
Abstract
Abundant calcifications and clear-cell change may occur in oncocytic thyroid adenoma (OTA). We aimed to report the features of a case of OTA peculiar by the presence of extensive calcifications and of a clear-cell component. The OTA was detected on a right thyroid lobectomy specimen. Clear-cell change was observed in 15%-20% of the cells. Numerous, focally confluent psammomatoid calcifications, resulting in macrocalcifications, were identified. The nodule cells, uni- or multinucleated oncocytes, including those with clear cytoplasm, expressed heterogeneously TTF1, S100 protein, Bcl2, CD10, as well as CD138 and CD56. Lipid-droplet markers adipophilin and TIP47 were also expressed. In conclusion, we report a rare type of OTA, peculiar by the presence of numerous psammomatoid calcifications and of macrocalcification and by the presence of clear-cell change. Heterogeneity in membrane CD56 and/or CD138 expression as well as cytoplasmic heterogeneity of Bcl2 and lipid-droplet marker TIP47 might be relevant for calcification and clear-cell change, requiring further investigation.
Keywords
Introduction
Oncocytic thyroid adenomas (OTAs) represent a distinctive group of thyroid tumors. Few morphological variants are considered in present classifications although clinical and histological features may vary. 1 Abundant calcifications of psammomatoid type (pseudopsammoma, psammoma-like) in OTAs have been rarely reported. 2
Here, we report a case of OTA morphologically heterogeneous, with prominent calcifications and with a clear-cell component.
Case Report
The nodule, measuring 1.6 cm, was detected on a right thyroid lobectomy specimen. The histology was that of an oncocytic adenoma with follicular and papillary architecture, without necrosis. Clear-cell change was seen in 15%-20% of the nodule. Multifocal psammomatoid calcifications were also observed, focally confluent attaining sizes of 2-3 mm (macrocalcifications; Figures 1 and 2). Calcifications showed varied aspects, small round, elongated, irregular or megamitochondria-like.3,4 The oncocytic cells, including those multinucleated, expressed heterogeneously cytoplasmic thyroglobulin and Bcl2, nuclear TTF1, nuclear and/or cytoplasmic S100 protein, membrane and/or cytoplasmic CD10, CD56, CD138, and anti-mitochondria antibody. CD56 was expressed in pericalcification cells. CD138 was expressed in a similar pattern, however, in a decreased number of cells. Membrane expression was focally granular and heterogeneous. Intracytoplasmic granules/globules (possibly of Golgi-, mitochondria, or endosomal-type) were positive for CD56 and CD138. CD138 was also expressed in several nodule cell nuclei and in the colloid. CD25 (performed for the study of inflammation-related cells) was expressed not only in intra- and extratumor-reactive mast cell and/or lymphocytes but also in rare nodule cell nuclei. Lipid-droplet markers showed different expression patterns. Adipophilin was expressed in a cytoplasmic, low-density, granular pattern in rare cells, while TIP47 in a cytoplasmic, high-density, granular, and diffuse pattern. Adipophilin was also expressed in the nuclei of nodule cells. Immunohistochemistry for WT1, calretinin, and CD68 was negative. Ki67 was expressed in nodule cell nuclei, in particular in binucleated cells suggestive of a post-M immediate cell cycle phase. The clear cells expressed TTF1. Thyroglobulin, anti-mitochondria antibody, and Bcl2 expression were heterogeneous both intranodular and intracytoplasmic, while CD68 expression lacked completely. Intracellular vacuoles (optically blank on hematoxylin-eosin-stained sections) were Bcl2-, S100-, CD10-, and CD56-negative, while CD138 expression was focally membranous. The non-nodular thyroid showed multifocal thyroiditis. A solid-cell nest and an intrathyroid parathyroid were also detected at microscopy analysis. Focal calcifications of the elastic lamina of perithyroid vessels were observed.
