
Abstract
Clinical models of sexual response link anxiety to the etiology of sexual dysfunction. Furthermore, some cognitive behavioral therapies (CBTs) for sexual dysfunction have included strategies targeting anxiety reduction. This review examines the experimental literature on the effects of manipulating aspects of the anxiety response (e.g., anxious sensations, thoughts, attentional focus) on genital and self-reported sexual arousal. An additional aim was to use this literature to elucidate potential mechanisms that may be useful for CBT for sexual dysfunction. Our review suggested that anxiety sometimes facilitates, inhibits, or has no effect on sexual arousal. These findings suggest that caution is warranted incorporating anxiety-focused interventions in the treatment of sexual dysfunctions. Importantly, little experimental research has utilized precise manipulations of anxiety (e.g., manipulating fear of penetration) that are related to current CBT interventions. To better understand the relationship between anxiety and sexual dysfunction, future research should explore the question of why and how anxiety exerts a variable effect on sexual arousal rather than simply if anxiety exerts an effect on sexual arousal. Importantly, experimental research examining individual differences in beliefs about anxiety and sex may be helpful in answering this important question and help advance and improve CBT interventions for sexual dysfunctions.
Researchers have long conceptualized anxiety as a central factor that can interfere with all phases of the sexual response cycle (i.e., sexual desire, arousal, and orgasm; American Psychiatric Association, 2013) and contribute to pain associated with sexual activity and/or the inability to experience vaginal intercourse (i.e., genito-pelvic pain/penetration disorder 1 ; American Psychiatric Association, 2013). Researchers and clinicians have typically regarded anxiety-related physiological sensations, thoughts, and behaviors as likely etiological factors in the development, maintenance, and exacerbation of sexual dysfunction. Therefore, principles of cognitive behavioral therapy (CBT) guide some of the most common interventions to address sexual dysfunction by focusing on the reduction of anxiety, fear, and avoidance (e.g., ter Kuile, Both, & van Lankveld, 2010). However, there is also evidence that the induction of anxiety can both inhibit and facilitate sexual arousal (e.g., Barlow, Sakheim, & Beck, 1983).
Our initial intent in this article was to review the effects of anxiety on all stages of the sexual response to tease apart these conflicting theories and findings. However, as the majority of studies focused specifically on the effects of anxiety on sexual arousal, we opted to concentrate primarily on self-reported and genital sexual arousal. Thus, we reviewed the experimental research to elucidate the effects of the anxiety response on sexual arousal in both nonclinical and clinical populations with sexual dysfunction where possible. Our goal was to clarify the conditions under which anxiety may facilitate, inhibit, or have no effect on sexual arousal to make recommendations and inform the utility of CBT for sexual dysfunctions. To frame the literature review, we first provide a definition of how we define anxiety in this article. We then present the theoretical models that implicate anxiety in the etiology and maintenance of sexual dysfunction and follow with a brief discussion of the role of anxiety reduction in CBT for sexual dysfunction.
Working definition of anxiety
Generally, CBT models of psychopathology understand emotions like anxiety through the interaction of three factors: physiological sensations (e.g., the sensations associated with anxiety, such as increased heart rate and sweating), cognition (e.g., the beliefs and interpretations associated with the feared stimuli), and behavior (e.g., avoidance, safety behaviors, hypervigilance). In the current article, we also regard “anxiety” as an emotional process that is triggered within a context. As such, it can be elicited through a variety of antecedents. For instance, a person may experience anxiety during sexual interactions because he or she is afraid of not pleasing their partner or of not performing appropriately; a person may also feel anxiety relating to sexually transmitted infections during an unprotected sexual interaction; a person may feel anxiety about getting caught engaging in sexual activities. Anxious affect and cognitions are also likely to impact behavioral tendencies (e.g., avoiding sexual activity or focusing on size of erection). From this framework, the effects of anxiety on sexual arousal can be experimentally examined by manipulating components of the anxiety response (e.g., by inducing anxious arousal, affect, thoughts, or behaviors), ideally taking into consideration the context by which anxiety is induced.
Theories on the role of anxiety in sexual dysfunction
There are a number of theories and hypotheses about the role of anxiety in sexual dysfunction. From a physiological standpoint, Wolpe (1958) suggested that sexual arousal and anxiety may be mutually inhibitory because they are characterized by opposing nervous system activation—that is, sexual arousal by parasympathetic activation and anxious arousal by sympathetic activation. According to this theory, should two antagonistic responses such as anxiety and sexual arousal occur simultaneously, the stronger response (anxiety) would inhibit the weaker response (sexual arousal), resulting in decreased sexual arousal. However, research on the role of the sympathetic nervous system in inhibiting sexual arousal has produced conflicting results. Specifically, Meston and Heiman (1998) observed significant increases (not decreases as would be predicted by Wolpe’s theory) in genital arousal when they activated the sympathetic nervous system using ephedrine sulfate—an adrenergic agonist. Yet, they observed no effect on self-reported sexual arousal; thus, it is possible that the asynchrony between parasympathetic and sympathetic activations contributes to some aspects of sexual dysfunction but not others.
Masters and Johnson (1970) asserted that the root of sexual dysfunction was cognitive in nature. They proposed that anxiety associated with performance and self-monitoring (“spectatoring”) was incompatible with the ability to produce a sexual response sufficient for sexual activity. Barlow’s model (1986) was similar to Masters and Johnson’s in hypothesizing that sexual dysfunction is the result of cognitive interference. Specifically, in men with sexual dysfunction, increased autonomic arousal associated with anxiety is hypothesized to distract attention from erotic cues, thereby reducing or impeding sexual arousal and contributing to behavioral avoidance of sexual cues and sexual activity. Thus, Barlow integrated both cognitive and behavioral components. In contrast to Masters and Johnson (1970), Barlow (1986) also proposed that in men without sexual dysfunction, increased autonomic arousal associated with anxiety might actually facilitate sexual arousal through increased attention toward sexual cues. Thus, the effects of anxiety on sexual arousal may vary in clinical and nonclinical populations according to Barlow (1986).
The idea that anxiety might facilitate sexual arousal is consistent with Zillman’s (1983) excitation transfer hypothesis (i.e., residual excitation from one stimulus creates enhanced excitation to a second stimulus, which a person misattributes as originating from the second stimulus). In addition, Kempeneers and Barbier (2008) proposed that anxiety may not only enhance attention to sexual cues, but that people may misinterpret anxious arousal as sexual arousal, thereby enhancing sexual responsivity through both cognitive and physiological mechanisms. This misinterpretation could be explained by the overlapping bodily sensations present during sexual and anxious arousal (e.g., increased heart rate, sweating, racing thoughts) and likely depends on the context in which the sensations occur.
