
Abstract
Objective:
To provide data on the standard anatomical dimensions and configuration of labia minora in a cohort of women, who perceive their external genitalia as entirely usual.
Methods:
This is a Cross-sectional Prospective study where 207 women, subjectively free of any physical or objective symptoms related to their external genitalia, were enrolled over six months from the outpatient of the Department of Obstetrics and Gynecology (OBG) of a tertiary care hospital in the southern part of India, after taking their informed consent. The measurements of their labia minora, and a note of its gross external appearance, were taken using a disposable wooden caliper with graduations. Labia minora length and width were measured on both sides, and a mean of the two measurements was taken. We also noted the relation of the labia minora with the level of the labia majora: under or within, or beyond, including its color compared to that of the adjoining areas, and the presence or absence of rugosities in labia minora.
Results:
The width of the labia minora (mean) was 15.72 +/− 6.83 mm (maximum 48 mm and minimum 5 mm, range 42 mm). The mean labia minora length was 4.41 +/− 0.86 cm (maximum 8 cm, minimum 1.5 cm, range 65 mm).
Conclusion:
The standard measurements of labia minora vary widely. The study provides baseline measurements of labia minora for South Asian women, which can be used as a reference range to counsel women regarding ‘normality.’ These data can be helpful in women presenting for cosmetic gynecology surgeries and other surgeries on external genitalia.
Introduction
The normal appearance of female external genitalia has been a matter of debate, and the data regarding the standard anatomical dimensions of the vulva is scarce. A study done in 2013 stated that none of the medical textbooks available described the standard measurements of the vulva satisfactorily. 1 The knowledge regarding the normal size and appearance of the vulva is lacking even in general practitioners and the patients themselves.2,3 While the lack of knowledge in the patients leads to unnecessary consultations in a desire to achieve ‘normality,’ that in the practicing physicians and gynecologists is manifested by more and more referrals to specialists in the field. This referral, by some patients, is perceived as proof that something may be ‘abnormal’, for which they need a specialist consultation, further reinforcing their belief and anxiety.
Female Genital Cosmetic surgery (FGCS) includes any surgical procedure performed on the female external genitalia with a deliberate intent to alter its external appearance, usually without an apparent physical or functional medical requirement for the same. 4 It includes procedures like labiaplasty (the surgical reduction/correction of labia minora), perineoplasty (tightening of the vaginal opening), clitoral hood reconstruction (sometimes also indicated in cases of congenital adrenal hyperplasia), vaginoplasty, hymenoplasty (surgical restoration of the vaginal membrane), vulval lipoplasty (smoothening of vulva or mons pubis and upper portions of labia majora by removal of unwanted fat), and G-spot augmentation through lipofilling or injection of synthesized human collagen. One of the most popular and widely practiced cosmetic gynecology surgeries is labiaplasty, which is characterized by surgically reducing the labia minora, so that they come at the level of, or are completely hidden by, labia majora. 5 Although initially the procedure was indicated for labia minora hypertrophy, nowadays, it is mainly undertaken for cosmetic indications. The problem here is that the perception of ‘normal,’ is influenced by several factors, including culture, photographs shown on media or social platforms, opinion of friends, family, sexual partners, and sometimes even on the opinion of health care professionals. Although several classification systems, describing the normal and abnormal appearance of labia minora and labia majora are currently in place, none has attained widespread acceptance. The current most important indication of doing labiaplasty is an ‘abnormal vulva’. This makes it very important to define what is normal. The normal threshold or cut-off value to label labia minora as ‘abnormal,’ and therefore needing corrective surgery, should be clearly defined. 6
The perception of beauty has also seen seasonal and timely variations worldwide due to developments in fashion and technology. Given the lack of validated standard data, any deviation from an ideal appearance has a probability of being identified as abnormal, therefore needing surgical repair to achieve ‘normality’ and perfection in appearance or function. The present study has been planned to address the gap in our knowledge regarding normal labia minora measurements. The aim is to provide standard anatomical dimensions and configuration of the labia minora in a cohort of women, who perceive their external genitalia as completely ‘normal.’
Material and Methods
This Cross-sectional Prospective Study was carried out in the Department of Obstetrics and Gynecology (OBG) of a tertiary care hospital in the southern part of India, after taking approval from the Institutional Ethical Committee (IEC). The data presented in the study are from an individual center, but a part of an ongoing larger study ‘Anatomical measurements of Vulva and Vaginal length for an Unselected Indian population: A Multi-centric Cross-sectional Prospective Study.’ Women were recruited from the outpatient department of OBG. The source population was all women visiting OBG outpatient department for any complaint other than those related to appearance or physical discomfort relating to the external genitalia. Women aged more than 18 years, who had not attained menopause and subjectively perceived their vulva as completely normal were included in the study population.
