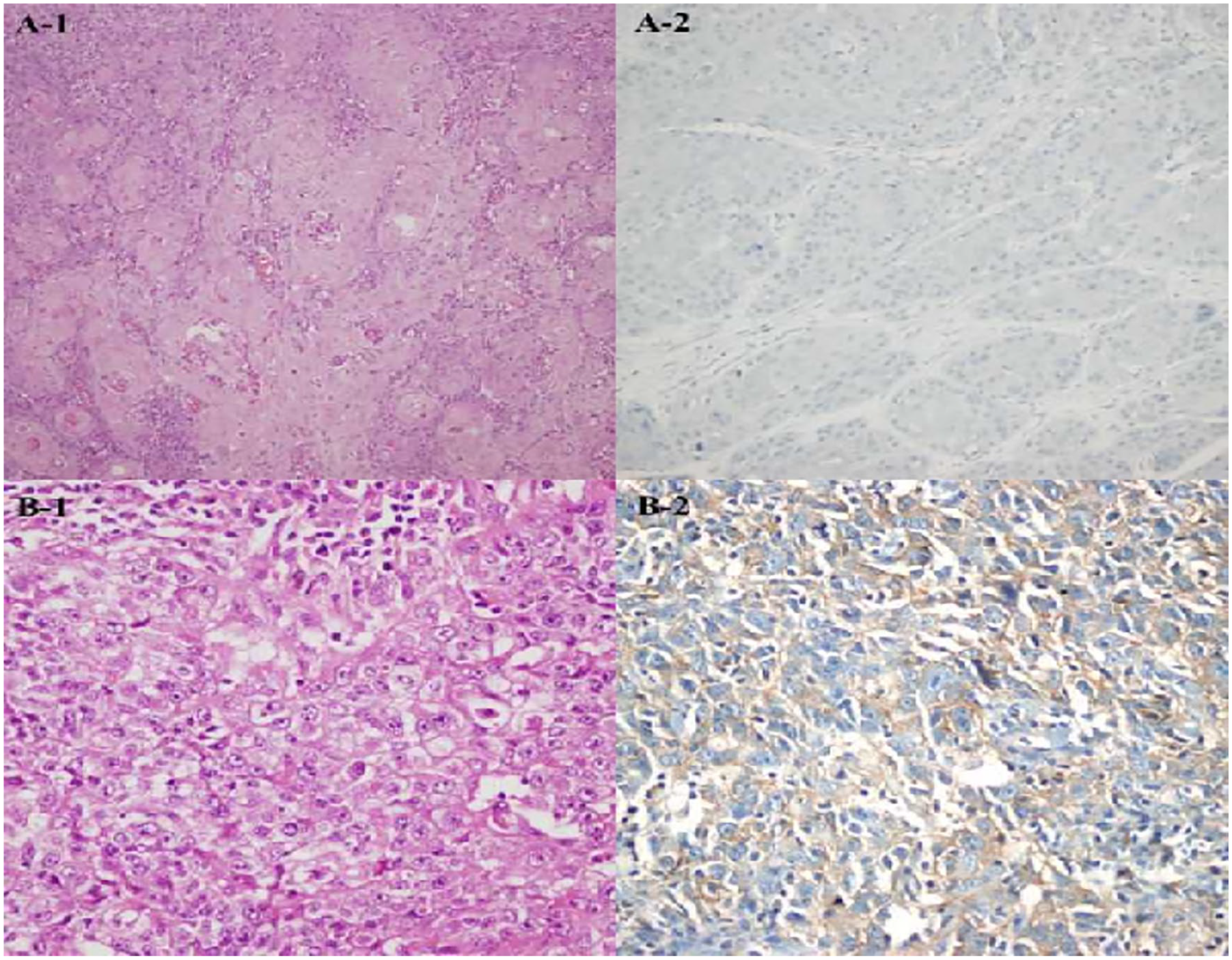
Tumor cell PD-L1 expression: (A) PD-L1-negative (PD-L1 × 200) and (B) diffuse membranous expression of PD-L1 (PD-L1 × 400).

PD-L1 shows focal staining in tumor cells on the left, staining in tumor-infiltrating lymphocytes on the right (PD-L1 × 400).
There was no statistical relationship between TPS, CPS, and other clinicopathological data (age, tumor localization, tumor grade, tumor diameter, clinical-stage, lymphatic, vascular, perineural invasion, lymph node metastasis status, stromal response, necrosis or survival; Table 1).
There was no correlation between patient survival and clinicopathological parameters except lymph node metastasis. When survival rates of N groups were compared, 75% of N0 group, 80% of N1 group, 85% of N3A group, and 62.5% of N3B group were found to be alive, and a statistically significant difference was found (P = .001).
Discussion
The etiopathogenesis of head and neck tumors includes smoking, alcohol, and HPV. Smoking and alcohol consumption are the most important risk factors in SCCs of the oral cavity.
Of 133 oropharyngeal SCC cases, Kim et al 3 found no association between PD-L1 expression and age, sex, smoking, tumor localization (tonsil, tongue root, soft palate, and oropharynx), and stage.
Cho et al 5 revealed that 39 out of 43 oral cavity SCC cases showed PD-L1 immunopositivity.