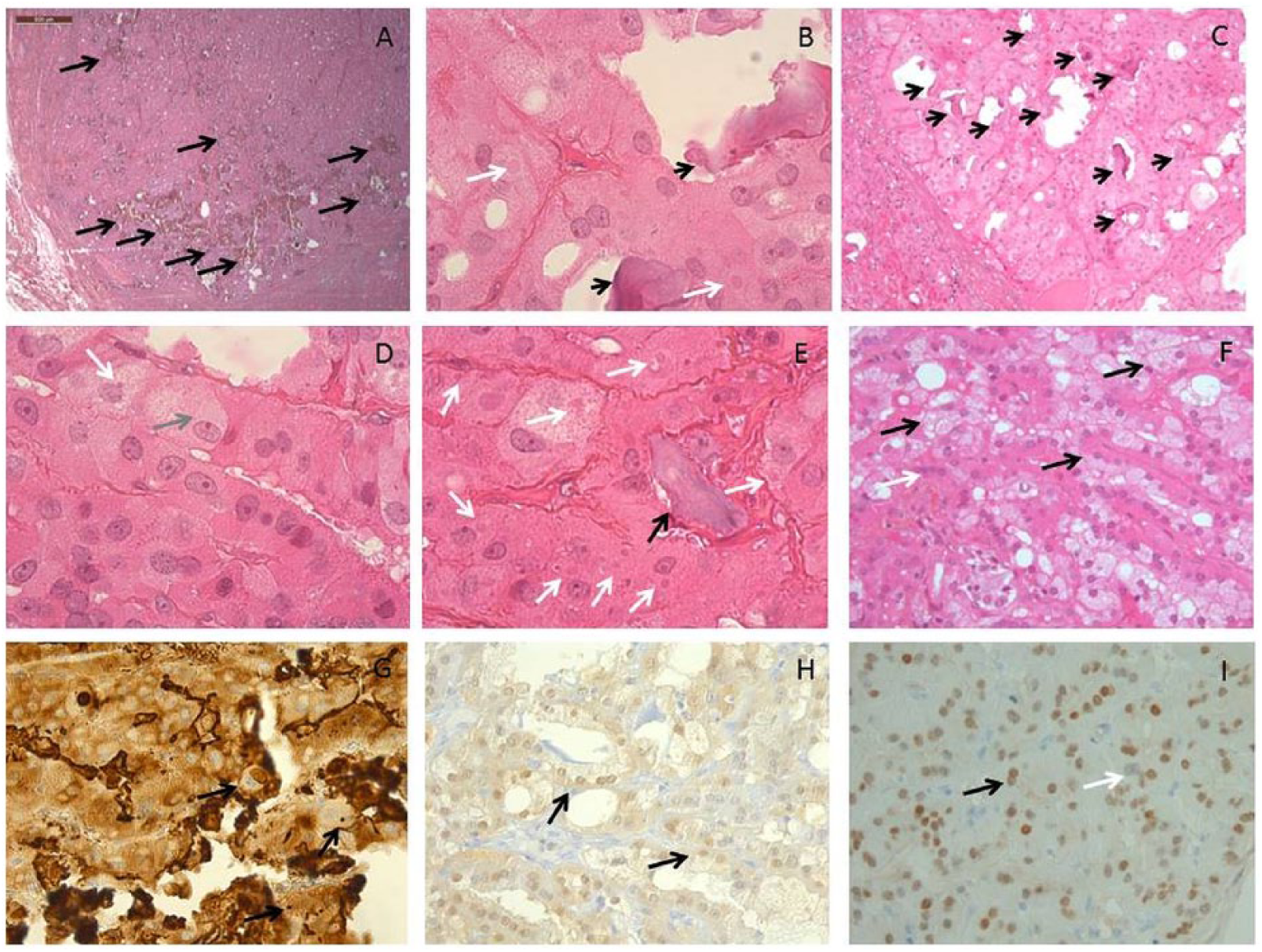
The thyroid nodule showed multiple, confluent calcifications, most of psammomatoid-type (A, B, C, and E: black arrows). Several cytoplasmic globules were seen, round, oval or irregular, rather of megamitochondria- (without or with calcification) or colloid-type than of micronuclei-type (B, D, and E: black arrows for psammomatoid bodies, white arrows for cytoplasmic globules, gray arrow for densely granular mattified, “ground-glass”-like aspect). Nodule cells showed either an oncocytic or clarified cytoplasm. This heterogeneity was observed also at unicellular, intracytoplasmic level, with a polarized pattern: basal oncocytic/luminal clarified (F: black arrow for clarified cytoplasm and white arrows for oncocytic cytoplasm). Thyroglobulin was expressed in both nodule cell types (G). Bcl2 was heterogeneously expressed (H). To note would be the presence of cells showing intracytoplasmic heterogeneity consisting in basal dense staining (black arrow) and luminal lack of staining (H). TTF1 was expressed in most nodule cell nuclei (I). To note would be the fact that binucleated cells showed both a TTF1+ and TTF1− immunoprofile (I: black and white arrows, respectively).