A detailed history was taken to assess whether these women had any complaints regarding their vulval appearance or function. These included complaints like discomfort when wearing undergarments or body-hugging tight clothing, difficulty or pain during intercourse or experiencing any form of uneasiness while engaging in sports activities such as cycling, or complaints like feeling uneasy or awkward, or any type of psychological complaints such as feeling uneasy when intimate with the sexual partner. Women less than 18 years, post-menopausal women, or unwilling to participate in the study were excluded. Women with any history suggestive of surgery or radiotherapy in the genital region that could modify the regular measurements of the external genitalia, women with genital prolapse, chronic vulval disease, or those with congenital malformation of the external genitalia and lower reproductive tract were also excluded. All participants were explained in detail the examination protocol, and written informed consent was taken.
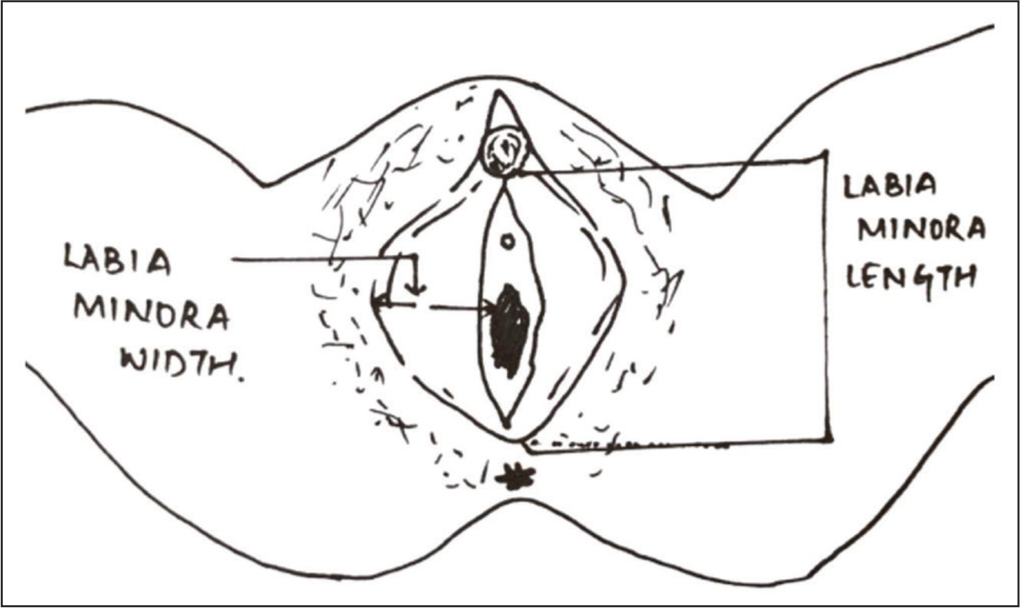
After a brief interview of the study participants regarding their age, occupation, and education status, a record of their height, weight, and body mass index (BMI) was taken. The participants were then asked to lie on the examination table in a lithotomy position to take their genital measurements. External genital measurements were done using a disposable wooden caliper with graduations, measuring 1/10 mm, as shown in Figure 1. The measurements were taken by the first and second authors only to ensure uniformity and avoid inter-observer variations. The principal investigator ensured standardization of the measures by supervising the first ten measurements done by the co-investigator. The template in Figure 1 was used for the genital measurements, which were taken according to the following definitions. LMn width was defined as the length from the base of the labium minora to the widest lateral prominence and LMn length as the longest craniocaudal length of the labium minora. 7 LMn length and width were measured bilaterally, and a mean of the two measurements was taken. A note was also made of the visibility of the LMn: under or within, or beyond the level of the labia majora, its color compared to that of the adjoining areas, and the presence or absence of rugosities in LMn.
Template Used for the Measurements of Labia Minora Length and Width.
Statistical Analysis
The data collected were entered into a Microsoft Excel sheet and analyzed by SPSS 21 version software (SPSS Inc., Chicago, IL, USA). Categorical data were described by number, frequency, relative frequency or proportion, mean +/− standard deviation, and interquartile range. To find out whether the collected data were distributed normally or not, Kolmogorov- Smirnov test was used. Box and Whisker plots have been used to display variation in the normal anatomical measurements of the study population. Quantitative variables between the study groups were compared using the Mann–Whitney U test and the Kruskal–Wallis test. A probability value (P value) less than .05 was considered statistically significant.