Ukpo et al 6 found PD-L1 expression in 84 out of 181 oropharyngeal SCC cases. Similar to Kim et al, 3 they could not observe a relationship between clinical parameters and PD-L1 expression.
Steuer et al 7 could not show a statistically significant difference between PD-L1 expression and survival but addressed the relationship between high PD-L1 expression and increased nodal status.
In contrast to other localizations, smoking and alcohol consumption are the most important risk factors in the etiopathogenesis of laryngeal SCC. Human papilloma virus has a limited role in the pathogenesis of laryngeal SCC. Recent studies have asserted that 4% to 15% of laryngeal SCC cases showed HPV positivity. 8 In those studies, the number of HPV-positive cases was very low. In our study, we did not evaluate the relationship between HPV status and PD-L1 expression.
In their study, Birtalan et al reported that PD-L1 positivity in immune cells of laryngeal SCC was associated with good prognosis. However, they could not show the relationship between gender, localization, stage, and PD-L1. 9
Vassilakopoulou et al evaluated the percentage of PD-L1 and tumor-infiltrating lymphocytes (TIL) on paraffin blocks of 206 patients diagnosed with laryngeal SCC and evaluated mRNA levels of PD-L1 on fresh-frozen sections of 89 patients. It was shown that stromal TIL percentage was correlated with PD-L1 expression, and PD-L1 mRNA levels were correlated with PD-L1 protein levels. They found out that overall survival was low in tumors with low stromal TIL percentage compared to the group with high TIL percentage. Patients whose tumors overexpressed PD-L1 showed a favorable outcome. 10
Müller et al used 2 different cohort groups of 98 and 195 cases, including 27 and 44 laryngeal SCC cases, respectively. They evaluated PD-L1 expression by membranous staining and evaluated scoring as negative for lack of expression, low for minor intensity, and high for strong expression. High PD-L1 levels were detected in 6 and 9 of these cases, and low PD-L1 levels were detected in 20 and 33 patients, respectively. They could not show a correlation between PD-L1 expression and stage, lymph node involvement, lymphatic and vascular invasion, grade, or extracapsular spread in all cases. They concluded that PD-L1 expression was a strong predictor of poor prognosis and that high PD-L1 expression was associated with distant metastasis in primary tumors. 11
In Heineman et al’s study, 25% of 279 HNSCC cases were located at the larynx and PD-L1 somatic mutation status evaluated by whole genome sequencing and is found to be negative. Genetic changes were detected in 6.2% of the cases. The relationship between PD-L1 and caspase-7, ZFYE9 and PlgR (CT) genes has been shown. In the same study, they revealed that PD-L1 expression in HNSCC was 60 times higher in comparison with renal cell carcinoma, lung and bladder cancers, and melanoma. 12
In our study, we observed that 35 cases (67.3%) fell into the CPS < 1 group and 17 cases (32.7%) fell into the CPS ⩾ 1 group. Twelve cases with CPS ⩾ 1 were on the advanced stage. Perineural invasion was found to be almost statistically significant (P < .058). 86.7% of CPS < 1 group did not have perineural invasion while 13.3% of CPS ⩾ 1 group was negative.
On the other hand, TPS of 9 cases (17.3%) out of 52 laryngeal SCC cases had greater than or equal to 1. There was no significant difference between TPS and clinicopathological data and survival.
Since our study did not include stage IVC cases (any T, any N, M1), we could not evaluate the relationship between metastasis and CPS or TPS.
There are very few studies evaluating PD-L1 expression on laryngeal SCC. Our study is single-centered and one of the few studies that focus on larynx. Consistent with most of the studies, no correlation was found between CPS, and TPS and clinicopathological data, and survival.
Discordance on PD-L1 expression in studies of HNSCC might be attributed to applying different antibodies and using different cut-off values for defining the positive expression and subjective scoring criteria, and the intrinsic heterogeneity of PD-L1 expression within tumors.
The limitation of our study was a relatively short follow-up period and a small number of cases which may cause the misinterpretation of statistical data. Other weakness of our study was that advanced-stage patients were not included in our cohort. Longer follow-up periods with larger series might remark the effects of PD-L1 staining/scoring. Nevertheless, studies on PD-L1 expression on laryngeal SCC cases were a few in English literature. In this respect, our study shed a light on this emerging subject.
Conclusions
The percentage of CPS ⩾ 1 was 32.7%. Twelve cases were on advance stage in this group.
In our study, no correlation was found between TPS, CPS of PD-L1 staining and clinicopathological data, and survival.
Footnotes
Acknowledgements
The authors are grateful to Bugra Taygun Gulle (MD: Department of Public Health, Istanbul University, Istanbul Faculty of Medicine, Istanbul, Turkey), for his help in statistical analysis.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Substantial contributions to the conception or design to the work or the acquisition, analysis, interpretation of data for the work (Sebnem Batur Zeynep Ecem Kain Emine Deniz Gözen Nuray Kepil Ovgu Aydın Nil Çomunoğlu). Drafting the work or revising it critically for important intellectual content (Sebnem Batur) Final approval of the version to be published(Nıl Comunoğlu).