
Abstract
Purpose:
To examine the effects of radiation therapy on sexual health in cervical, breast, and prostate cancer patients.
Methods:
Four electronic databases (PubMed/PubMed Central, Google Scholar, Embase(Ovid), and SCOPUS) were searched, and articles published in English from January 1, 2011, through 2022 were extracted. Five reviewers independently selected primary studies that reported patient sexual health symptoms caused by cervical, breast, or prostate cancer following radiation therapy treatment. The primary outcome measures sexual health trends during or after radiation therapy through external beam radiotherapy or brachytherapy where applicable. Secondary outcomes measured predictive factors contributing to sexual health scores (age, race, and geographical location).
Results:
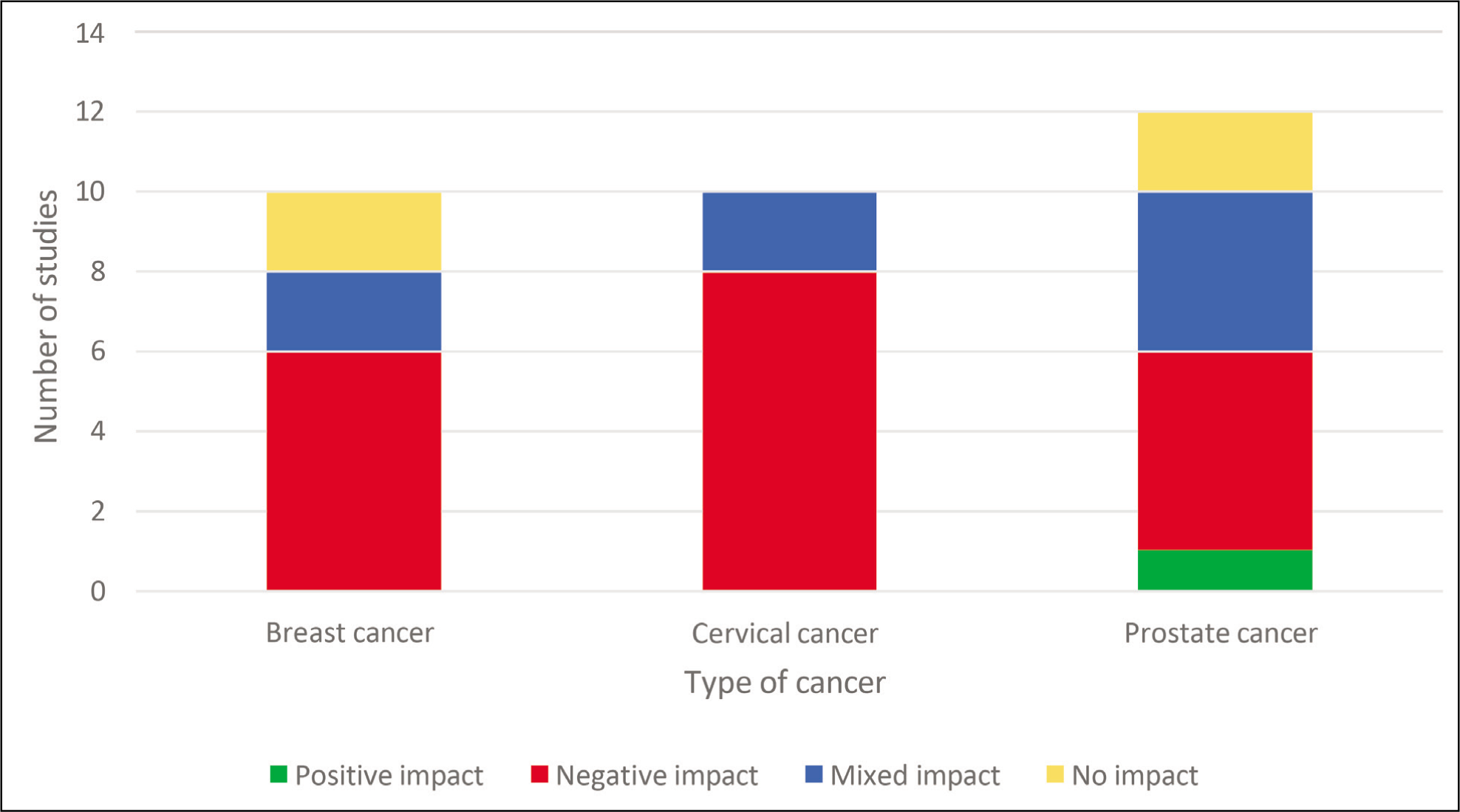
32 studies with a total of 5033 individuals were included in the systematic review. Overall, 19 studies reported a reduction in sexual health trends, 8 reported mixed trends, and 4 reported no significant trends in sexual health. Of the 10 breast cancer studies, 6 reported decreased sexual well-being, 2 found no trends, and 2 stated mixed trends. Among 12 prostate cancer studies, 5 reported worsening sexual health, 2 found no trends, 1 reported positive sexual functioning, and 4 found mixed trends. Among 10 cervical cancer studies, 8 reported worse sexual health, while 2 reported mixed trends. Younger breast and cervical cancer patients who received radiation therapy experienced greater body image and sexual health concerns. Evidence was insufficient to evaluate trends in geographical location or race between sexual health and radiation therapy.
Conclusion:
In this study, prostate, breast, and cervical cancer patients who received radiation therapy treatment experienced more troublesome sexual health symptoms compared to non-irradiated cancer patients. Interventions to improve sexual health should be prioritized.