Results
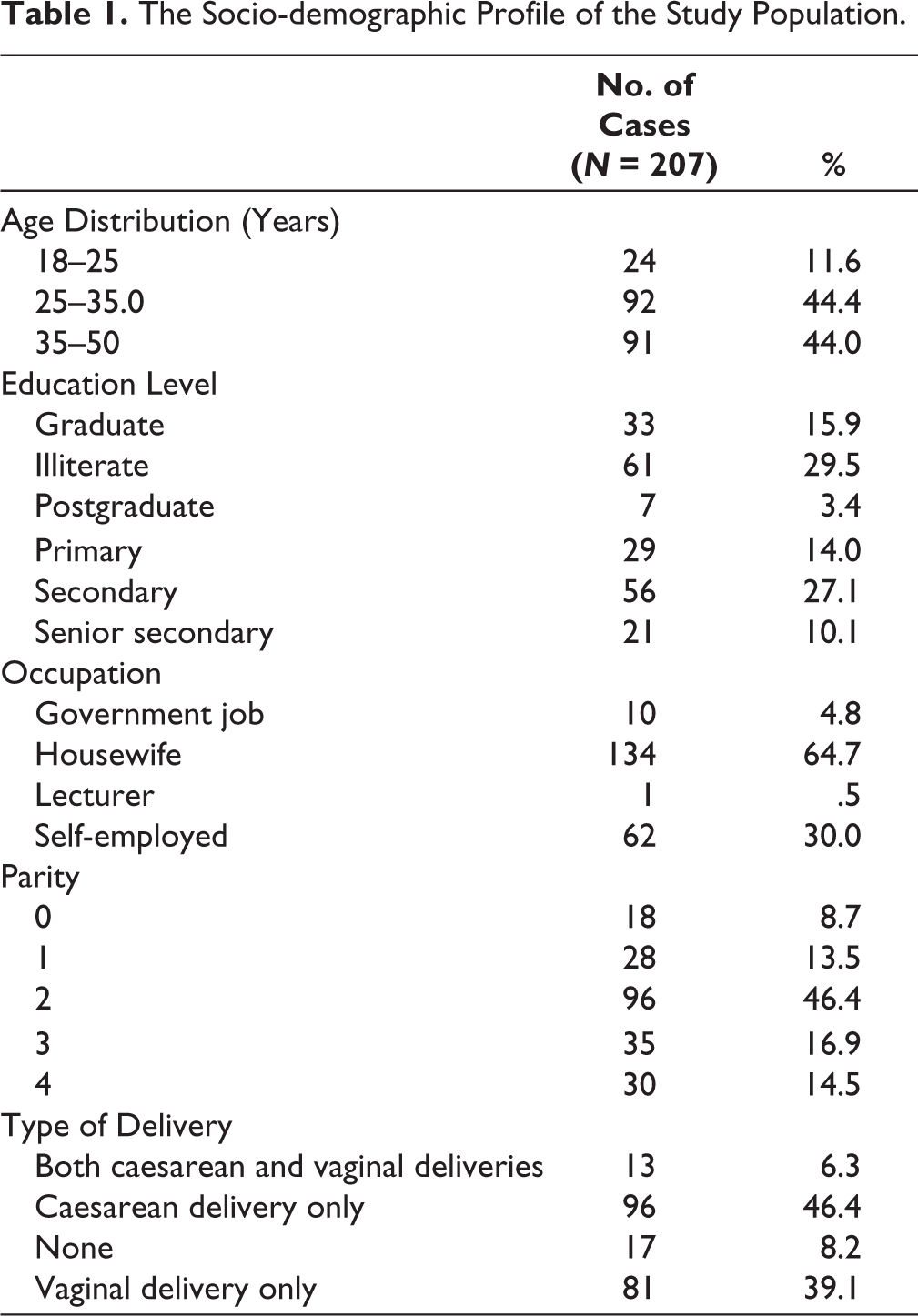
A total of 207 females participated in the study over six months, from January 2022 to June 2022. The socio-demographic profile of the study participants is described in Table 1. All women were premenopausal, with ages ranging between 20 and 48 (mean age 34.51 +/− 8.13 years). The study population’s mean height, weight, and body mass index (BMI) were 152.82 +/− 5.75cm, 57.106 +/− 10.84 kg, and 24.57 +/− 4.21, respectively.
The Socio-demographic Profile of the Study Population.
