
Abstract
Renal cell carcinoma (RCC) commonly metastasizes to areas such as the lungs, liver, bone, brain, adrenals, and lymph nodes. We present a rare case of a 59-year-old female patient with RCC metastasis to the gallbladder. The patient had undergone right nephrectomy for RCC more than 6 years prior to the metastasis. During routine follow-up, a polypoid lesion of the gallbladder was identified. Laparoscopic cholecystectomy was performed, and pathologic examination of the specimen revealed metastatic RCC. The patient was completely asymptomatic, which reinforces the importance of postoperative follow-up. Renal cell carcinoma is one of the few common malignancies for which there is good evidence of survival benefit from surgical resection of the metastatic tumours.
Keywords
Introduction
Renal cell carcinoma (RCC) accounts for approximately 3% of all adult malignancies, and clear cell type represents about 70% of all RCC. It is well known for its high rate of metastasis, with approximately 30% of patients having metastatic disease at initial presentation, and another third of patients develop metastasis during follow-up. 1 We report a rare case of RCC, clear cell type, metastasizing into the gallbladder.
Case Report
A 59-year-old woman was admitted to the hospital with an upper pole mass in her right kidney. A right radical nephrectomy and caval thrombectomy were successfully performed and the patient was discharged. The patient enrolled in a blinded randomized controlled trial of the effects of adjuvant sunitinib/placebo or sorafenib/placebo in high-risk, non-metastatic RCC. 2 Due to some symptoms experienced by the patient, she was presumed to have been assigned to an active treatment arm.
The patient was performing extremely well with negative scans. Six years later, she complained of lower urinary tract symptoms and right flank pain. Kidney functions were normal; however, an ultrasound test showed a pedunculated, 2-cm lesion within the gallbladder body (Figure 1). The cause of the lesion was unclear, and surgery was offered because the lesion was greater than 1 cm in size. The preoperative differential diagnoses included gallbladder polyp, adenomyomatosis, and less likely gallbladder malignancy. The patient underwent an uncomplicated laparoscopic cholecystectomy.

Ultrasound demonstrating a 2-cm pedunculated gallbladder polyp.
Pathological examination showed a normal-sized gallbladder with an intact wall. On opening the gallbladder, a 1.1 cm polypoid tumour was attached to the mucosa. Microscopically, the lesion was composed of malignant clear cells with an overlying ulcerated epithelium (Figures 2 and 3). Immunohistochemistry showed positive staining of the neoplastic cells for vimentin, and cytokeratin AE1/AE3, and negative staining for cytokeratin 7 (Figures 4 and 5). The morphologic and phenotypic profiles were consistent with a metastasis from the patient’s previous primary clear cell RCC. The cystic duct node was negative for malignancy. The patient has since been in good health.

Low power view (40× magnification) of a cellular nodule within the gallbladder wall.