Keywords
Introduction
Worldwide, more than 18.1 million people are diagnosed with cancer annually since 2020. Through improving technology and early detection, the number of cancer survivors has been increasing every year. 1 With various modalities available to treat cancers, radiation therapy is a highly preferred choice and is suggested as part of a treatment plan for more than 50% of cancer patients. 2 From 2000 to 2020, the absolute number of radiation-treated cancer survivors increased from 24% to 29%, with another estimated increase in future years. 3 An increase in long-term cancer survivors brings about the need to assess these patients’ quality of life (QoL), which is often described as the combination of physical, psychological, sexual, and social aspects of life. 4 Several studies have described the physiological effects of radiation therapy on sexual health. Incrocci studied the impact of radiation therapy on sexual dysfunction in prostate cancer patients, looking specifically at post-radiation erectile dysfunction. 5 Tramacere et al performed a systematic review on assessing sexual dysfunction in cervical cancer patients after varying treatment modalities, with notable side effects of vaginal stenosis, fibrosis, and lack of libido. 6 Boswell and Dizon discuss the impact of cancer treatment on breast cancer patients in their systematic review, wherein radiation contributed to worsening sexual well-being. 7 Despite the extensive body of literature on radiation-therapy-induced side effects, there is limited literature on the psychosocial aspects of sexual health and body image. The purpose of this systematic review is to assess the impact of radiation therapy on the sexual health of patients with cancer in three common sites—breast, prostate and cervix—and the varying degree of impact through the lens of age, race, and geographical location.