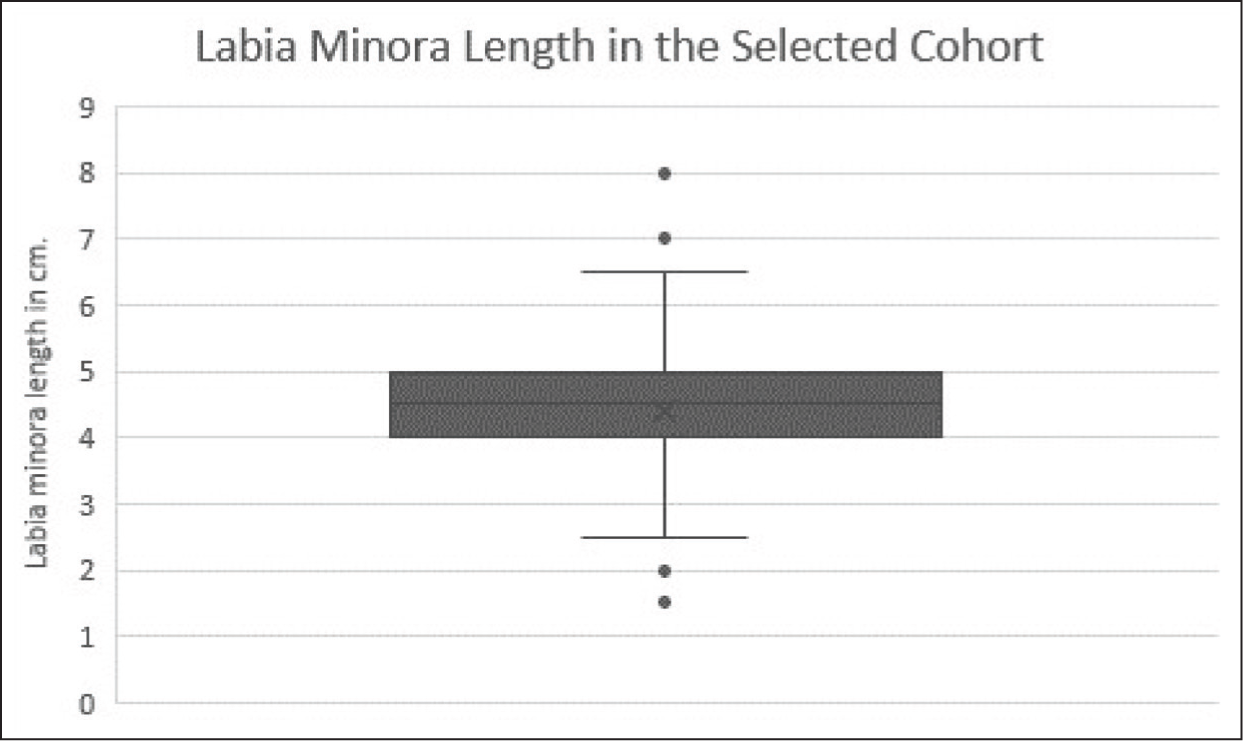
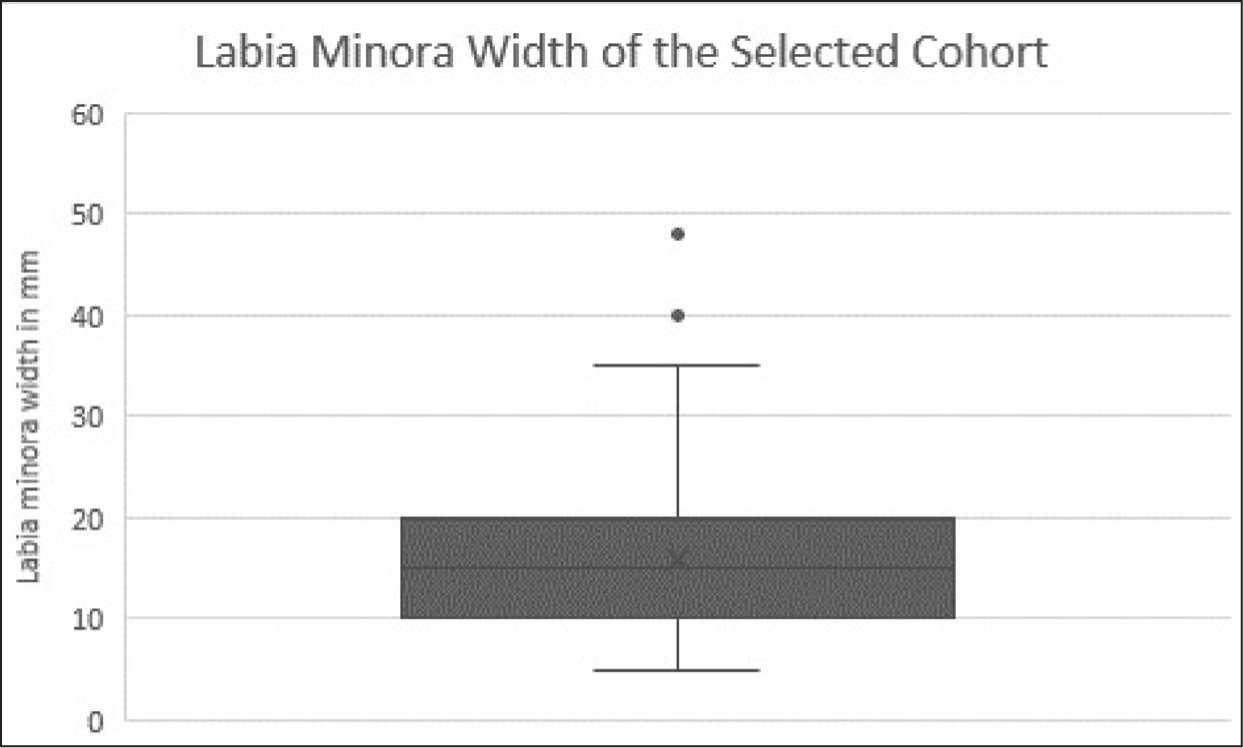
The anatomical measurements of LMn and its characteristics are summarized in Table 2. Figure 2 and Figure 3 demonstrate the normal anatomical variation of labial measurements in women who have no complaints regarding the anatomy and no physical complaints regarding their vulva. The mean LMn width was 15.72 +/− 6.83 mm (maximum 48 mm and minimum 5 mm, range 42 mm). The mean LMn length was 4.41 +/− 0.86 cm (maximum 8 cm, minimum 1.5 cm, range 65 mm). The 5th and the 95th centiles are mentioned in Table 2.