Janssen and Bancroft’s (2007; see also Bancroft, Graham, Janssen, & Sanders, 2009) dual control model of sexual response is the only model to date that proposes that sexual arousal and behavior are determined by the relative balance of central sexual excitation and sexual inhibition. In men, they identified two types of sexual inhibition: inhibition related to the threat of performance failure and inhibition related to the threat of negative consequences (Janssen, Vorst, Finn, & Bancroft, 2002a). They posit that high inhibition due to threat of performance failure, coupled with low sexual excitation, may contribute to sexual dysfunction. Thus, this model proposes that changes in physiological arousal, coupled with different cognitions, lead to the potential for sexual dysfunction. Although the authors do not equate inhibition to anxiety or fear, it is possible that fear and anxiety play a role in these types of inhibition given the prominence of threat. For example, a person who has high sexual inhibition in response to threats of performance failure and/or performance consequences could also experience feelings of anxiety when presented with the threatening situations (e.g., engaging in sexual activity when there is a chance of someone seeing, being concerned with losing arousal if intercourse does not occur right away). More research is needed to determine whether fear and anxiety may contribute to or be consequences of high sexual inhibition.
Cognitive behavioral treatments targeting anxiety in sexual dysfunction
Clinicians and researchers have used these theoretical frameworks and principles to inform CBT for sexual dysfunction. A comprehensive review of all cognitive behavioral interventions for sexual dysfunction is beyond the scope of this article (for systematic reviews, see Berner & Günzler, 2012; Günzler & Berner, 2012; for a meta-analysis, see Frühauf, Gerger, Schmidt, Munder, & Barth, 2013). However, it is important to note that common treatments for sexual dysfunctions often include strategies that target a reduction in fear of penetration, anxiety, and avoidance behaviors to increase sexual function through various cognitive behavioral mechanisms (i.e., physiological arousal, cognition, behaviors). These strategies or treatments consist of CBT for fear-related cognitions (e.g., van Lankveld et al., 2006), exposure therapy to target behavioral avoidance related to sexual activity common to sexual dysfunctions (one component of CBT for anxiety disorders; Abramowitz, Deacon, & Whiteside, 2012; ter Kuile & Reissing, 2014), and systematic desensitization via behavioral hierarchies of sexual activities where the goal is to reduce anxiety before moving on to the next step primarily for dysfunction related to arousal and orgasm (e.g., van de Wiel, Jaspers, Schultz, & Gal, 1990). Mindfulness-based interventions may also indirectly target anxiety in sexual contexts by increasing awareness of sexual responses, decreasing judgment toward these responses, and reducing the effect of distractions (e.g., by viewing them as mental events not necessarily needing to be attended to; Brotto & Basson, 2014).
CBT and related interventions are efficacious in the treatment of certain sexual dysfunctions including vaginismus, provoked vestibulodynia, and anorgasmia in women and premature ejaculation and erectile dysfunction in men (Berner & Günzler, 2012; Günzler & Berner, 2012; Molaeinezhad et al., 2014; ter Kuile et al., 2009; ter Kuile, Melles, de Groot, Tuijnman-Raasveld, & van Lankveld, 2013). However, research on the treatment of other sexual dysfunctions in women and men (e.g., female sexual interest/arousal disorder, hypoactive sexual desire disorder) is limited.
Although anxiety and fear are theoretically proposed to play a role in sexual dysfunctions, and treatment efficacy supports the use of CBT targeting relevant fears and anxiety, it would be useful to better understand the specific effects of anxiety on sexual arousal to identify specific mechanisms that can be targeted. There is some existing evidence for mechanisms of change in certain disorders. For example, reduction in coital fear among women with vaginismus is changed through addressing avoidance behavior (e.g., Melles et al., 2014; ter Kuile, Vigeveno, & Laan, 2007). Desrochers, Bergeron, Khalifé, Dupuis, and Jodoin (2010) found that higher levels of pain-related fear and catastrophizing prior to CBT predicted higher intensity of pain at follow-up in women with provoked vestibulodynia (i.e., recurrent pain with touch or pressure at vulvar vestibule). Together, these results suggest that targeting sex-related fears or anxiety may be beneficial in the treatment of some sexual dysfunctions. Reviewing the effect of other aspects of anxiety on sexual arousal may prove fruitful in determining whether anxiety should in fact be a target in the treatment of sexual dysfunctions. This topic is even more pertinent given that the interventions mentioned above frequently include multiple components, some of which are aimed at targeting anxiety and others that are unrelated to anxiety. Therefore, the contributing role of anxiety reductions in the overall treatment effects remains unknown.
Experimental research on the effects of anxiety on sexual arousal
Correlational studies investigating anxiety and sexual arousal have been informative and have inspired further research on the topic. Previous reviews of the role of anxiety in sexual arousal also exist (e.g., Seto, 1992). Here, we reviewed the experimental body of literature in which researchers manipulated aspects of the anxiety response (i.e., anxious sensations, anxious cognition, and behavioral responses to anxiety [e.g., distraction, avoidance]) in erotic contexts to identify potential targets for CBT intervention for sexual dysfunction. We expected that reviewing how the anxiety response was manipulated would help to highlight possible explanations for the mixed findings in the literature as discussed above. Our main objectives were to (1) understand the conditions under which anxiety inhibits and facilitates sexual arousal, (2) use this information to make recommendations regarding cognitive behavioral interventions for sexual dysfunction, and (3) highlight areas for future research based on Objectives 1 and 2.
Literature search strategies
Using PsycINFO, Medline, and Google Scholar, we searched for keywords relating to anxiety 2 paired with keywords relating to sexual function. 3 We also ensured that relevant research known to the authors was either represented or added to these results. 4 Next, we reviewed the reference list of selected articles for any additional references. We excluded literature reviews and correlational studies. This search strategy yielded 30 studies that used an experimental or mixed-experimental design.
The first and second author classified the studies into three overarching manipulation strategies: (1) manipulation using anxiety-provoking stimuli or sensations, (2) manipulation of performance demand, and (3) manipulation of attentional focus. Studies in which researchers used more than one manipulation strategy were reviewed in each relevant section. Given the potential utility of this review to inform clinical practice in the treatment of sexual dysfunction, we distinguished the experimental findings based on sample type (i.e., nonclinical or clinical) and participants’ gender. Table 1 provides a summary of the sample characteristics, methodological information (e.g., how the anxiety response was manipulated, how sexual arousal was measured), and outcomes of the reviewed studies. Genital arousal was generally assessed using penile plethysmography in men and vaginal photoplethysmography in women; whereas self-reported sexual arousal was assessed using a continuous scale. Though most researchers measured self-reported sexual arousal, occasional alternate types of self-report were used (e.g., sexual desire; Beck & Bozman, 1995). When reporting specific results, below we use the self-report term that was used by the original researchers, though our tables summarize these as self-reported sexual arousal. Table 2 provides a summary of results for genital arousal and self-reported sexual arousal (the main dependent variables examined across studies) for each anxiety response manipulation strategy.
