
Abstract
Introduction:
Some studies reported that there is abnormality in the histopathology of atretic bowel in jejunoileal atresia (JIA). We have made an attempt to assess sequential histopathologic changes in the resected atretic segment.
Material and methods:
The histopathology of the resected segment was evaluated at 1, 3, 5, 7, 9, and 11 cm from atretic end (Sections A to F, respectively). The ratio of inner and outer muscle layer (measured by NIS-Element D software) was calculated at every section. Immunohistochemistry for α-smooth muscle actin (α-SMA) was also done. The findings were compared with control.
Results:
In control set (n = 5), the ratio of inner and outer muscle layer was 1.03. In patients with JIA, the ratio was 0.68 to 0.9 at section A. This ratio varied at various sections in all specimens. In section F, this ratio was 0.95 to 1.09, which is close to control ratio. There were no specific findings related to α-SMA staining.
Conclusions:
It appears that the bowel proximal to the atresia is abnormal for a varied length. It may be a possibility that this abnormality is present at least up to about 10 cm proximal to atresia. Adequate resection is important for optimal outcome.
Introduction
Jejunoileal atresia (JIA) is the most common congenital anomaly of the small intestine and is a major cause of intestinal obstruction in neonates. 1 It is generally considered to result from intrauterine vascular disruptions to a segment of the developed intestine. 1 Ideally, the treatment for this entity is resection of the dilated, proximal, atretic segment and anastomosis to the distal bowel. It has been observed that the proximal segment has ineffective peristalsis and fails to function with lower pressures seen postoperatively. Intestinal dysmotility, which usually has been encountered in the severely dilated proximal segment, is an important problem in postoperative management of patients with JIA. 2
There are certain studies which have demonstrated that there is abnormality in the histopathological morphology of the atretic bowel.2-6 However, apart from sporadic studies, 3 the literature is scarce on what should be the adequate length of bowel resection for optimal outcome of the patients with JIA. This study was undertaken to evaluate the histopathological changes in the resected, atretic proximal bowel in patients with JIA at various levels and to evaluate whether there is any difference in the histopathological features at various levels. Furthermore, it was attempted to assess whether this information could be translated into an effective segment of atretic bowel that may be resected for better outcome.
Material and Methods
It was a prospective cohort study conducted in the Department of Pediatric Surgery, in collaboration with Department of Pathology of a medical university. It was approved by the hospital ethical committee (2365/Ethics/R.cell-17). The consent of the parents was obtained for inclusion in this study. We followed the Anatomical Quality Assurance (AQUA) guidelines endorsed by the EQUATOR Network for conducting this study.
All patients with distal jejunal or ileal atresia in whom laparotomy was performed along with resection of the atretic bowel segment were included in this study. Exclusion criteria included proximal jejunal atresia, duodenal atresia, or multiple atresia.
Procedure
The proximal atretic bowel segment was resected. It was less than 15 cm. The segment was marked by silk ties at 1, 3, 5, 7, 9, and 11 cm, respectively, from atretic end and transferred to neutral buffered formalin for fixation and histopathology. The specimen carefully grossed, representative sections from all sutured sites were labeled (A to F starting from atretic segment) and embedded for histological examination. Thus, there were 6 sections per patient (Figure 1). After processing, each section was first stained with hematoxylin and eosin and detailed evaluation was performed by the consultant pathologist (P.A.) for morphological features, namely, mucosal status, muscle architecture, presence of ganglion cells, inflammation, and fibrosis. All observations were recorded and sections from every marked site were compared to see for changes occurring in atretic bowel with respect to distance from the atretic end.

Line diagram of the distance from atretic end at which sections were taken for histopathological evaluation.