Anatomical Length Measurements of ‘Normal’ Labia Minora in South Indian Females.
Anatomical Width Measurements of ‘Normal’ Labia Minora in South Indian Females.
‘Normal’ Anatomical Measurements of Labia Minora in the Study Cohort.
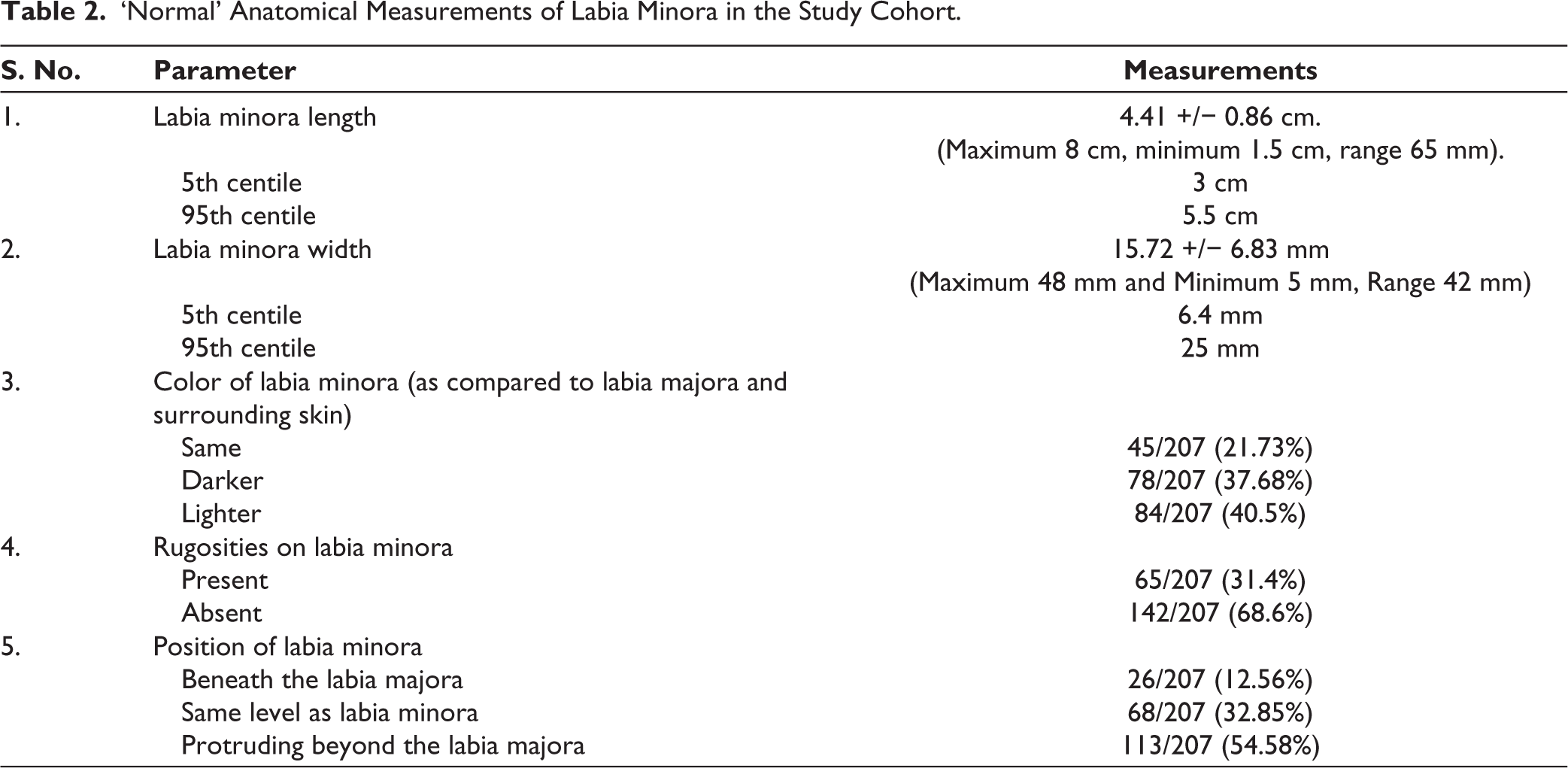
There was no statistically significant correlation between the LMn length and width with age. However, a positive correlation was found between the length of LMn and weight (r = 0.154, P = .027), BMI (r = 0.151, P = .030), and parity (r = 0.163, P = .019). A positive correlation was also observed between LMn width and parity (r = 0.150, P = .031). LMn length and width also had a positive correlation (r = 0.305, P = .00).