Radiation-Induced Side Effects in Patients with Cancers of the Breast, Cervix, and Prostate
Breast cancer (BC) is the most common cancer experienced by women globally, affecting as much as one in eight (12%) US women. 8 Radiation therapy (RT) is used for BC patients commonly after surgery, in unresectable cases, or when cancer has metastasized to other sites in the body. The two most common side effects experienced by BC patients post-radiation treatment include fatigue and skin reactions. For instance, one study found that dry skin, hyperpigmentation, and skin hypersensitivity were common symptoms patients experienced following RT. 9 Changes in physical appearance, limitations in sexual functioning, and the stigma of the disease can significantly impact a patient’s self-confidence and ability to experience intimacy and sexual pleasure. 10
Cervical cancer (CC) is the second most common cancer in women worldwide, and survivors of RT treatment for cervical cancer often experience significant disruptions to their QoL. These late effects of survivorship include sexual dysfunction and psychosocial concerns. 11 RT delivered close to the reproductive tract can significantly affect fertility by leading to impaired ovarian hormone production, uterine dysfunction due to inadequate estrogen exposure, and early menopause. 12 Some acute side effects of post-radiation treatment to the cervix region include erythema, moist desquamation, epithelial sloughing, and mucositis. Some long-term effects include vaginal wall thinning, fibrosis, and stenosis. 13 These side effects can reduce libido and intimacy, negatively impacting the ability of patients to enjoy or complete sexual intercourse. 13
Prostate cancer (PC) is one of the most common cancers found in men globally, although incidence and mortality rates vary substantially by population. The most common radiation treatment modalities for PC include external beam RT and low- or high-dose brachytherapy.14, 15 Despite high patient survival rates, there is often a significant impact on the QoL. Common side effects experienced post-treatment include urinary incontinence, a decline in sexual function, and erectile dysfunction. 15
Materials and Methods
Eligibility Criteria
Thirty-two studies were included in this review: 10 for BC, 10 for CC, and 12 for PC. Articles published between 2011 and 2022 were extracted for this study. Studies of individuals with BC, PC, or CC at stage 1, 2, or 3 who had received RT treatment were included. Data extraction was not limited to any geographic region, and studies that measured outcomes pertinent to sexual health were included. Studies with a sample size (N) of less 20 were excluded. Systematic and literature reviews were