After histological evaluation, every paraffin block was subjected to α-smooth muscle actin (α-SMA) immunohistochemistry (IHC) by microwave-mediated antigen retrieval method at high pH (TRIS-EDTA buffer pH 9). Primary antibody used was α-SMA (pre-diluted ready-to-use Rabbit polyclonal antibody, DAKO, Denmark) and secondary antibody was Dako Envision FLEX Detection system (high pH). Masson trichrome stain was performed in those sections where there was histological evidence of fibrosis for confirmation. No special stain and IHC was performed for identification of interstitial cells of Cajal (ICC) or other enteroendocrine cells.
All the hematoxylin and eosin–stained sections which were studied were also interpreted with the help of NIS-Element software (Version 4.5 for Windows, Nikon Corporation, Tokyo, Japan). The thickness of inner and outer muscle layers of muscularis propria was measured, and the ratio of inner and outer muscle layer was calculated at every section. The findings were compared to age-matched controls (ie, neonates in this study).
We obtained control specimen from patients who underwent bowel resection for non-inflammatory congenital pathology. In this study, the cause in control population was patent vitello-intestinal duct (VID). The small healthy bowel segment resected along with patent VID was used as control.
Results
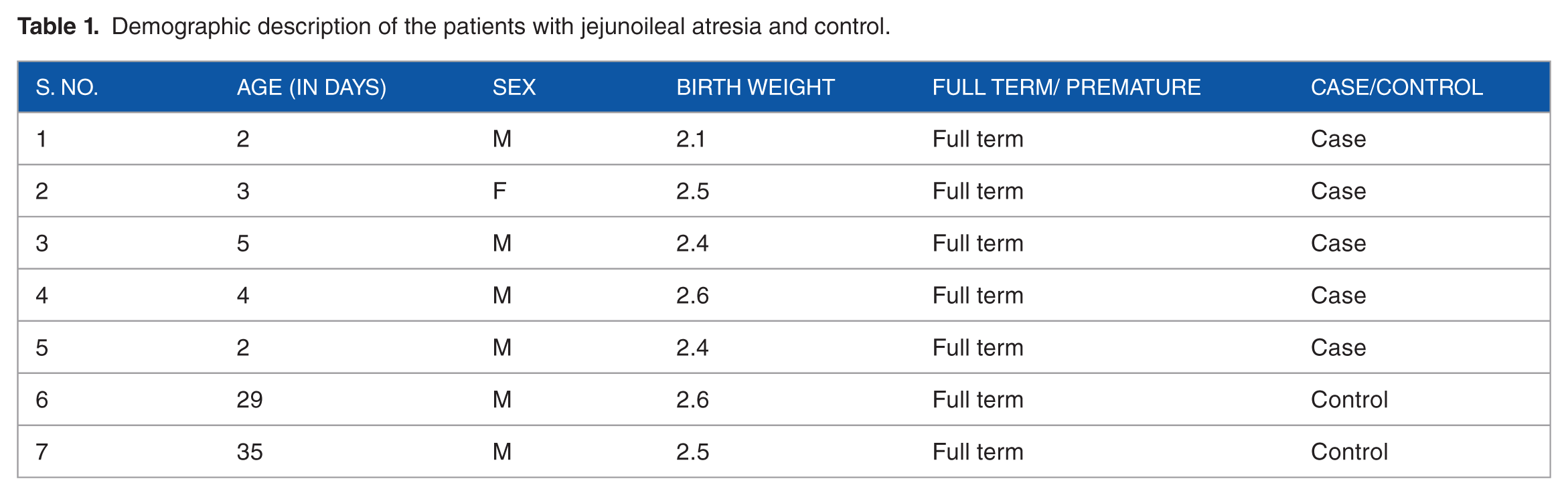
The duration of this study was 1 year. During this period, 15 patients of bowel atresia were operated. Of these, nine had JIA, five had duodenal atresia, and one had large bowel atresia. Of nine patients having JIA, four were of proximal jejunal atresia. Thus, we evaluated 5 patients in this study. There was no patient of multiple atresia in this series. The age range was 2 to 5 days. The weight was between 2.1 and 2.6 kg. There were 2 control specimens (Table 1). There was no premature patient in these 5 patients.