Discussion
Labia minora is mucocutaneous folds lying medial to labia majora. They form the boundaries of the vaginal vestibule. They lack hair but have abundant sebaceous glands, elastic fibers, and blood vessels. Because of these anatomical characteristics, they form erectile tissue, quite similar to the penis in males. 7 An ideal or ‘normal look of labia minora is, till now, a matter of debate. Some authors say that the labia minora should be small in size and should not protrude beyond the labia majora; others consider that an ideal labia minora sits flush with the labia majora.8,9 The definition of an ‘ideal vulva’ and thus ‘ideal labia minora’ lacks standard criteria, making it subjective and, to a large extent, dependent on the discretion of the surgeon or patient.
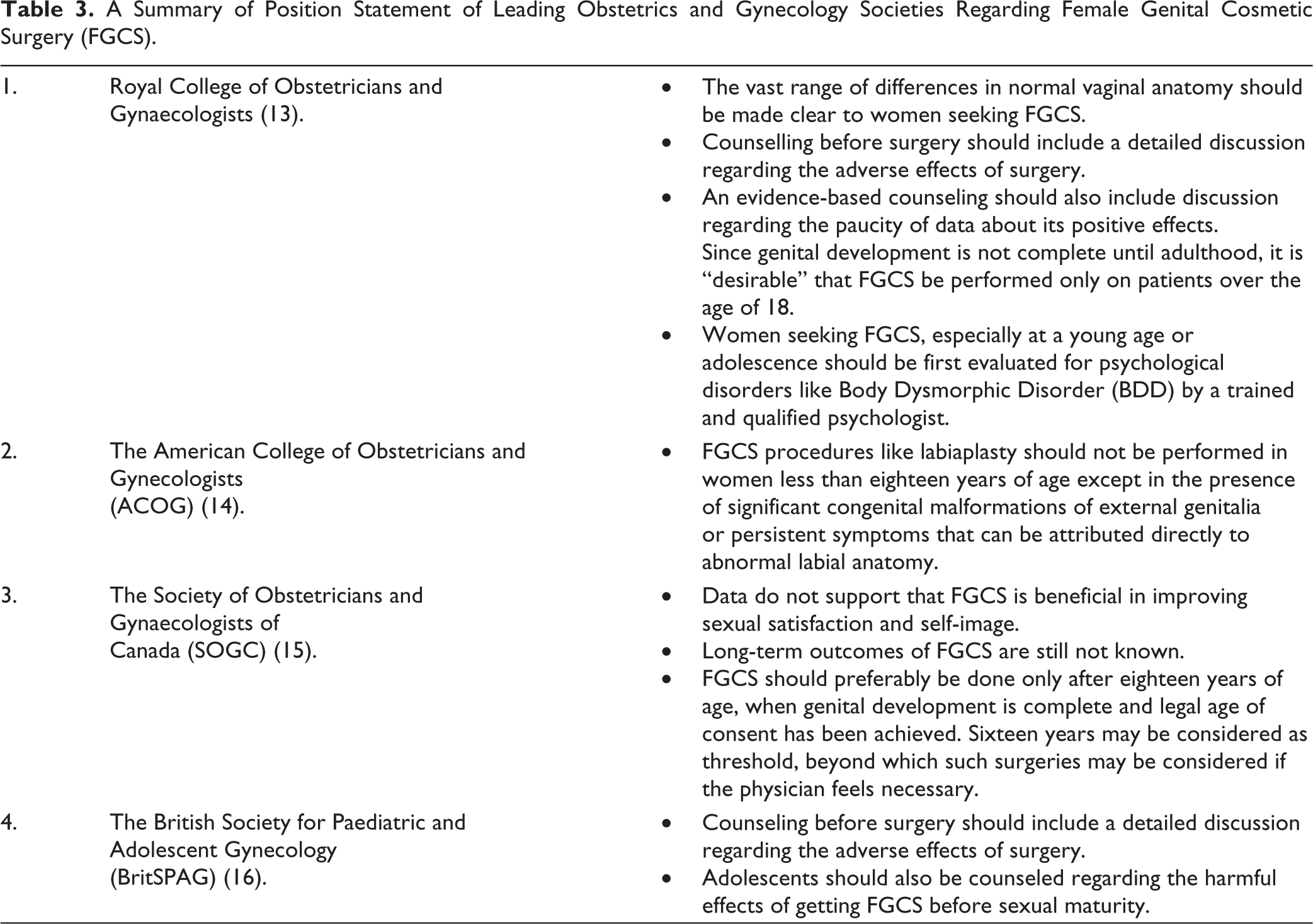
Labiaplasty, one of the favorite procedures to achieve a ‘normal’ vulva, has seen tremendous demand in recent years. According to a recent report published by the American Aesthetic Plastic Surgery National Databank, FGCS generated a revenue of approximately nine billion dollars in 2020. This is surprising, considering that this was when the coronavirus pandemic was near its peak. There were restrictions on surgical procedures, being restricted to only emergencies in a few countries. A total of 13,697 labiaplasties were performed during this time. 10 This number demonstrates an increase compared to 12,903 and 9945 labiaplasties completed in 2019 and 2015, respectively. However, it is important to understand that these numbers may be misleading and an actual underestimate because women seeking surgeries at private centers may not be reported. The decision to undergo a surgical procedure just for cosmetic reasons should be undertaken only after having complete knowledge regarding all its pros and cons. Before going for such procedures, a well-informed decision is a must. Any surgical procedure is not wholly free of the risk of complications. Genital or cosmetic gynecological surgery to achieve the so-called ‘ideal genitalia’ comes with a risk of damage to underlying nerves and blood vessels of the perineal region, which can lead to impaired sensation in the genital region and even affect the future capacity for sexual pleasure.11,12 The prerequisite for proceeding for FGCS, both for the patient and the performing surgeon should be that they have a clear understanding of variations in normal appearance. The cases chosen for FGCS should be the ones, which differ markedly from normal. The recommendations of leading scientific societies in obstetrics and gynecology are summarized in Table 3.13-16 Almost all, unanimously recommend that these procedures should preferably be avoided in women less than 16-18 years of age, and should always be done after giving due consideration to their side effects.
A Summary of Position Statement of Leading Obstetrics and Gynecology Societies Regarding Female Genital Cosmetic Surgery (FGCS).
