
Abstract
Intraplacental leiomyomas are extremely rare and are generally incidental findings in term placentas. We present the first reported case of a placental leiomyoma associated with preterm intrauterine fetal demise, with histological findings providing the cause of adverse outcome. This was an intrauterine fetal demise detected at 26 weeks gestation with a placental finding of a 2.8-cm leiomyoma. Histological findings in the placenta and fetus were consistent with intrauterine fetal demise of weeks. The umbilical cord was markedly hypercoiled, with 6 twists per 10 cm. Features of maternal vascular malperfusion were evident in the placenta, including villous hypermaturity, an infarct adjacent to the leiomyoma, and retention of smooth muscle in spiral arterioles within the decidua overlying the leiomyoma. Implantation-site trophoblasts invaded into the leiomyoma and the overlying decidua. We hypothesize that incorporation of the leiomyoma into the placenta contributed to fetal demise due to disordered placental implantation, implying that these tumors may not be as benign and incidental as previously described. The finding of implantation-site changes in the leiomyoma may also suggest a potential cause for this rare tumor.
Introduction
Nontrophoblastic, nonvascular intraplacental tumors are rare. Of these tumors, leiomyomas within the placenta or fetal membranes are exceedingly rare, with fewer than 10 reported cases.1-7 The proposed cause of these lesions is the incorporation of submucosal leiomyomas into the placenta or fetal membranes. 3 Nearly all prior reports of intraplacental or fetal membrane leiomyoma have been incidental findings with term or near-term delivery of viable infants. We describe a placental leiomyoma associated with second-trimester intrauterine fetal demise.
Case Report
A 32-year-old G2P0 with a history of one prior spontaneous abortion and no other significant past medical history was diagnosed with intrauterine fetal demise at 26 weeks 3 days gestation. An ultrasound at 19 weeks gestation showed a fetus with measurements appropriate for gestational age and normal anatomy. Fetal heart rate and fetal movement were detected at a 22-week prenatal checkup. At delivery, a firm mass was palpated at the cervical os; abdominal ultrasound showed a 5-cm mass consistent with leiomyoma.
At autopsy, the fetus was phenotypically male and small for the stated gestational age of 26 weeks, with external measurements and weight more commensurate with a gestational age of 20 to 21 weeks. In addition, the fetus exhibited extensive changes of maceration consistent with an intrauterine fetal demise interval of weeks, including skin slippage sparing only the palms and soles and extensive loss of nuclear basophilia in all histologically examined organs. No significant dysmorphic changes or structural abnormalities were noted.
The placenta was received disrupted and weighed 100 g after trimming umbilical cord and membranes, less than the 10th percentile for both 21 and 26 weeks gestational age. The umbilical cord was dusky, edematous, and hypercoiled, with a coiling index of 0.6 (17 coils per 28 cm; expected coiling index 0.1-0.3), right-handed twist, and eccentric insertion 1 cm from the placental disk edge (Figure 1A). Fetal membranes were edematous, dusky, and semi-translucent. The placental parenchyma was pale pink-tan and contained a well-defined, firm, white-pink intraplacental nodule (2.8 cm) with a whorled-appearing cut surface, involving the maternal surface and approaching within 0.5 cm of the fetal surface, overall occupying approximately 20% of the maternal surface (Figure 1B). This nodule was incorporated into the placental parenchyma and could not be easily separated from the disk. Histologically, the nodule was well-circumscribed and consisted of long fascicles of spindled cells with long tapered nuclei and no significant atypia or mitotic activity; these cells were diffusely positive for smooth muscle actin, consistent with leiomyoma (Figure 2). There was decidua focally overlying the leiomyoma on the maternal surface, with associated implantation-site trophoblasts. The opposite aspect of the leiomyoma, adjacent to the placental parenchyma, was partially involved by implantation-site trophoblasts. Sex chromosome fluorescence in situ hybridization was performed to confirm the maternal vs. fetal origin of the leiomyoma. The leiomyoma had a sex chromosome complement consistent with maternal origin (XX); this was in contrast to the rest of the placenta, which was cytogenetically male (XY) as expected given the phenotypically male fetus.

Placental gross findings. (A) The umbilical cord is dusky and hypercoiled with approximately 6 coils per 10 cm length. (B) On cross section, the placental parenchyma is pale pink-tan with a discrete 2.8cm firm, white-tan, whorled-appearing nodule underlying the maternal surface and extending nearly to the fetal surface.