List of reviewed studies and summary of variables and outcomes.
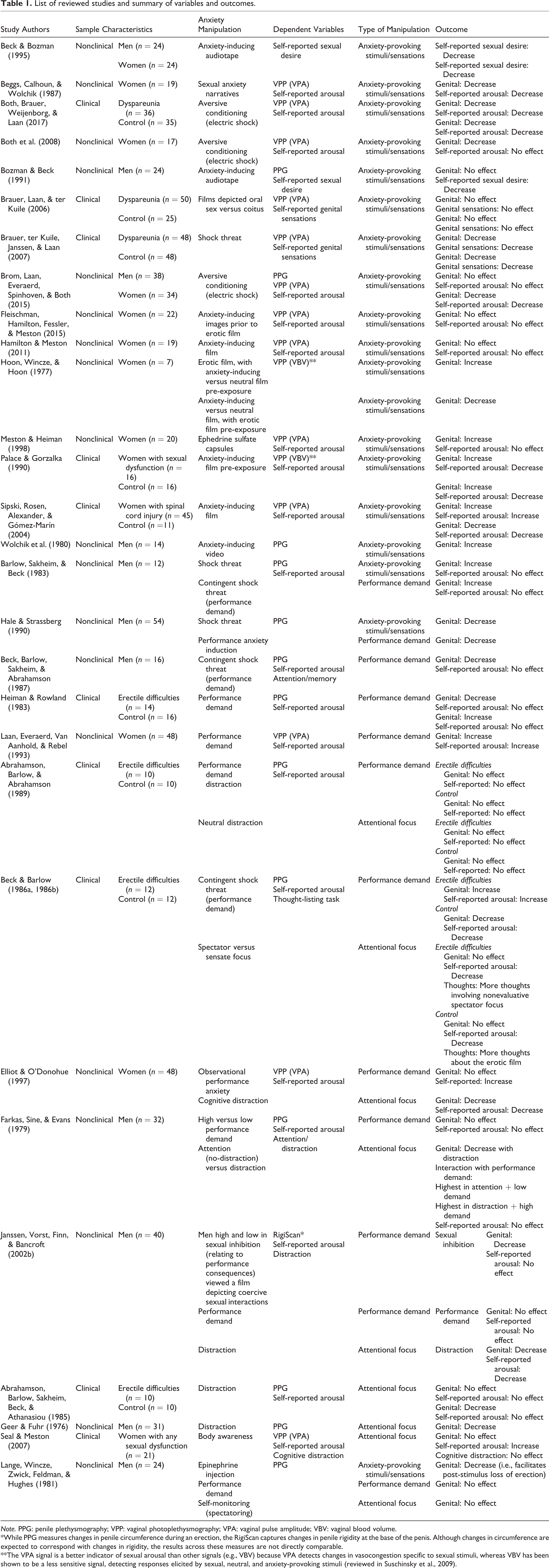
Note. PPG: penile plethysmography; VPP: vaginal photoplethysmography; VPA: vaginal pulse amplitude; VBV: vaginal blood volume.
*While PPG measures changes in penile circumference during an erection, the RigiScan captures changes in penile rigidity at the base of the penis. Although changes in circumference are expected to correspond with changes in rigidity, the results across these measures are not directly comparable.
**The VPA signal is a better indicator of sexual arousal than other signals (e.g., VBV) because VPA detects changes in vasocongestion specific to sexual stimuli, whereas VBV has been shown to be a less sensitive signal, detecting responses elicited by sexual, neutral, and anxiety-provoking stimuli (reviewed in Suschinsky et al., 2009).
Summary of results for genital and self-reported sexual arousal for manipulations using anxiety-provoking stimuli or sensations, manipulations of performance demand, and manipulations of attentional focus.

Note. Numbers in the table represent a compilation of the number of findings consistent with an increase, decrease, or no effect of anxiety on sexual response.
aClinical samples consisted of women with spinal cord injury (k = 1), dyspareunia (k = 3), and sexual dysfunction (k = 1).
bClinical samples consisted of women with spinal cord injury (k = 1), dyspareunia (k = 3), and sexual dysfunction (k = 1).
cClinical samples consisted of men with erectile difficulties.
dClinical samples consisted of women with sexual dysfunctions.
Anxious pairings: Manipulations using anxiety-provoking stimuli or sensations
As shown in Table 1, we found 18 studies in which researchers manipulated anxiety by using stimuli to provoke anxious arousal/affect and assessed the effect on sexual arousal in samples of men and/or women. In these studies, erotic stimuli were paired with (or primed by) a variety of anxiety-related stimuli, including shocks or shock threat, anxiety-inducing video or audio clips, epinephrine hydrochloride injections, ephedrine sulfate capsules, and stressful tasks. We begin by summarizing the main results of the studies in nonclinical and clinical samples of men and women, followed by a discussion of potential methodological factors that may explain discrepant findings.
Nonclinical samples
As shown in Table 2, an equal number of studies found that anxiety increased, decreased, or had no effect on men’s genital arousal. Fewer studies examined how anxiety affected men’s self-reported sexual arousal, with an equal number finding that anxiety decreased and had no effect on self-reported sexual arousal. None of the studies found that anxiety increased men’s self-reported sexual arousal.
More than half of studies demonstrated that anxiety decreased women’s genital arousal. However, in a few studies, anxiety increased or had no effect on genital arousal. The majority of studies indicated that anxiety decreased women’s self-reported sexual arousal, with a minority observing no effect. No studies observed a facilitative effect of anxiety on women’s self-reported sexual arousal.
Clinical samples
There were very few studies examining the effects of anxiety induction on genital or self-reported sexual arousal in clinical samples. As seen in Table 1, samples included women with various sexual dysfunctions, dyspareunia, or women with a spinal cord injury, which is often associated with decreased sexual functioning (Sipski, Rosen, Alexander, & Gómez-Marín, 2004). The results of these studies were mixed (see Table 2). Anxiety increased genital arousal in one study with a sample of women with various sexual dysfunctions (including anorgasmia, low sexual desire, and dyspareunia), but decreased genital arousal in three samples of women with dyspareunia. Most studies found that self-reported sexual arousal decreased under conditions of high anxiety in samples of women with either various sexual dysfunctions or dyspareunia. In women with spinal cord injury, genital arousal and self-reported sexual arousal increased under conditions of high anxiety.