Enormous variations in the size and measurements of female external genitalia have also been highlighted in several previous studies. In reproductive-age women, without any vulvar or sexual complaints, the width of the labia minora was found to range between 7 mm to 50 mm. 17 Women considering FGCS should be aware of this wide variation in the normal range. Surgeons should help their patients make an informed choice regarding whether or not to proceed with the procedure. Authors believe that a significant proportion of women who approach the cosmetic gynecology specialist surgeon would decide against the procedure if they are reassured that their external genitalia is completely normal and if counselled in an evidence-based manner, with normative datasets.
The present study is probably the first to publish the average measurements of LMn in the south Indian population. The authors could find just one more study that has studied the same for the north Indian population. These data are fundamental because racial and ethnic factors significantly impact the measurements of the vulva and vagina for a given population sample. These data will be instrumental in counseling the patients seeking medical advice for ‘abnormal vulva’ or ‘labial abnormalities.’ Practicing gynecologists can use this as a reference range to guide women and young girls regarding normality. Further, many patients also have concerns about whether the outcome was aesthetically favorable after a surgical procedure on the vulva, like labial cyst excision or simple or radical vulvectomy. Knowledge of normal anatomical measurements is helpful when planning reconstructive or transgender surgery. 18
Our study found that the mean LMn width was 15.72 +/− 6.83 mm (maximum 48 mm and minimum 5 mm, range 42 mm). The mean LMn length was 4.41 +/− 0.86 cm (maximum 8 cm, minimum 1.5 cm, range 65mm). The data regarding white women was published by Kreklau et al. in 2018. 19 This study’s normal anatomical measurements of the vulva were length 4.21 +/− 16.35 and width 14.15 +/− 7.63 mm. A comparison of the two populations shows that the standard dimensions of the vulva in white women and South Asian women are not significantly different. However, if we compare these values for the North Indian and South Indian populations, there is a significant variation. A recent study published by Agarwal N et al. in 2021 found normal LMn length as 4.8 +/− 1.03 cm and width as 2.6 +/− 0.74 cm. 20 An important observation in setting up a reference range for the selected cohort was the outliers detected in the data set regarding labial measurements. The authors acknowledge that the sample size of the population was not large enough to comment on the ‘normality’ of these outlier values. However, it is essential to note that women with these grossly different measurements too perceived their vulva to be completely normal.