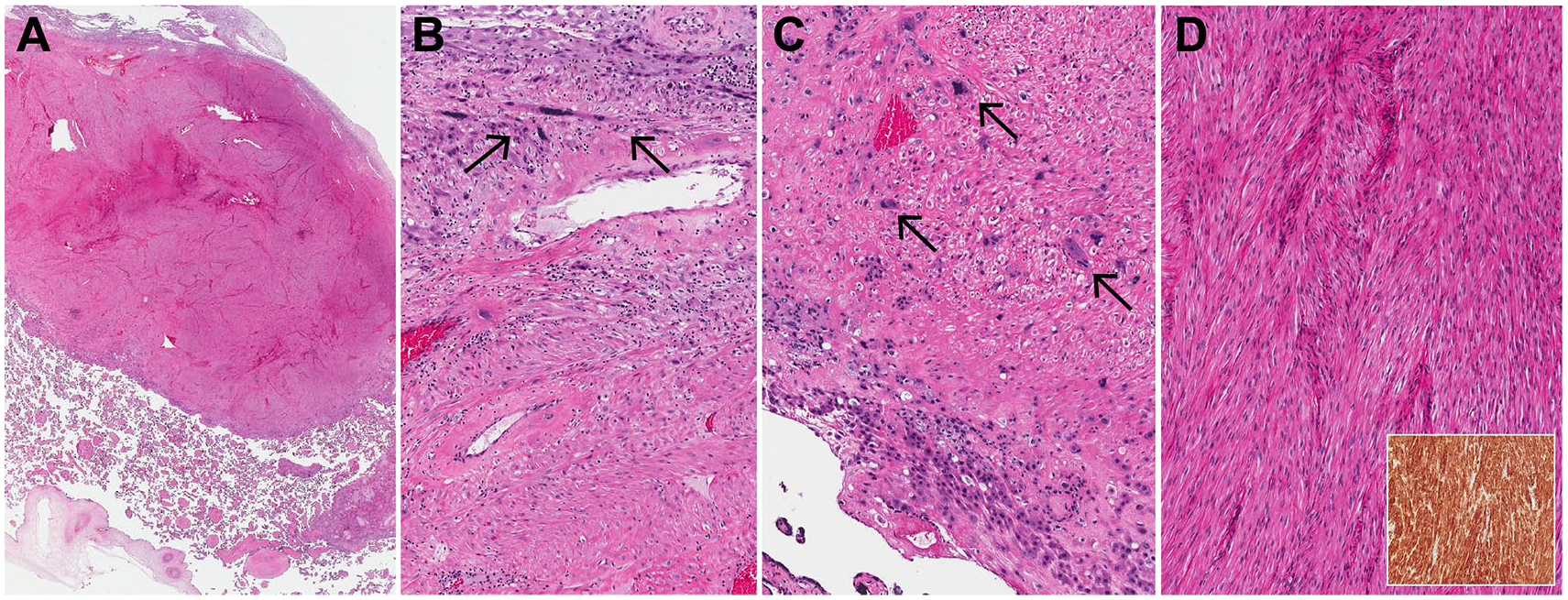
Placental leiomyoma histological findings. (A) On low power, there is a well-defined solid nodule underlying maternal decidua and distinct from the fetal surface (4×). (B) There is decidua with implantation-site trophoblasts (top of image; arrows) overlying the leiomyoma (100×). (C) At the interface of the placental parenchyma with the leiomyoma, there are implantation-site trophoblasts infiltrating into the leiomyoma (arrows; 100×). (D) The leiomyoma consists of long fascicles of spindled cells with eosinophilic cytoplasm and long tapered nuclei (100×). Inset: Tumor cells are diffusely positive for smooth muscle actin (100×).
Distant from the leiomyoma, there were foci of smooth muscle fibers consistent with myometrium adherent to the maternal surface of the placenta and adjacent to extravillous trophoblasts and rare sclerotic villi with few layers of intervening decidua (Figure 3A). Chronic inflammation with plasma cells was found in the decidua as well as within the leiomyoma. Consistent with the maceration changes seen in the fetus, the placenta showed diffuse changes consistent with intrauterine fetal demise, including extensive villous fibrosis and fetal vessel thrombosis with recanalization (Figure 3B). Changes of maternal vascular malperfusion were also evident, including hypermaturity with multiple small villi and syncytial knots (Figure 3B) as well as a 0.7-cm placental infarct adjacent to the leiomyoma (Figure 3C). Within the decidua adherent to the surface of the leiomyoma, spiral arterioles showed retention of a smooth muscle layer (Figure 3D).