Methodological considerations
There are a number of factors that may explain the variability in the results. First, in some studies, researchers induced anxiety simultaneously with erotic stimuli presentation (e.g., using shock threat, aversive conditioning, orally administered ephedrine sulfate, or audio narratives containing erotic and anxiety-inducing content), whereas in other studies, they induced anxiety prior to or following erotic stimuli presentation. In men, most studies that induced anxiety simultaneously found that genital arousal declined or was unaffected (Bozman & Beck, 1991; Brom, Laan, Everaerd, Spinhoven, & Both, 2015; Hale & Strassberg, 1990; Lange, Wincze, Zwick, Feldman, & Hughes, 1981), although Barlow, Sakheim, and Beck (1983) found that shock threat increased genital arousal in men. Self-reported sexual arousal did not seem to be influenced by simultaneous anxiety induction when the induction technique involved shock threat or aversive conditioning (Barlow et al., 1983; Brom et al., 2015), but self-reported sexual desire decreased when anxiety was induced via audio recording (Beck & Bozman, 1995; Bozman & Beck, 1991). In most studies with women, simultaneous induction of anxiety led to reduced genital arousal (Beggs, Calhoun, & Wolchik, 1987; Both et al., 2008; Brauer, ter Kuile, Janssen, & Laan, 2007; Brom et al., 2015) and self-reported sexual arousal (Beck & Bozman, 1995; Beggs et al., 1987; Both, Brauer, Weijenborg, & Laan, 2017; Brauer, ter Kuile, Janssen, & Laan, 2007; Brom et al., 2015, but see Both et al., 2008 for an exception). Only ephedrine as a physiological arousal induction technique seemed to affect genital arousal (increasing it) and self-reported sexual arousal (not affecting it) differently in women (Meston & Heiman, 1998).
In the few studies using a sequenced approach, researchers presented participants an anxiety-inducing stimulus (typically a film or audio clip), followed by an erotic stimulus (Fleischman, Hamilton, Fessler, & Meston, 2015; Hoon, Wincze, & Hoon, 1977; Palace & Gorzalka, 1990; Sipski et al., 2004; Wolchik et al., 1980). Only one study found that the anxiety induction increased genital arousal in men during the erotic film clip (Wolchik et al., 1980). Self-reported sexual arousal was not examined. In women without sexual dysfunction, anxiety pre-exposure either decreased or had no effect on both genital and self-reported arousal to erotic cues (Fleischman et al., 2015; Sipski et al., 2004). However, in women with spinal cord injury, anxiety pre-exposure increased genital and self-reported sexual arousal (Sipski et al., 2004). A third study found that anxiety pre-exposure resulted in increased genital arousal and decreased self-reported sexual arousal in women both with and without sexual dysfunction (Palace & Gorzalka, 1990). Hoon, Wincze, and Hoon (1977) also found an increase in genital arousal with anxiety pre-exposure in a nonclinical sample. However, both Palace and Gorzalka (1990) and Hoon and colleagues (1977) measured genital arousal through vaginal blood volume, which has been found to increase with sexual, neutral, and anxiety-provoking stimuli (reviewed in Suschinsky, Lalumière, & Chivers, 2009). Thus, the increase in genital arousal in these studies needs to be interpreted with caution. Given the limited number of studies in men and women on the effect of anxiety pre-exposure on sexual arousal and the contrasting findings, conclusions are again difficult to draw. Further research examining the effect of anxiety pre-exposure on sexual arousal is warranted, particularly in light of the hypothesis that anxiety sensations could “jump start” sexual arousal (e.g., Kempeneers & Barbier, 2008; Zillman, 1983). The only study to our knowledge to have examined the contrary, or the effect of anxiety post-exposure on genital arousal (i.e., presenting an erotic film followed by an anxiety-inducing film), found that inducing anxiety inhibited genital arousal more rapidly compared to when participants saw a neutral film instead (Hoon et al., 1977). Thus, the order in which individuals experience sexual arousal and anxious arousal may affect the response to erotic content. Finally, alternate explanations for the effect of anxiety manipulations, such as shock threat, should be ruled out. It is possible that a third variable, for example, distraction from sexual arousal, could conceivably play a role in some of the effects observed. 5
With respect to gender effects, most studies sampled either men or women and only two studies directly compared the effects of anxiety on men’s and women’s sexual arousal. Beck and Bozman (1995) induced anxiety by having participants listen to an anxiety-inducing sexually explicit audio recording and observed similar declines in self-reported sexual desire among women and men. In contrast, anxiety induced via aversive conditioning had no effect on men’s genital or self-reported sexual arousal, but decreased genital and self-reported sexual arousal in women (Brom et al., 2015). More research is needed to determine if anxiety affects sexual arousal and desire differently in men and women.
Summary
The effect of induced anxious sensations or affect on genital arousal in nonclinical samples of men is variable, whereas in women it appears to decrease genital arousal. In contrast, anxiety appears to exert a similar influence on self-reported sexual arousal in men and women. Research does not support the notion that anxiety will increase self-reported sexual arousal, but under some circumstances anxiety may decrease self-reported sexual arousal. To the best of our knowledge, no study has examined the effect of anxious sensations manipulations on sexual arousal in men with sexual dysfunction. In women with sexual dysfunction, the effect of manipulations of anxious sensations on genital arousal is variable. Self-reported sexual arousal appears to either decrease or not be affected by manipulations of anxious sensations in women with sexual dysfunction. Examination of methodological factors, furthermore, did not yield any clear-cut explanation for the variability in findings. Thus, it remains unclear under what conditions reducing general anxious sensations or affect will be beneficial for sexual arousal in men and women.
Manipulations of performance demand
We found 11 studies in which researchers manipulated performance demand (i.e., anxiety related to the need to achieve a certain level of sexual performance) to induce performance anxiety and observed the effect on sexual arousal. Most of these studies were with men (see Table 1), and there were no studies with both men and women. Surprisingly, we found few studies that manipulated other anxious cognitions (e.g., relating to the fear of penetration), despite the theorized importance of such cognitions in the treatment of many sexual dysfunctions (ter Kuile et al., 2010). Researchers used a variety of paradigms to manipulate performance demand, including shock threat contingent on size of erection, setting expectations or instructions relating to size of erection or level of arousal, indicating that the person was being observed, and self-ratings relating to size of erection. One study also used a mixed-experimental design by recruiting men high and low in “sexual inhibition.”