Demographic description of the patients with jejunoileal atresia and control.
The mucosa was unremarkable in all specimens. In submucosa, dilated and congested blood vessels were noted in sections A to C in 2 patients and section A in 1 patient. It was normal in the remaining patients. Muscularis mucosa was hypertrophied in section A to C in 2 patients. Muscle fibrosis was present in few sections. Ganglion cells were present in all sections (Table 2); however, the number increased as we moved from section A toward section F. Besides, the morphology of ganglions cells was close to normal in section F as compared to section A. All layers were normal in the control specimens.
Histopathological features of patients with jejunoileal atresia evaluated in the study.

Abbreviation: ur, unremarkable.
Ganglion cells were present in all sections; however, number increased as we proceeded from section A to section F.
In both control specimens, the ratio of inner and outer muscle layer was 1.03. In patients, the ratio was 0.68 to 0.9 at section A. This ratio varied at various sections in all specimens with highest ratio at section C. In section F, that is, the proximal most section, this ratio was 0.95 to 1.09, which was close to control ratio (Figures 2 to 5).

Photomicrograph showing 2 control specimens (A and B, HE ×400). The thickness was measures by NIS element software, which is visible.
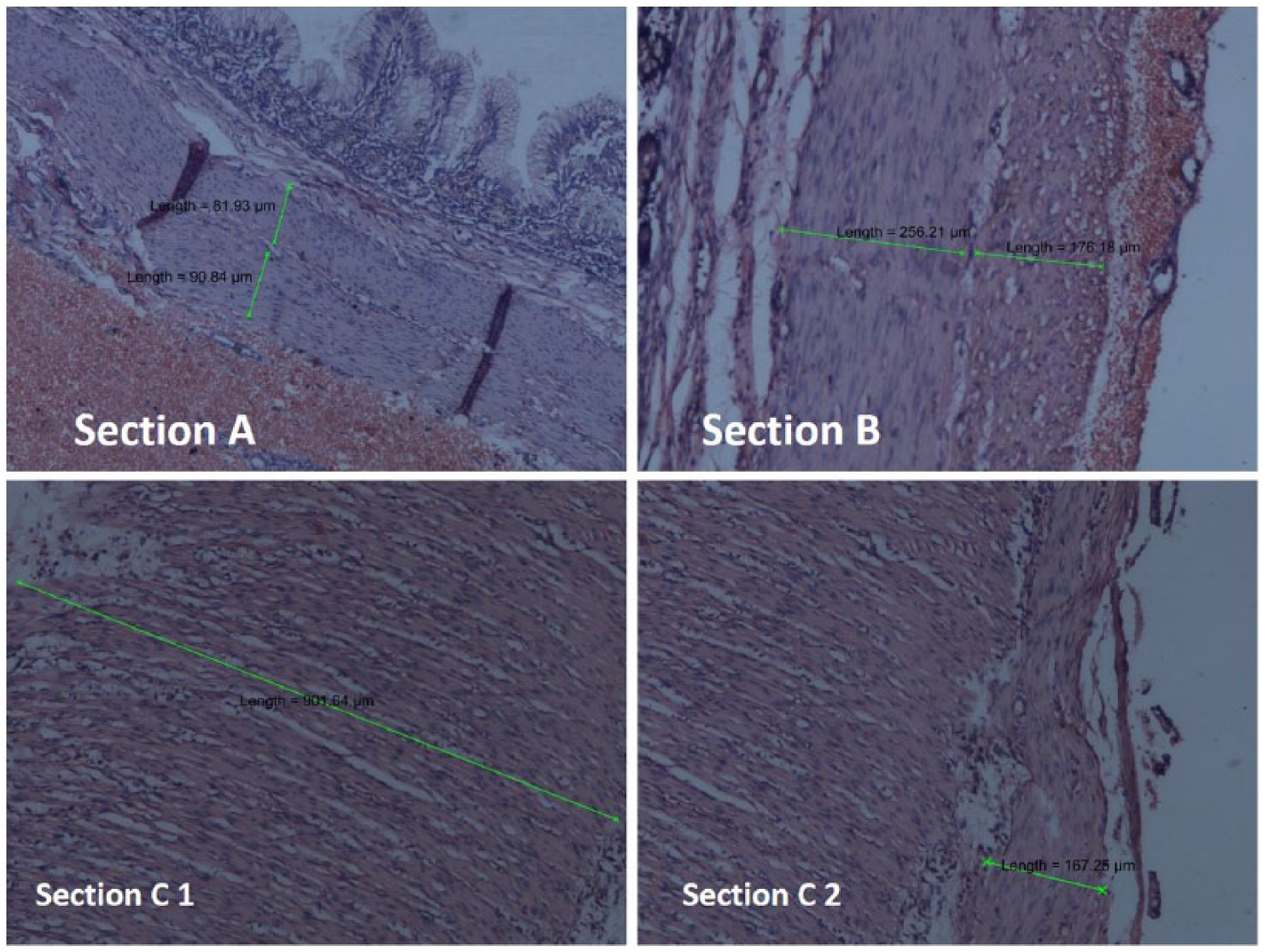
Photomicrograph showing sections A to C of atresia (HE ×400). Both muscle layers are visible in sections A and B. Section C1 is showing inner circular muscle layer and section C2 is showing outer longitudinal layer. Muscle layer is thickest in section C1. The measured muscle thickness is depicted over the muscle layer.