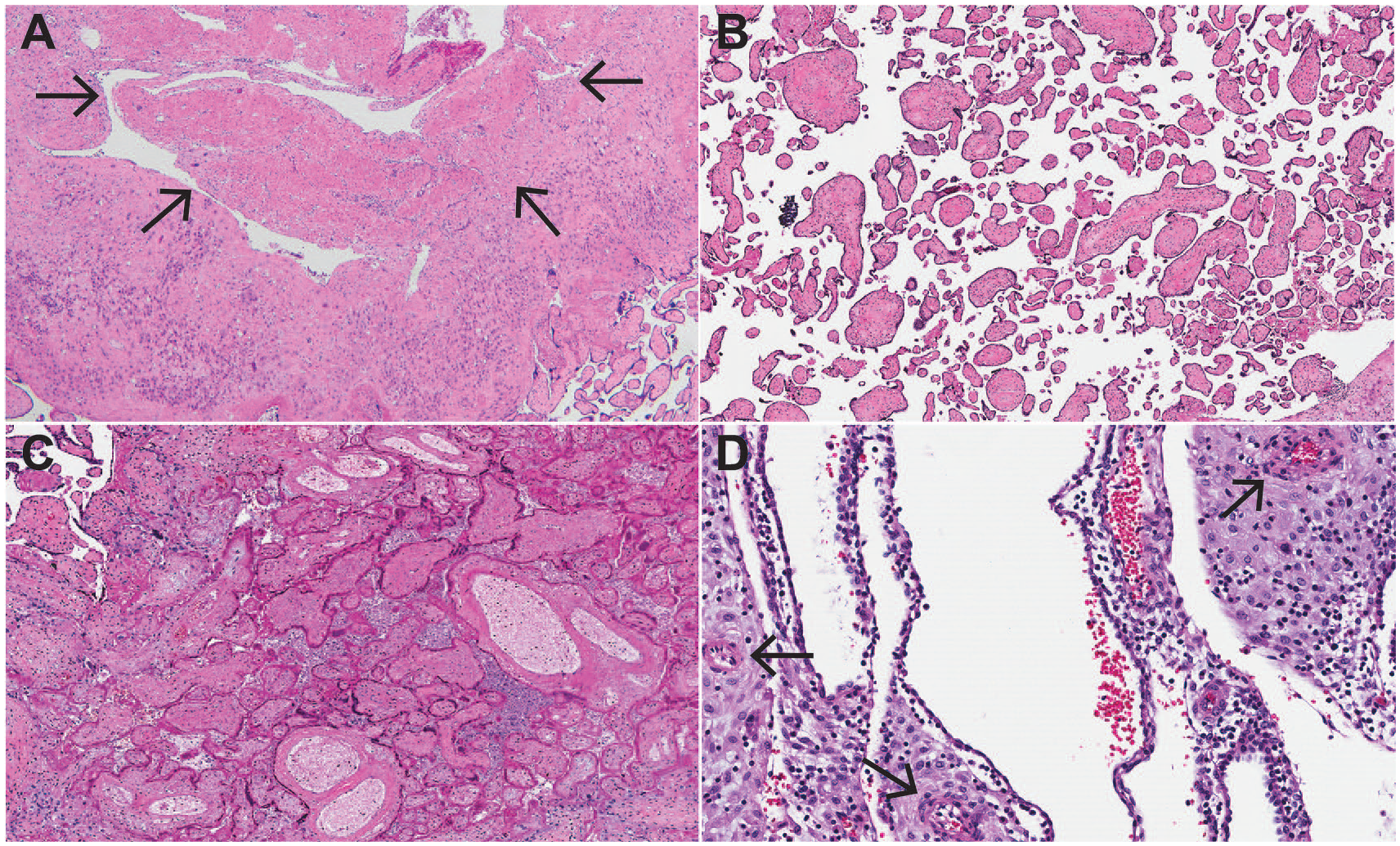
Other histological findings. (A) The basal plate distant from the leiomyoma shows large fragments of adherent myometrial fibers (arrows; 40×). (B) Placental villi show diffuse loss of vascularity and sclerosis, as well as accelerated villous maturation with small terminal villi and increased syncytial knots (40×). (C) Adjacent to the leiomyoma, there is a parenchymal infarct with loss of nuclear basophilia and villous agglutination (40×). (D) Decidua adherent to the surface of the leiomyoma shows retention of smooth muscle in spiral arterioles (arrows; 200×).