excluded alongside studies that utilized concurrent or adjuvant modalities (e.g., chemoradiotherapy, hormonal therapy, targeted therapy) during cancer treatment. This minimizes confounding factors that may have affected sexual health experiences due to concurrent treatments. Contrarily, surgical modalities were included as RT is often delivered as a post-operative or preoperative measure. Studies involving participants with stage 4 cancer, metastatic cancer, or palliative cancer diagnoses were also excluded.
Information Sources and Search Strategies
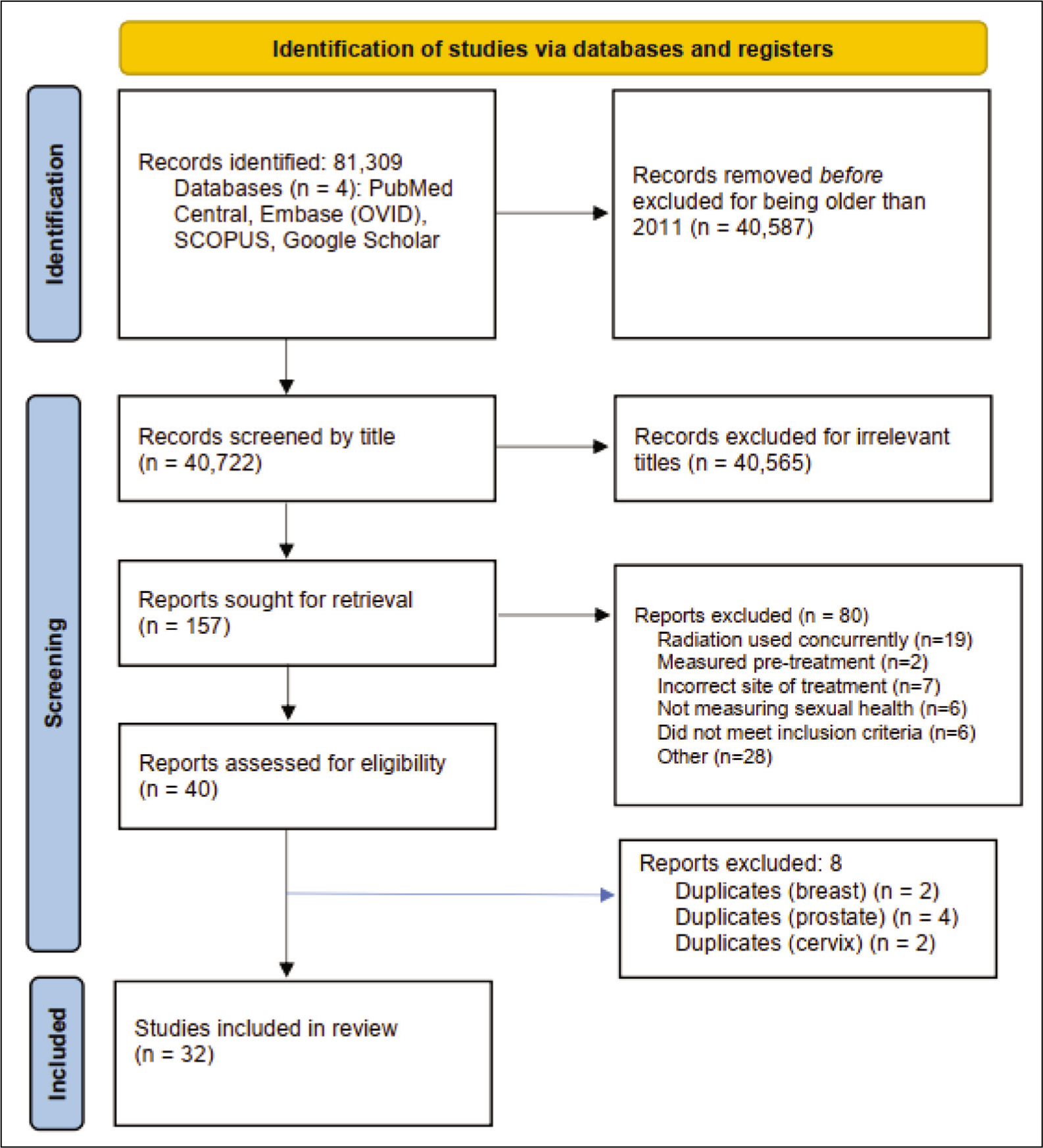
We performed a comprehensive literature search using four electronic databases for data extraction—EMBASE (Ovid), Google Scholar, PubMed/PubMed Central, and SCOPUS—and organized the search according to the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) format. Searches were limited to English-language articles published from January 1, 2011, through 2022 due to advanced technology in RT within the last 10 years. The studies were identified using medical subject headings (MeSH) terms “breast cancer,” “cervical cancer,” “prostate cancer,” “radiation therapy,” ”sexual health,” “body image,” “intimacy,” “age,” “race,” and “geographical location.” For each of the three cancers, the search strategy was a varied version of: (“cervical cancer” [Mesh] AND (“radiation therapy” [Mesh] OR “radiotherapy” [All fields]), AND (“sexual health” [Mesh] OR “sexual function” [All fields]), AND (“psychosocial” [Mesh] OR “psychosexual” [All fields]). To assess for age, race, and geographical location, for each type of cancer, the search strategy included (“age” [Mesh] OR “geographical location” [Mesh]) OR “race” [Mesh]). Studies without sexual function as a primary outcome were still included as long as they had sexual health as a measure with statistical significance.
Study Selection and Data Collection
Five members of the research team independently screened the studies (YB, NA, SA, MK, and SS). Titles and abstracts of the studies were screened to eliminate articles as part of the exclusion criteria. Following this, the text of the relevant articles was further screened for eligibility regarding context and quality. After a study was deemed eligible, each article was re-assessed twice by different team members. The research lead (YB) conducted a third and final check. All work was overlooked by a research advisor (TV). Each member of the team independently extracted data from their respective studies. Data was extracted extensively for BC (MK), PC (SS and NA), and CC (SA) (Figure 1). The second extraction process was conducted wherein researchers from another site were randomized to evaluate the articles similarly.