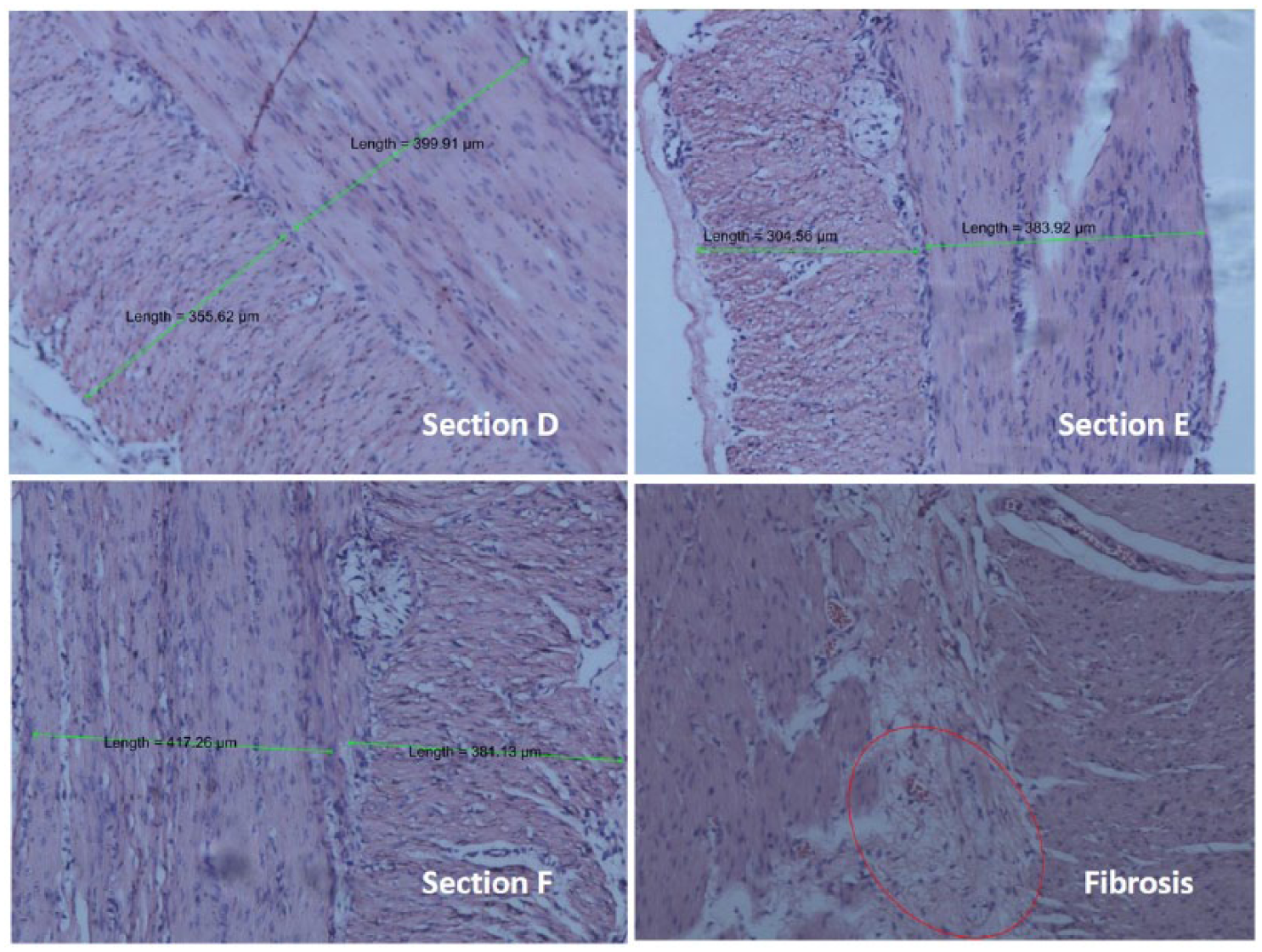
Photomicrograph showing sections D to F of atresia (HE ×400). Both muscle layers are visible in these sections. The measured muscle thickness is depicted over the muscle layer. Last photomicrograph is showing fibrosis, which is encircled.

Diagrammatic representation of all specimens and control. It is obvious that all specimens have varied ratio of inner circular and outer longitudinal muscle layer. This is coming close to control ratio in section F.
There was presence of fibrosis in 1 specimen. We could not find any abnormality related to α-SMA expression.
Discussion
Functional intestinal obstruction at the site of anastomosis has been an important postoperative complication, 1 which affects the outcome of the patient. The cause of intestinal obstruction has been believed to be ineffective peristalsis due to grossly dilated atretic segment. 7 Procedures such as plication or tapering enteroplasty have been suggested to counter this. 7 However, postoperative intestinal motility disorders remain the most common clinical complication of intestinal atresia. 8
In the last 20 years, the focus has shifted on the histopathological changes, which occur in the atretic segment. These are supposed to be the causative factor for the postoperative motility disorders. It has been suggested that there is presence of segmental intestinal musculature defect in patients with small bowel atresia. 9