Nonclinical samples
As shown in Table 2, performance demand had variable effects on men’s genital arousal; however, the majority observed either a decrease or no effect. Most studies found that performance demand had no effect on men’s self-reported sexual arousal and no studies observed an increase in men’s self-reported sexual arousal. Performance demand appeared to either increase or have no effect on women’s genital arousal, and to increase women’s self-reported sexual arousal.
One mixed-experimental study compared the response to films depicting sexually coercive or noncoercive sexual interactions in men high and low in sexual inhibition relating to threat of performance consequences (Janssen, Vorst, Finn, & Bancroft, 2002b). Although self-reported sexual arousal was similar in both groups for both films, men high in sexual inhibition had weaker genital arousal to the coercive film compared to men low in sexual inhibition, supporting the inhibitory role of cognitive components of anxiety in genital arousal. These results are intriguing and may suggest that individual differences in sexual inhibition may explain the variability found in some studies.
Clinical samples
There were only three studies in which the effects of performance demand on sexual arousal in men with erectile difficulties were examined, each producing different outcomes on genital arousal (i.e., an increase, a decrease, and no effect on men’s genital arousal; see Table 2). Two of the three studies found that performance demand had no effect on men’s self-reported sexual arousal, whereas the third observed an increase in self-reported sexual arousal. We found no studies examining the effect of performance demand among women with sexual dysfunction.
Methodological considerations
The use of various paradigms across these studies may explain the variability in results. As seen in Table 1, many studies used shock threat contingent on size of erection; however, there were differences in the ways contingent shock threat was induced. For instance, Beck and Barlow (1986a) presented an actual example shock to participants. This may have reduced anxiety regarding what to expect from the shock. Moreover, in some studies, participants were told they had a 60% chance of receiving a shock (e.g., Beck, Barlow, Sakheim, & Abrahamson, 1987), whereas in other studies they were told they would definitely receive a shock (Hale & Strassberg, 1990). Therefore, the anxiety induced by contingent shock threat likely varied across these studies, producing different effects on sexual arousal (Hale & Strassberg, 1990). Contingent shock threat paradigms have not been used in samples of women.
Performance demand anxiety that was elicited verbally (e.g., telling participants they should expect to be highly aroused) did not affect genital or self-reported sexual arousal in men without sexual dysfunction (see Table 1). One study observed decreased genital arousal in men with erectile dysfunction. However, no change in self-reported anxiety was observed; thus, factors other than performance anxiety may explain this finding (Heiman & Rowland, 1983). Using different anxiety-inducing instructions, Hale and Strassberg (1990) found that telling men without sexual dysfunction that they had displayed subnormal genital arousal during a baseline measurement decreased genital arousal during a subsequent viewing of an erotic film. That is, at least in men, trying to perform optimally versus being told that their sexual performance is suboptimal may affect genital arousal differently. In women, performance demand instructions to try to be as aroused as possible during an erotic film or while engaging in sexual fantasy led to increased genital and self-reported sexual arousal, especially during the sexual fantasy (Laan, Everaerd, Van Aanhold, & Rebel, 1993). To our knowledge, there has been no research in which performance demand was manipulated by telling women participants that their level of arousal is suboptimal.
Abrahamson, Barlow, and Abrahamson (1989) used another method to induce performance demand: They provided live visual feedback of genital arousal to men every 30 s during an erotic video and asked them to rate the percentage of full erection and indicate whether the erection was sufficient for intercourse. In men without sexual dysfunction, genital arousal was similar under conditions of performance demand distraction and no-distraction.
One final way that performance demand has been induced is via observation by others. Elliot and O’Donohue (1997) told women that they were being videotaped while listening to erotic tapes, and that a research assistant evaluated them on attractiveness, personality, and body language. This observational performance anxiety led to increased self-reported (but not genital) sexual arousal.
Summary
The effect of performance demand on genital arousal in nonclinical samples of men and women is variable. Performance demand appeared to have no effect on self-reported sexual arousal in men and a facilitative effect in women. In men with erectile difficulties, the effect of anxiety induced by performance demand is equivocal, although it is important to note that the few available studies do not support a decrease in sexual arousal. Research seems to suggest that being told to perform optimally versus believing that performance is suboptimal exerts different effects on sexual arousal in men and should be further explored. The number of studies where researchers manipulate performance demand relative to those where they manipulate anxious sensations is small. Moreover, gaps in the literature exist, such as studies directly comparing men and women and in clinical samples of women. Finally, most of the cognitive anxiety inductions have focused on performance demand. It remains to be seen whether other anxiety-related beliefs and expectations impact sexual arousal, which could then be targeted using, for instance, behavioral experiments in CBT.
Manipulations of attentional focus
In response to anxiety, people can have different reactions or urges. For instance, a person could focus their attention toward or away from what is making them anxious. They could also engage in other behaviors to manage anxiety such as avoidance, escape, or safety behaviors. Despite the inclusion of these behaviors in cognitive behavioral models of sexual dysfunction (e.g., ter Kuile and Reissing’s fear-avoidance model of vaginismus, 2014), we did not find any studies in which researchers examined the effect of these behaviors on sexual arousal. However, as seen in Table 1, we found nine studies that included manipulating attentional focus. In six, researchers directed participants’ attention away from sexual cues—a form of cognitive distraction, which Barlow (1986) hypothesized contributes to sexual dysfunction. In three, researchers directed participants’ attention toward the person’s own body or sexual arousal to induce spectatoring (i.e., focusing on oneself from a third-person perspective). Spectatoring is hypothesized to negatively affect sexual functioning by directing attention away from sexual pleasure and toward sexual performance (Wiederman, 2012) and is linked to Masters and Johnson’s (1970) theories about the etiology of sexual dysfunction.
Nonclinical samples
In six studies, researchers instructed participants to direct attention away from sexual cues to induce distraction; five of these studies were with men, one with women, and none included both men and women (see details in Table 2). 6 In men, the majority of studies showed that distraction decreased genital arousal and had no effect on self-reported sexual arousal. In women, Elliot and O’Donohue (1997) manipulated distraction and anxiety (see Table 1 for details). They found that in conditions of low anxiety, distraction resulted in decreased genital and self-reported sexual arousal compared to no-distraction. Interpretation of results from the high anxiety condition was complicated by the fact that women in this condition were also exposed to potential observation by others; therefore, separating the effect of distraction from that of performance anxiety is not possible. Only one study examined whether sexual arousal was affected by spectatoring in a nonclinical sample (Lange et al., 1981). Researchers found that genital arousal was unaffected in men who were asked to self-monitor their genital arousal compared to men who were not asked to monitor their genital arousal.