Although it is not uncommon to find the persistor group in patients seeking gynecologic cosmetic surgery, the normal reference range, especially of a cohort of women who perceive that their external genitalia is entirely normal concerning appearance and measurements, can be very useful in counseling. Accurate knowledge of anatomical measurements of the female external genitalia, including the vulva, is required for various reasons, including designing and shaping medical and surgical equipment necessary for examination and surgical procedures. The following medical devices would be directly impacted by accurate or inaccurate anatomical data regarding the female vulva: speculum, douche, intrauterine devices, uterine sound, endometrial biopsy curette, vaginal dilators, vacuum-assisted delivery device, catheters, menstruation products, vaginal retractors. 3
In Western literature, a significant focus has been on the growing trend of cosmetic labiaplasty, largely driven by media portrayals of a narrow “ideal” vulvar aesthetic. Research in these regions suggests that women often experience heightened body dissatisfaction, anxiety, and a distorted sense of normalcy due to unrealistic beauty standards that emphasize smaller labia minora. Studies have also pointed to a high rate of mental health distress among women seeking labiaplasty, often influenced by societal and pornographic representations.21,22 In this context, anatomical diversity is often viewed as problematic, leading to a normalization of surgical interventions that may not be medically necessary but are fueled by aesthetic ideals. In many South Asian communities, the discourse surrounding women’s bodies, including their genital anatomy, has historically been more private or even taboo, leading to limited awareness and openness about anatomical diversity.23,24 The findings of the present study advocate for a broader recognition of natural anatomical variations, challenging the influence of both Western beauty standards and traditional taboos. This contrasts with Western research by focusing on how embracing diversity within a cultural context can reduce the mental health burden that often stems from unrealistic beauty expectations or social pressures. Furthermore, the mental health impact in South-Asian contexts may not be as directly linked to cosmetic surgery but could instead be influenced by cultural stigma, leading to feelings of shame, anxiety, or inadequacy when faced with societal expectations of “proper” female anatomy.
In cultures where rigid beauty and body norms persist, women may experience significant mental health implications, including body dysmorphia, anxiety, and low self-esteem.21-24 The normalization of diverse labial dimensions through the present research can empower women to embrace their individuality, reducing feelings of inadequacy or shame. Furthermore, the study may help dispel misconceptions perpetuated by media and cultural narratives, fostering a healthier self-image among women and encouraging acceptance of their bodies as natural and unique. The findings of the study could also have broader implications for mental health within medical and societal contexts. A greater understanding and acceptance of anatomical variations may prompt healthcare providers to adopt more compassionate and patient-centered approaches, thereby mitigating the psychological distress that arises from stigmatization or unnecessary medical interventions, such as cosmetic labiaplasty. Additionally, by promoting education and awareness, the study may serve as a catalyst for open conversations about female anatomy, reducing stigma and enabling women to seek support for related mental health concerns without fear of judgment. Overall, the study underscores the interconnectedness of anatomical awareness, cultural perceptions, and mental well-being.
Study Limitations
The present study is the first to provide the reference range for the South Indian population, but it had certain limitations. Firstly, the sample size was small. One of the reasons for this was that females in this part of the world are very conservative and usually reluctant to give consent about any study involving measurements of external genitalia. Secondly, this is a hospital-based study, where only patients visiting the gynecology outpatient department due to any gynecological complaint were included for data collection. Thirdly, since our study was conducted only on Indian women residing in the southern part of the country, measurements from other parts of the country and other countries are needed to evaluate racial differences. Studies with larger sample sizes in the community with structured tools assessing the actual perceptions of women, their external genitalia, and their corresponding measurements are required.
Conclusion
The standard measurements of Labia Minora vary widely. The study provides baseline measurements of Labia Minora for South Asian women, which can be used as a reference range to counsel women regarding ‘normality.’ These data can be helpful in women presenting for cosmetic gynecology surgeries and other surgeries on external genitalia.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all of the patients who opted to take part in the study; without them, the study would not have been possible. We also thank the nursing personnel for their assistance with the study during the usual OPD hours.
Author Contributions
Concept: MM, SRR, SKS, RM, AJ, NP.
Design: MM, SRR, SKS, RM, AJ, NP.
Data Collection or Processing: MM, SRR, SKS, RM, AJ, NP.
Analysis or Interpretation: MM, SRR, SKS, RM, AJ, NP.
Literature Search: MM, SRR, SKS, RM, AJ, NP.
Writing: MM, SRR, SKS, RM, AJ, NP.
Critical review: MM, SRR, SKS, RM, AJ, NP.
Approval of final manuscript: MM, SRR, SKS, RM, AJ, NP.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This work was approved by the Institute Ethical Committee (IEC) of our Institute [Approval Number: AIIMS/BBN/IEC/DEC/2021/136, dated: 22 December 2021].
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was taken from all involved women.
Peer Review
Externally peer reviewed.