It was observed in one experimental study on chick intestinal model that there are alterations of the intramural nervous distributions. 10 Taking this study further in neonates having JIA, the authors observed that there was decreased expression of neural elements protein gene product (PDP) and NADPH-d. Besides, there was decreased expression of pacemaker cells, α-SMA, and hypertrophy of muscle layers as compared to controls. 2 We had not found any abnormality regarding α-SMA expression in our series. However, hypertrophy of muscle layer was evident in all of the specimens, which was well observed and documented by software-based annotations and measurement of the muscle layer thickness (see “Material and Methods”).
In a series of 10 patients with JIA, authors took sequential samples at 2 and 4 cm proximal to atresia and 1 and 2 cm distal to it. 3 The authors noted segmental absence of muscle layers at atretic end and 2 cm proximal to atresia, but near normal pattern at 4 cm. With regard to ganglion cells, the authors found that mean number, diameter, and the intensity of the ganglion cells were decreased when compared with those at 4 cm proximal to the atresia and control group. In contrast to it, we observed that ganglion cells were decreased in number at section A, and this abnormality persisted beyond the 4 cm length. However, as mentioned above, segmental absence of muscle layer was not observed by us. Abnormality of ganglion cells, loss of polygonal architecture of the meshwork of nerve fibers, and decreased expression of NADPH diaphorase has also been observed by others. 4 However, they had not evaluated the distance up to which these changes persisted.