Clinical samples
As seen in Table 2, we identified two studies in which the effect of distraction on sexual arousal was studied in clinical samples of men, and none in clinical samples of women. Both studies in men with erectile difficulties suggested that distraction had no effect on either genital or self-reported arousal. Two studies examined spectatoring in clinical samples. Seal and Meston (2007) asked women with sexual dysfunctions to listen to erotic stories either in the presence or absence of a full-length mirror to enhance body awareness. Enhancing body awareness had no effect on genital arousal, but increased self-reported sexual arousal. In this study, increased body awareness did not induce cognitive distraction (as measured by questions pertaining to the content of the films) as had been expected. The authors suggested that increased body awareness without cognitive distraction may lead to increased self-reported sexual arousal (Seal & Meston, 2007).
In two related articles, Beck and Barlow (1986a, 1986b) compared the effect of sensate focus (attention toward thoughts, feelings, sensations) versus spectator focus (attention toward the size of their erection from an observer perspective), as well as performance demand (reviewed in the Manipulations of performance demand section), while watching an erotic film in men both with and without erectile dysfunction. They found that in men both with and without erectile dysfunction, sensate compared to spectator focus resulted in greater self-reported sexual arousal but not genital arousal, though men without erectile dysfunction self-reported greater sexual arousal overall (Beck & Barlow, 1986a). In a second paper, Beck and Barlow (1986b) examined the content of the men’s thoughts during the task. Men with erectile dysfunction reported more thoughts involving nonevaluative spectator focus, indicating that they did not evaluate themselves while focusing on their erection (Beck & Barlow, 1986b). In contrast, men without erectile dysfunction reported more thoughts about the erotic films, suggesting that they focused more on the erotic cues during the task.
Methodological considerations
The type of material used for distraction was highly variable. In fact, no two studies used identical procedures, which limits the conclusions that can be drawn. For example, Farkas, Sine, and Evans (1979) had participants keep a mental tally of tones they heard; Janssen, Vorst, Finn, and Bancroft (2002b) had participants complete math questions; and Elliott and O’Donohue (1997) had participants repeat sentences. The material in this study was also negatively valenced (e.g., sexually relevant, anxiety-provoking sentences such as “I might get herpes”; Elliott & O’Donohue, 1997). Unfortunately, the methodology of this study makes it difficult to determine if the valence of distracting material affects the impact of distraction on sexual arousal, though this would indeed be a beneficial line of inquiry. Given this variability, drawing firm conclusions about the role of distraction in sexual arousal is difficult. Regarding spectatoring, given the small number of studies conducted, it is virtually impossible to speculate how methodological factors may have impacted findings.
Summary
Research examining the role of attentional focus (i.e., using cognitive distraction and spectatoring) in sexual arousal is few. Considering the available research, preliminary evidence suggests that in nonclinical samples of men distraction either inhibits or has no effect on genital and self-reported sexual arousal, whereas neutral distraction may reduce both genital and self-reported sexual arousal in women (Elliott & O’Donohue, 1997). In clinical samples of men, distraction appears to have no effect on either genital or self-reported arousal. The effect of spectatoring appears to be inconsistent with predictions made from theoretical models (e.g., Masters & Johnson, 1970). Spectatoring does not appear to have a negative effect on men’s genital or self-reported sexual arousal, and in men with erectile dysfunctions may actually facilitate genital arousal. In women, despite evidence suggesting that body image self-consciousness during physical intimacy is associated with sexual dysfunction (Wiederman, 2012), manipulating body awareness experimentally does not seem to impact the degree of cognitive distraction or negatively affect sexual arousal (Seal & Meston, 2007). Further research is needed to clarify the effects of distraction and spectatoring in clinical and nonclinical samples of men and women. Indeed, should distraction have an inhibitory effect on sexual arousal, it may then warrant additional focus in treatment for clients who engage in sometimes subtle forms of distraction.
Discussion
Our goal was to review the experimental research in which researchers manipulated aspects of the anxiety response in erotic contexts to better understand under which conditions anxiety may inhibit, facilitate, or have no effect on sexual arousal. Furthermore, by working toward a clearer understanding of the experimental research investigating this complex relationship, we aimed to help inform cognitive behavioral interventions for sexual dysfunction.
Manipulations using anxiety-provoking stimuli or sensations produced variable effects on genital arousal. Based on the existing research, models that assert that anxiety can increase sexual arousal were only partially supported. Barlow (1986) suggested that increased autonomic arousal can facilitate sexual arousal in men without sexual dysfunction. However, with the exception of two studies upon which his model is based, enhancing anxious sensations either decreased or did not affect genital arousal in men. Additionally, although this model is a clinically focused model, we identified no studies in which anxious arousal was induced in clinical samples, and therefore cannot evaluate whether anxious arousal inhibits sexual arousal in men with sexual dysfunction. These findings are also inconsistent with Zillman’s (1983) excitation transfer hypothesis and the model proposed by Kempeneers and Barbier (2008) that suggests that anxious arousal could enhance sexual responsivity via the misinterpretation of anxious arousal sensations. However, it is notable that we were unable to locate studies examining if anxious sensations are misinterpreted as sexual sensations. As such, whereas a reduction of anxiety may increase general well-being and thereby increase sexual function, this effect appears indirect and may not always result in the desired impact.
Based on research with men and limited research with women, Masters and Johnson’s (1970) theory stating that performance-based fears inhibit sexual arousal was not entirely supported. Again, genital arousal seemed to be influenced in a variable fashion. Although some studies found that performance demand decreased genital arousal in men, an equivalent number of studies found that it can also increase or have no effect on genital arousal. The majority of studies in men found that performance demand had no effect on self-reported sexual arousal. In contrast, in women, performance demand appeared to increase self-reported sexual arousal, though only two studies examined this topic.
Despite the correlational evidence that various beliefs (e.g., body image- and age-related beliefs) may constitute vulnerability factors for sexual dysfunctions (Nobre & Pinto-Gouveia, 2006), most studies in the review explored the effect of only a single belief relating to sexual performance (i.e., performance demand) on sexual arousal. There were virtually no studies that examined other belief domains, most notably pain catastrophizing. This is surprising given the role that pain catastrophizing plays in cognitive models of some sexual dysfunctions, such as pain and vaginal penetration–related problems in women (Reissing, 2009; ter Kuile & Reissing, 2014) and that such beliefs (e.g., pain fear and catastrophization) are related to treatment outcome (Desrochers, Bergeron, Khalifé, Dupuis, & Jodoin, 2010; ter Kuile et al., 2007). These treatment-related studies suggest that CBT targeting fear and catastrophization of pain may prove especially beneficial for women with pain-related sexual disorders. One of the few experimental studies to examine fear-related learning (e.g., via fear classical conditioning and extinction) in women with dyspareunia found that, during extinction, these women reported a greater shock expectancy for the erotic stimulus that had never been paired with a shock compared to the women without dyspareunia (Both et al., 2017). That is, even though the stimulus was “safe,” the women with dyspareunia expected pain in the form of a shock. Another study found that women with vaginismus reported greater fear of vaginal penetration stimuli and rated erotic stimuli as less inducive of positive affect than women without vaginismus (Melles et al., 2014). However, women both with and without vaginismus demonstrated similar automatic fear associations (i.e., a relatively fast and nonintentional affective appraisal) in response to erotic stimuli (Melles et al., 2014). These correlational designs suggest that fear and catastrophization of pain may be particularly important for dyspareunia and vaginismus. Experimental manipulations of key cognitions-related models of sexual dysfunction would strengthen the argument of a causal role of such cognitions in the etiology of these disorders.