Discussion
In this case, histological findings were of an intraplacental leiomyoma involving the maternal surface, with features consistent with disordered implantation and suggestive of placenta accreta elsewhere in the placenta. Placental features that likely contributed to intrauterine fetal demise included a hypercoiled umbilical cord (which would be expected to lead to fetal vascular malperfusion, in this case obscured by diffuse postmortem vascular changes) and features of maternal vascular malperfusion, in this case potentially attributable to the disordered implantation. Each of these individual features is known to be associated with an increased risk of preterm labor and fetal demise.8,9 In addition, chronic inflammatory lesions such as deciduitis with plasma cells are hypothesized to result from a maternal anti-fetal immune response. 10 The presence of maternal vascular malperfusion in the context of a maternal history of a prior spontaneous abortion may raise the possibility of an autoimmune thrombophilia such as lupus or antiphospholipid syndrome, although this was not noted in the patient’s clinical history and the histological findings are nonspecific. In this case, the presence of histological features of placenta accreta and implantation over a leiomyoma could also be hypothesized to result in altered perfusion by maternal blood, although these changes are not limited to the area directly affected by the tumor and a causal relationship cannot be confirmed.
Placental leiomyomas are exceedingly rare, with only 7 reported cases1-7 (summarized in Table 1). In 4 of these cases, the leiomyoma had been incorporated into the placenta, while the remaining 3 were found in the membranes. Various causes have been proposed for intraplacental leiomyomas. Prior reports of cytogenetic data support a maternal origin for these tumors,3-6 as was seen in this case. The histological apposition of the leiomyoma between decidua and extravillous basal plate trophoblasts has not been previously described. It lends support for the theory that intraplacental leiomyomas may represent endometrial or submucosal leiomyomas that were incorporated into the placenta by invading extravillous trophoblasts early in placental development. Unlike placental leiomyomas, uterine leiomyomas are extremely common, affecting up to 70% of women of childbearing age. 11 To date, the reason for this apparent discrepancy in prevalence is unknown. There are case reports of placental implantation sites on uterine leiomyomas, 12 and it is possible that placental implantation on a leiomyoma represents an intermediate step in the development of leiomyomas that have been fully incorporated into the placenta or membranes. In this placenta, the presence of adherent myometrial fibers elsewhere on the maternal surface also supports disordered placental implantation as a potential contributing factor to placental leiomyoma incorporation.
Clinical, pathological, and cytogenetic features of reported cases of intraplacental leiomyoma.

Abbreviations: FISH, fluorescence in situ hybridization; PCR, polymerase chain reaction; N/A, not available.
Previous cases of placental leiomyomas were associated with delivery of liveborn full-term or near-full-term infants, of which the majority (4/6) were male, and 1 full-term intrauterine demise, also male. This is the first case of placental leiomyoma associated with second-trimester intrauterine fetal demise. A large leiomyoma along the maternal surface would be expected to restrict maternal perfusion of the placenta due to physical obstruction. Correspondingly, chronic placental effects of poor maternal vascular perfusion were evident in this placenta, including an infarct, villous hypermaturity, and inadequate spiral arteriole remodeling, as would be expected with disrupted placental implantation. As most of the other intraplacental leiomyomas were presumed incidental findings in liveborn term or near-term infants, it is possible that the leiomyoma in this case was merely an incidental finding in an intrauterine fetal demise due to other causes. However, although multiple placental factors, including umbilical cord hypercoiling, likely contributed to intrauterine fetal demise, poor uteroplacental perfusion due to placental incorporation of the leiomyoma and disordered implantation is likely contributory given the downstream histological changes that were seen. This thus represents the first case of intrauterine fetal demise attributable at least in part to a placental leiomyoma with histological evidence of downstream placental effects. When identified in the placenta, these tumors, although histologically benign, should be considered potentially harmful for the developing fetus.
Footnotes
Funding:
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SCK: case diagnosis and review, literature review, manuscript writing and editing, final approval of manuscript.
FB: case review, literature review, manuscript writing and editing, final approval of manuscript.