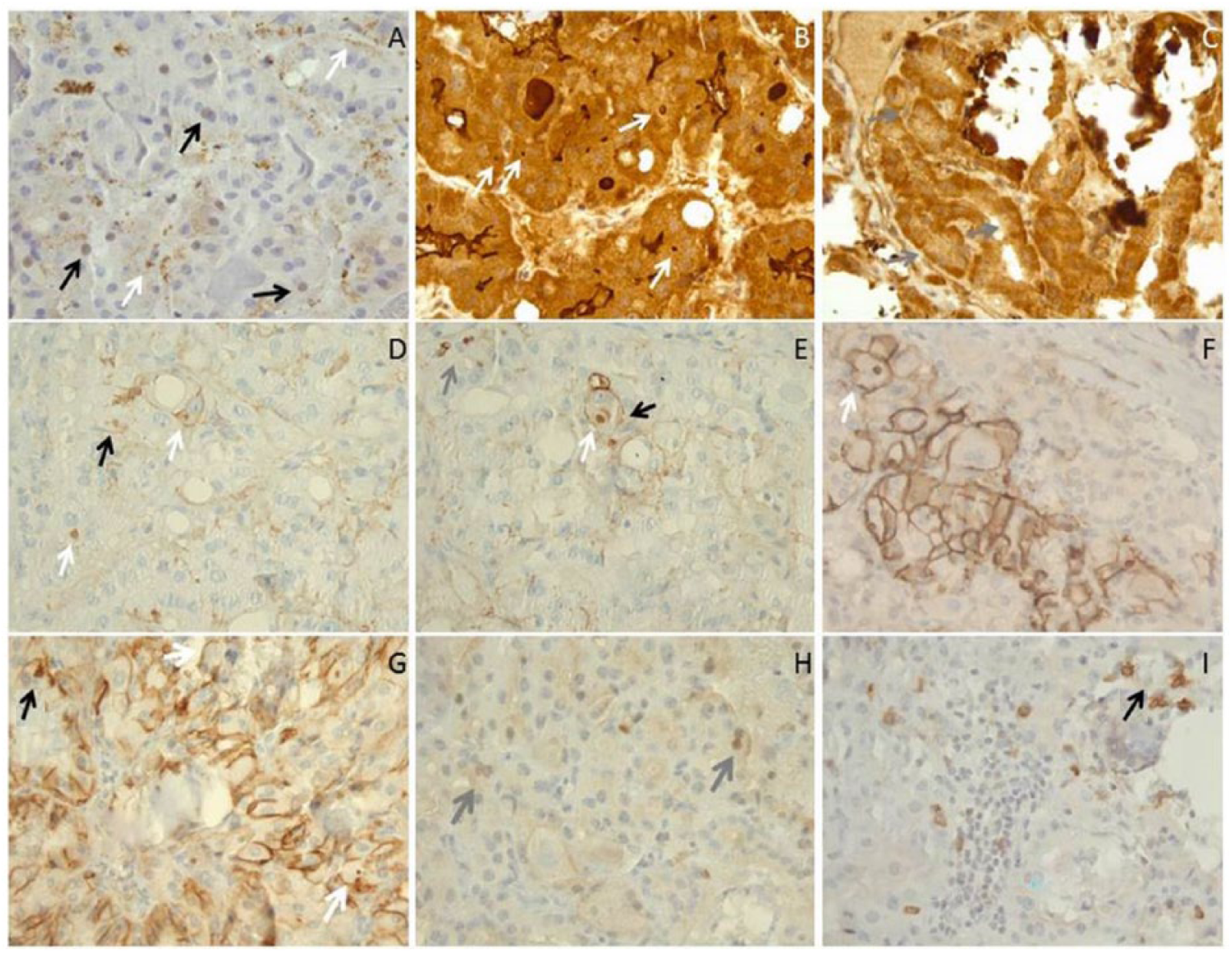
(A) Adipophilin was expressed in thyrocyte nuclei as well as in cytoplasmic granules (black and white arrows, respectively) (A). TIP47 showed a diffuse cytoplasmic expression, microgranular and dot-like (B: white arrows). A focal heterogeneous intracytoplasmic staining was also noted (C: gray arrows). CD138 was expressed in pericalcification cells, the membrane expression showing focal heterogeneity, with presence of dot-like structures (D and E: black arrows for membrane staining, white arrows for dot-like staining). Nodule thyrocyte nuclei were positive for CD138 (gray arrow). CD56 was expressed more frequently in a membrane pattern than in a cytoplasmic pattern (F and G: white and black arrows, respectively); however, positive in cytoplasmic granules or dot-like structures. To note would be the presence of several binucleated cells H and I: gray arrows CD25 expression was nuclear in nodule thyrocytes (H and I). Sparse lymphocytes and mastocyte-like cells were positively stained (black arrows).