Cognitive models that incorporate individual differences with regard to beliefs about anxiety and sexuality may be useful in explaining the variability of findings. For example, Janssen and Bancroft’s (2007) dual control model of sexual response might explain the variability with which anxiety influences sexual arousal. However, we found only one mixed-experimental study that examined how these individual differences might impact sexual arousal. Janssen and colleagues (2002b) found that men high in threat of sexual consequences were more likely to show a weaker genital arousal to films depicting coercive sex compared to men low in threat of sexual consequences. Perhaps individual differences on these various types of sexual inhibition as well as sexual excitation predict the degree to which anxiety-provoking sexual contexts facilitate or reduce sexual responding. Further research should experimentally examine the impact of sexual inhibition and sexual excitation on sexual arousal.
A transdiagnostic approach, such as Janssen and Bancroft’s (2007) model, examining individual differences in belief systems may be especially helpful to extend our understanding of the etiology of sexual dysfunction and lead to the development of interventions that are based on established research findings rather than clinical intuition. Indeed, in the study of anxiety-based disorders, such as obsessive compulsive disorder, panic disorder, and generalized anxiety disorder, advances in the understanding and treatment of these disorders arose from studying individual differences. For example, the identification of the catastrophic misinterpretation of certain bodily sensations as a mechanism in the development and maintenance of panic attacks (Clark, 1986) was influential in establishing and understanding why some individuals go on to develop panic disorder, despite the fact that experiencing panic attacks is a relatively common experience in the general population. Moreover, the construct of anxiety sensitivity (i.e., the fear of anxiety-related sensations because of their potential harmful consequences; Reiss & McNally, 1985) was also instrumental in developing evidence-based cognitive behavioral interventions for panic disorder. Correlational research suggests that anxiety sensitivity is associated with greater sexual functioning difficulties in both women (Gerrior, Watt, Weaver, & Gallagher, 2015; Tutino, Ouimet, & Shaughnessy, 2017) and men (Tutino, Shaughnessy, & Ouimet, 2018). Experimental research manipulating anxiety sensitivity (e.g., by inducing beliefs about physiological sensations and their consequences) is greatly needed to determine whether anxiety sensitivity impacts sexual arousal and other aspects of the sexual response.
Taken together, findings from the performance demand portion of this review and from correlational studies suggest that strategies focused on modifying beliefs and cognitive appraisals might be particularly helpful and informative in the treatment of sexual dysfunction. However, the range of cognitive beliefs manipulated is narrow, and further research examining the impact of various belief domains on sexual functioning is necessary. Considering that many criteria for sexual dysfunction are polythetic and as such, anxiety-related mechanisms may not be integral to sexual dysfunction for everyone, a case formulation approach whereby beliefs are assessed and then inform the treatment approach may help increase the effectiveness of CBT interventions.
Relatively few studies included manipulations of attentional focus. Distraction away from erotic cues seems to decrease or have no effect on genital and self-reported sexual arousal. Thus, Barlow’s (1986) model, wherein distraction negatively affects sexual arousal through decreased attention to sexual cues, is partially supported. This theory is further evidenced by Hamilton and Meston (2013), who found that greater distraction was the only variable correlated with less genital arousal in women. However, it is notable that none of the studies examining distraction were in clinical samples. Furthermore, the few studies on spectatoring suggested that this process seems to have no effect on genital arousal and an inhibitory effect on self-reported sexual responding in men, and possibly no effect on genital arousal and a positive effect on self-reported sexual responding in women. With the current state of the literature, Masters and Johnson’s (1970) model received limited supported given the lack of evidence that spectatoring and enhanced body awareness would decrease genital arousal. However, it is likely that how participants are instructed to focus their attention influenced whether the manipulations had a positive, a negative, or no effect on arousal and, therefore, the consequences of spectatoring on sexual arousal remain unclear. Overall, treatment strategies that aim to reduce distraction and increase attention toward sexual cues may be useful in increasing sexual arousal, especially self-reported, as exemplified by evidence-based approaches to the treatment of female sexual dysfunction using mindfulness approaches (for a meta-analysis, see Stephenson & Kerth, 2017). Attention modification techniques modeled on those that are designed for the treatment of anxiety disorders (see Jones & Sharpe, 2017 for a review) may be useful in this process by shifting attention away from distracting internal or external stimuli.
Limitations and gaps in the experimental literature
Implications of this review suggest that exercising caution when targeting anxiety in the treatment of sexual dysfunction is warranted. Although we embarked upon this review with the goal of identifying clear ways to enhance CBT for sexual dysfunctions via the effect of anxiety on sexual responding, we became quickly aware of the complexity surrounding the topic of study and of a number of gaps in the experimental literature. First, the experimental literature almost exclusively focuses on only one part of sexual response, sexual arousal, and thus little can be said about the effects of anxiety on other aspects, such as orgasm or satisfaction. Additionally, despite the clinical relevance of influential theoretical models of anxiety and sexual arousal, little experimental research has been conducted in clinical samples and results in these samples has been variable. Thus, targeting anxiety may have unpredictable effects on sexual arousal. The findings must be considered within, and actually may be explained by, the limitations of the studies included in the review (e.g., small sample sizes, varying definitions of constructs, methodological differences). For instance, many of the reviewed studies were conducted many years ago; more modern studies would be informative. Moreover, a discussion of the size of the effects, although critical and in line with current research practices, is not possible since most studies did not provide information on effect size. Future research on anxiety and sexual arousal should focus on the size of the effects to fill this gap in the literature.