The 200× magnification illustrates the abundant clear cytoplasm, round nuclei, and prominent nucleoli nested within a capillary network. No sarcomatoid features were present in either primary or metastatic renal cell carcinoma.
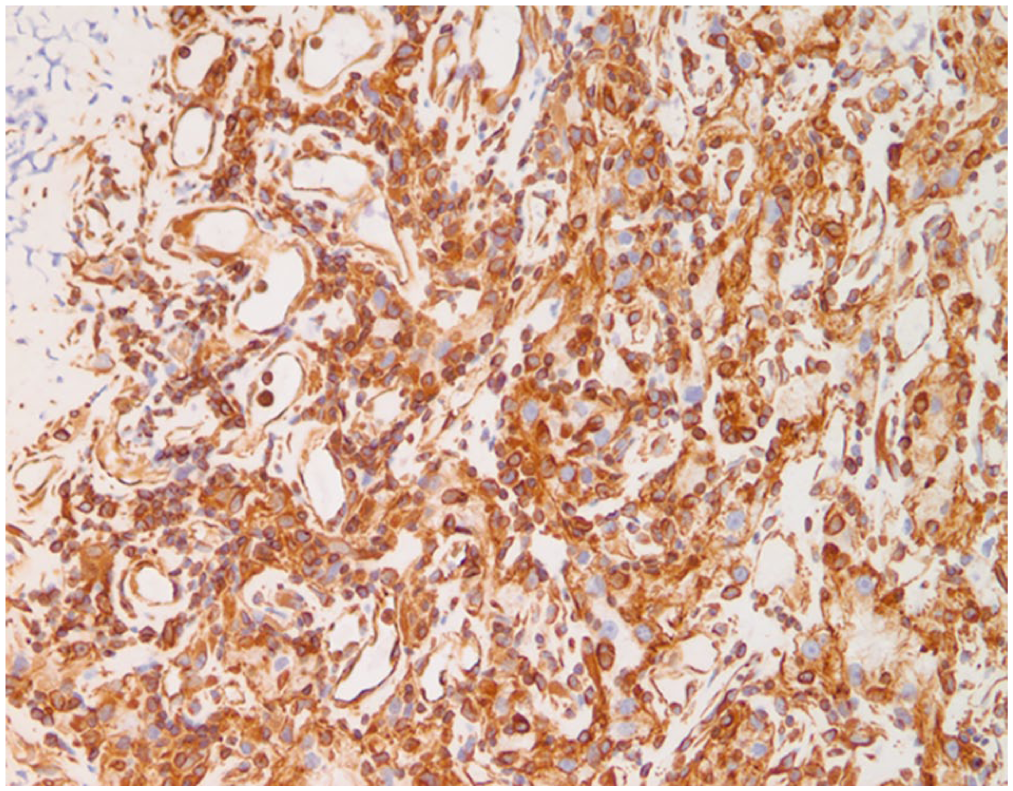
The neoplastic cells have cytoplasmic positivity for vimentin immunomarker, characteristic of renal clear cell carcinoma but uncommon in other carcinomas.
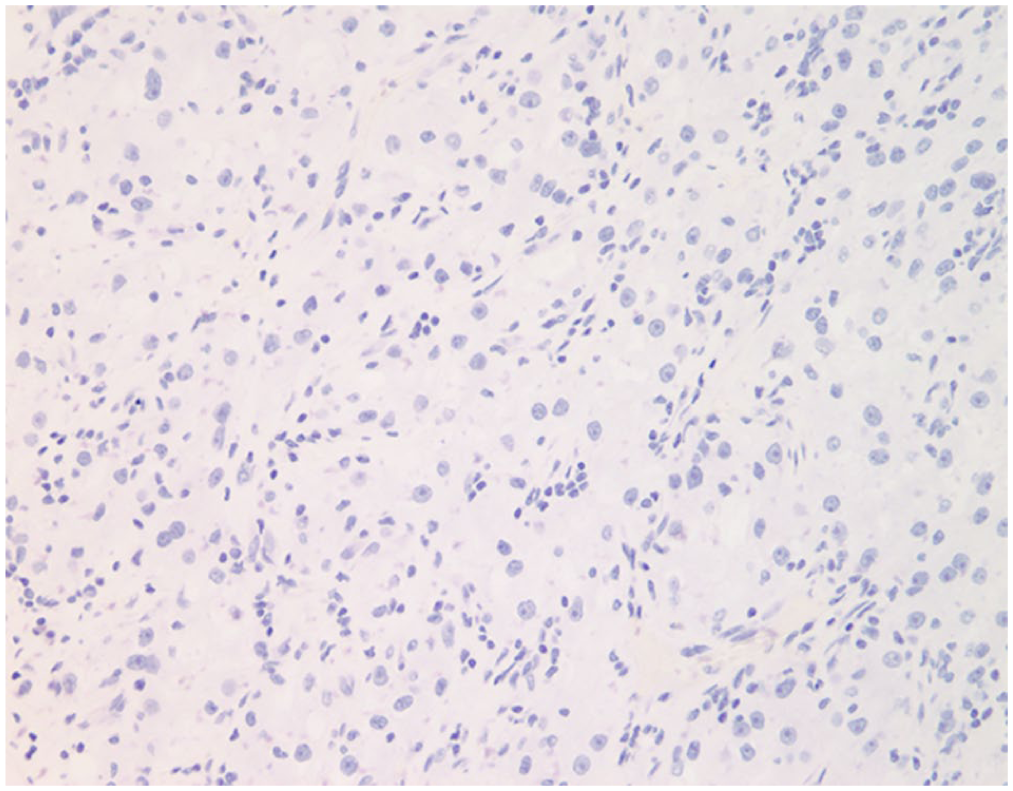
The neoplastic cells stain negatively for the cytokeratin marker CK7, which is positive in biliary tract and many other carcinomas, but characteristically negative in renal cell carcinoma.
Discussion
Metastases to the gallbladder (MGB) are very uncommon. There are case reports of multiple different malignancies that can metastasize to the gallbladder, usually in cases of diffuse metastasis. Isolated MGB are less common and have been described with primaries of gastric cancer, RCC, hepatocellular cancer, non–small cell cancer of the lung, and melanoma. In a review of computed tomography (CT) scan findings of metastasis to the gall bladder, Choi et al 3 described a series of 24 patients with metastasis to the gall bladder. The most common primary tumour metastasized to the gallbladder was gastric cancer (n = 8), followed by RCC (n = 4) and hepatocellular carcinoma (n = 3). All gallbladder metastases (n = 21) presented either with infiltrative wall thickenings (n = 15) or as polypoid lesions (n = 6). Metastatic adenocarcinomas to the gallbladder presented as infiltrative masses with persistently enhancing wall thickenings, while non-adenocarcinomatous metastases usually presented as polypoid lesions with early wash-in and wash-out. 3
Like many cancers, RCC has typical locations to which distant metastases occur: lungs, liver, brain, adrenals, and lymph nodes. Renal cell carcinoma, especially clear cell RCC, is also well known to metastasize to unusual locations, sometimes decades after initial tumour treatment. 4 It is unknown why metastases often present so late. 4
Gallbladder metastases from RCC are very rare, although they have been previously described.5–9 Most present metachronously, with a median time to presentation of 5 years. There is one case report of a gallbladder metastasis presenting 27 years after the primary tumour. 10 Some cases are only detected at post-mortem examination. 11 Most of such lesions are asymptomatic, although some may present as biliary colic or acute cholecystitis. 8
Identification and resection of solitary/localized metastases from RCC has a proven survival benefit, and evidence of good outcomes after resection of gallbladder metastases has been published.12,13
In the case of a patient with a current or past history of RCC, a symptomatic or incidental gallbladder lesion should raise the possibility of metastasis, and cholecystectomy for diagnostic and therapeutic purposes is indicated. This case highlights RCC’s propensity for metastasis to unusual locations, sometimes following a long disease-free interval.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
ED performed the surgery, KR performe pathological analysis, SS and IW performed literature review and drafted the manuscript. All authors reviewed and had input into the final manuscript.