Discussion
Here, we report a rare type of OTA, characterized by the presence of numerous psammomatoid calcifications, focally confluent resulting in macrocalcifications. To mention would be that macrocalcifications, easily detectable on imaging procedures, are considered more frequent in benign thyroid lesions. Another point of interest would be the morphological heterogeneity of microcalcifications observed not only in the colloid but also in the cytoplasm, 5 reminiscent of mitochondrial calcifications. Mitochondrial calcifications as detected by electron microscopy are reported in neoplastic cells, such as in bowel carcinoma 6 and synovial sarcomas. 7 The histogenesis of this type of calcifications in tumors is difficult to elucidate. A local cause as, eg, an abnormal blood supply may result in ischemia- or hypoxia-related calcifications. The latter type of calcifications is reported for damaged rabbit myocard cells after anoxic hypoxia. 8 Abnormal blood supply may also result in degeneration-related calcifications appearing as granular aggregates in neoplastic cells besides in degenerated hepatic and myocardial cells. 6 In the case we report, the hypothesis of a local cause of calcifications could be more plausible than a systemic cause. A calcific disease was ruled out based on the normal calcium levels and renal function tests. However, small calcifications of the elastic lamina of perithyroid vessels, age-related or not, were detected in the perithyroid tissue. The hypothesis of tumor-related acidosis associated with an active Warburg phenomenon remains to be further investigated. Consistent with the occurrence of tumor acidosis would be the expression of Bcl2 in most of the nodule thyrocytes, an acidic culture being associated with Bcl2 increase.9,10 Whether acidosis may be related also to changes in cell membrane characteristics as, eg, a discontinuous membrane expression pattern of CD56 and CD138 as seen in the studied case and be initiators of the pro-calcification process remains to be further investigated.4,5
The second peculiarity of the present case consisted in the presence of clear-cell change, already reported in thyroid nodules, mainly of carcinoma type.11–14 Interestingly, the clear cells did not express the anti-mitocondria antibody, the clear-cell change being suggestive rather of the granular vesicular swelling/balooning and cytoplasmic paraptosis sequence. 15 Kniseley and Andrews 16 reported loss of clear-cell appearance after administration of large doses of dessicated thyroidal substance and the association of clear-cell structure with enhanced concentration of I131. The heterogeneous expression with focal lack of cytoplasmic thyroglobulin in several nodule thyrocytes, in agreement with the observations of Kniseley and Andrews, 16 sustains the hypothesis of a necrobiotic-type change. Interestingly, markers of intracytoplasmic lipid-droplets adipophilin (already reported for oncocytic adrenal adenomas) 17 and TIP47 were expressed in the nodule thyrocytes including those with clear-appearing cytoplasm. This observation was not surprising, lipid droplet–mitochondria complexes being detectable in NIH3T3 fibroblasts. 18 Moreover, the diffuse expression of TIP47 we have observed in this oncocytic nodule is in agreement with the reported protector role of mitochondria integrity. 19 Interestingly, adipophilin showed nuclear expression as well as CD25 and CD138. While a nuclear translocation is reported for CD138, 20 the precise background of nuclear expression in thyrocytes of adipophilin and CD25 remains to be deciphered.
In conclusion, we report a rare type of OTA, peculiar by the presence of numerous psammomatoid calcifications and macrocalcification and by the presence of clear-cell change. Heterogeneity in membrane CD56 and/or CD138 expression as well as cytoplasmic heterogeneity of Bcl2 and lipid-droplet marker TIP47 are possibly relevant for calcification and clear-cell change, requiring further investigation.
Footnotes
Acknowledgements
The authors thank Pr M Sasaki, Pr R Katoh, Pr MG Siriois, G Balmus, R McIntyre, D Adams, K Schenke-Layland, C Coutin, M Dubois (Ozyme), S Rakel, and C Sayadian (Abcam) as well as B Mechekour, the NCA/Avicenne, BIUM, and CDMP/APHP teams.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
AHL data collection, analysis and writing of the manuscript. GB analysis and writing of the manuscript. BS analysis and writing of the manuscript.