A need for increased reliability and validity
Overall, there was a lack of consistency with regard to the way that the anxiety response was manipulated and also (though to a lesser extent) in how sexual arousal was measured. It is possible that some manipulations (e.g., narratives) invoked not only anxious sensations and affect, but also beliefs and interpretations related to the content in a way that other methods (e.g., shock threat) did not. Furthermore, some of these methods of inducing anxiety are more ecologically valid than others (e.g., will a person be completing arithmetic equations during sexual activity?). Although using this type of manipulation allows for increased consistency across participants and better variable control, generalizability remains an issue, highlighting the importance of balancing the internal and external validity of the studies constitutes one of the main challenges of cognitive behavioral experimental psychopathology research.
Greater precision in defining what aspect of the anxiety response is being manipulated, particularly in light of the fact that different manipulations seem to affect sexual arousal slightly differently, is imperative. There also appears to be a disconnect between what clinical and experimental research is measuring, which has perhaps led to a lack of conceptual clarity in the literature. We have found that researchers examining the efficacy of treatments do not always measure anxiety per se and that, conversely, experimental researchers do not examine the impact of fear of penetration. Moving forward, specific fear-related beliefs, distractions, or other (mal)adaptive behaviors (e.g., avoidance, safety behaviors) that are likely to be present in sexual situations should be systematically identified and then experimentally manipulated. The use of ambulatory approaches rather than lab-based paradigms to assess sexual arousal may also add to ecological validity. Finally, since many sexual activities include a partner and Pâquet and colleagues (2018) reported that daily anxiety symptoms influenced sexual outcomes in women with vulvodynia and their partners, incorporating a partner into experimental paradigms may reveal important insights into the source of anxiety and be more effective in producing meaningful effects on sexual arousal contributing to sexual dysfunction.
In addition, not all studies measured both genital and self-reported sexual arousal. This may be particularly important given that the effect of the anxiety response manipulations on self-reported sexual arousal was sometimes different than on genital arousal (e.g., Barlow et al., 1983; Elliott & O’Donohue, 1997; Meston & Heiman, 1998). The concordance between genital arousal and self-reported arousal is greater in men than in women (Bouchard, Chivers, & Pukall, 2017; Chivers, Seto, Lalumière, Laan, & Grimbos, 2010). Therefore, we recommend that researchers include multiple measures of sexual arousal (i.e, genital and self-reported) within their studies as well as provide further discussion on how the chosen measure may affect the interpretation of results. For instance, “self-reported sexual arousal” was assessed via self-reported sexual desire, perceived genital sensations, or self-reported sexual arousal. Research suggests that these different ways of assessing perceived sexual responding are not identical (Chivers et al., 2010). Furthermore, constructs such as sexual desire may not be identical in both men and women. For example, research suggests that women may have more difficulty than men differentiating sexual arousal from sexual desire (Dawson & Chivers, 2014). Given the complex relationship between self-reported and genital arousal both clinically and in the experimental literature, inclusion of both measures in future research will be important.
As noted, the other components of sexuality (e.g., sexual satisfaction, orgasm, willingness to engage in sexual activities) have been less frequently studied than sexual arousal in the experimental literature. Anxiety may impact these other components, such as orgasm, or other important sexual outcomes like sexual satisfaction, or the strength of sexual interests. Importantly, in treatment outcome research, outcome is often limited to the behavioral ability to experience intercourse; sexual function, pleasure, and satisfaction often remain impaired (ter Kuile et al., 2013). Therefore, research needs to include multiple sexual outcomes to fully understand the effect of anxiety on sexuality.
Sample diversity
There was virtually no research in which men and women were directly compared or studied using the same protocol; in fact, we identified only two studies, and the results were not consistent across the two studies (Beck & Bozman, 1995; Brom et al., 2015). Thus, relatively little is known about whether anxiety affects sexual arousal differently in men and women. This could indeed be relevant as there are documented gender differences with regard to the prevalence of anxiety disorders and sexual dysfunctions (e.g., Kessler, Petukhova, Sampson, Zaslavsky, & Wittchen, 2012; Laumann, Paik, & Rosen, 1999). There was also comparatively little research with clinical samples even though clinical models largely drive the research questions related to the role of anxiety in sexual dysfunction. More clinical experimental research is needed that manipulates the anxiety response in samples with sexual dysfunctions.
Moreover, to our knowledge, no research has experimentally examined the impact of anxiety on sexual arousal related to paraphilic interests and disorders. 7 A few researchers have theorized that threat-related constructs such as anxiety and sexual inhibition may be relevant for understanding paraphilic interests and sexual risk-taking (e.g., Janssen & Bancroft, 2007; Seto, 1992). There is also preliminary correlational evidence that people who positively interpret their bodily sensations (e.g., racing heart, sweating) also report more paraphilic interests (Kane & Ashbaugh, 2018). We had originally intended to review the impact of anxiety on sexual arousal in the context of both sexual dysfunction and paraphilias. However, it became clear early on that there were no experimental studies to examine. This lack of research was startling given that interventions for paraphilic disorders include techniques that may work by, directly or indirectly, increasing and decreasing anxiety relating to paraphilic and non-paraphilic behaviors, respectively (see Kaplan & Krueger, 2012 for a review). Therefore, better understanding how anxiety affects the sexual arousal of people with paraphilic disorders may aid in the refinement of treatments for these difficulties.
Limitations
We must note a few limitations of our literature review methodology. First, though we attempted to be consistent in our review, we did not employ formal systematic review methodology. Second, though we made attempts to categorize the studies by types of manipulation to facilitate interpretation of the results, it was not always clear what exactly was being manipulated (i.e., anxious sensations, thoughts, or attention) in a specific study. For example, we classified studies in which erotic audio-clips contained anxiety-provoking material as manipulating the physiological component of anxiety because no specific beliefs (e.g., cognitions) or behaviors were manipulated. However, it is likely that such material could also activate anxious cognitions (e.g., beliefs about safety).
Conclusions
We set out to review the experimental literature examining the effects of the anxiety response on sexual arousal, with an eye toward making suggestions for CBT for sexual dysfunction. A careful review of the research indicates that anxiety can sometimes inhibit, facilitate, or have no effect on sexual arousal, measured either via genital arousal or via self-reported sexual arousal. These perplexing findings do not fully support extant clinical models that suggest that anxiety is at the root of sexual dysfunction; complex interactions appear at play. Thus, our findings highlight the need to reexamine the utility and mechanisms of action of anxiety-focused interventions for sexual dysfunction. Future research would benefit from studies that aim to explore the question of why and how anxiety exerts a variable effect on sexual arousal rather than simply does anxiety exert an effect on sexual arousal. Experimental research examining the impact of individual differences in beliefs about anxiety (e.g., anxiety sensitivity) and sex (e.g., sexual inhibition, sexual excitation, fear of penetration) may prove a fruitful avenue toward answering this important question and pave the way toward more targeted and effective cognitive behavioral interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.