ICC which are believed to be the pacemaker cells and play a role in slow wave activity of intestine have been observed to be decreased in the atretic bowel. 5 As we intended to study the histomorphological alterations and α-SMA, we did not perform any special stain to assess the presence and absence of ICC in the atretic segment. Correct identification of these cells on morphology alone is difficult. 11
All these studies suggest that the histopathological changes, which occur in the atretic bowel, affect the postoperative outcome of the neonates. It is mentioned that inadequate resection of the atretic segment may lead to postoperative enteropathy like dilation and dysmotility of proximal intestinal segment. 5 But what is that adequate resection rests with the operating surgeon; no guidelines, which keep both histopathology and clinical features together, have been recommended.
In this study, the use of NIS element software is a novel edition in assessment of the JIA histopathology. This is a simple maneuver; it also makes the observation and interpretation objective reliving the interobserver variability as the software is used to perform the annotations and measurements. Its use revealed that the most common area for abnormally thickened muscle layer lies about 5 cm proximal to the atretic end. By sequential assessment and comparing with control set, it appeared to us that about 11 cm of bowel needs to be resected for better outcome. On the basis of expression of proteins calretinin (CR), glial-derived neurotrophic factor (GDNF), bone morphogenetic protein 2 (BMP-2), c-kit, α-SMA, and S-100 protein, Wang et al 8 concluded that about 15 cm of bowel may be resected for optimum outcome. As in this study, they observed that normal ganglion cells are present at about 10 cm from atretic end. Although they found lower positive staining for α-SMA as compared to control, we did not found such changes. It may be queried as to why a limit of 11 cm was set in this study. As there are sporadic studies on this topic, a predetermined limit of bowel for histopathological assessment was not possible. This limit could have been an arbitrary one. With clinical correlation of previously operated such patients, we could see that dilation of the atretic bowel was coming close to normal at about 10 cm from atretic end. We felt that a histopathological supplement to clinical observation may guide us for optimal resection.
In this study, we performed the detailed morphological evaluation, which was limited to small sample size as a pilot project to look for changes which can be easily evaluated even in set-ups with limited resources. As our inclusion criteria included distal jejunal and ileal atresia, we analyzed only these specimens out of 16. There may be an apprehension that the hypertrophy may be due to obstruction, and it may revert if the obstruction is relieved. This, according to us, may be just a speculation. Besides, it would be unjustified to anastomose in a histologically abnormal segment and wait for hypertrophy to revert spontaneously. Another concern may be the management of proximal jejunal atresia. As it is not possible to resect that much of bowel in such cases, resection of bowel as much as possible seems to be a viable option. However, as we have not studied proximal jejunal atresia, this is just a suggestion. The change in ratio may be due to a decrease in the inner circular layer compared to controls or an increase in the outer circular layer. However, because the ratio is evidently altered, it probably indicates that any of the 2 or both speculations may be possible. At this stage, we are not able to comment on the layer specifically involved.
The importance of this study lies in the fact that simple measurement of muscle thickness may show the abnormally thickened segment. This can be measured by simple annotations provided by image analysis software with minimal interobserver variability. This may be helpful to assess the limit of resection. A larger study is recommended to include this simple parameter and hence establish guidelines for minimal resection length to provide with better clinical outcome and avoid on table surgeons decision, made just on gross evaluation.
To conclude, the use of morphometry shows that the bowel proximal to the atresia is abnormal for a varied length. It may be a possibility that this abnormality is present at least up to about 10 cm proximal to atresia. Adequate resection is important for optimal outcome. This being a pilot study, further studies are needed in this regard to substantiate our efforts.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Study conception and design: AP; Data acquisition: AP, AS; Analysis and data interpretation: AP, AP, AS; Drafting of the manuscript: AP, JR, AG; Critical revision: SNK.