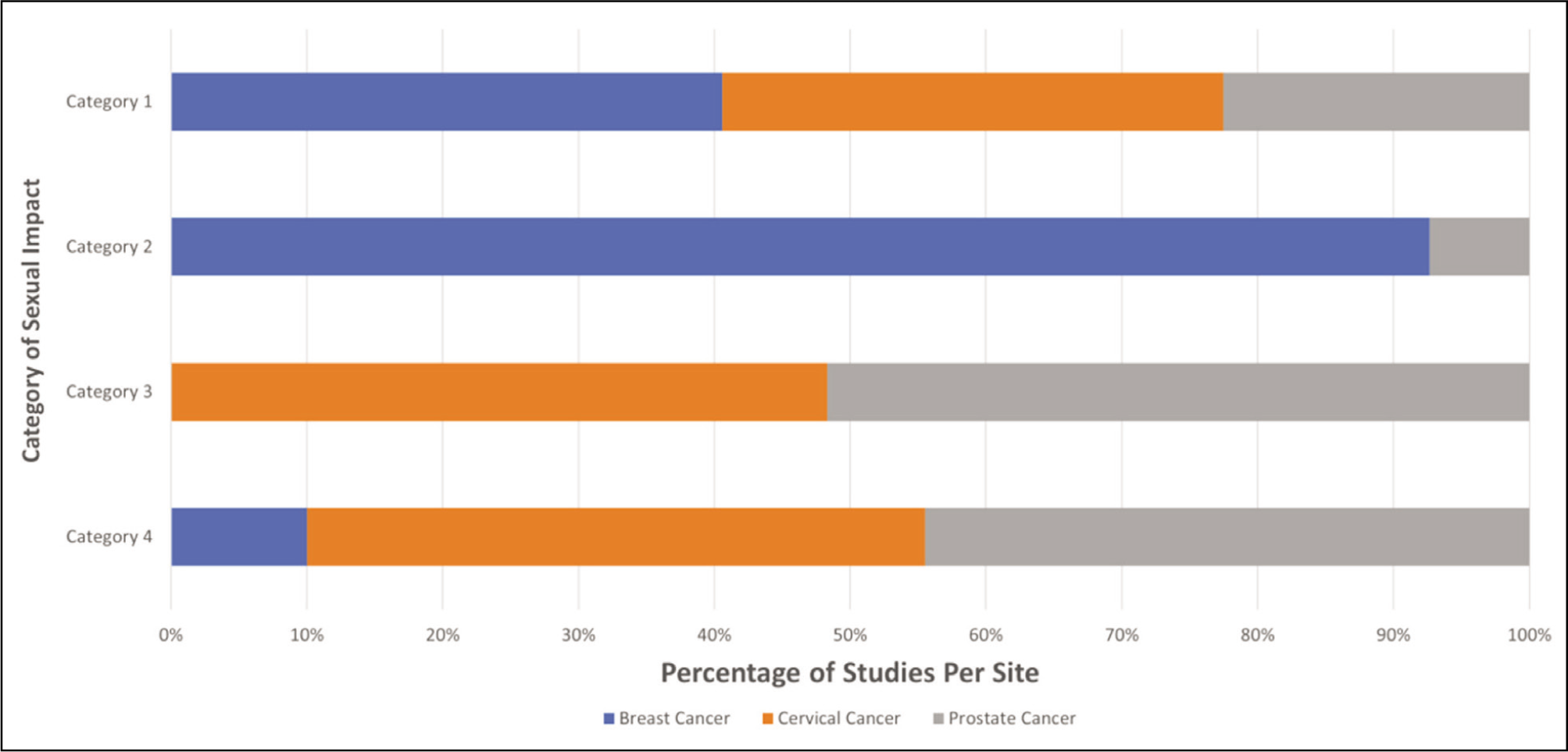
Disagreements were resolved among the researchers or through the lead researcher. Sexual health was categorized as (a) relationship satisfaction and intimacy concerns, (b) negative body image and self-esteem, (c) inability to experience sexual pleasure, and (d) physiological dysfunction (Table 1 and Figure 3).
Characteristics of Original Studies Assessing Sexual Function After Radiation Therapy in Breast, Prostate, and Cervical Cancer Patients.
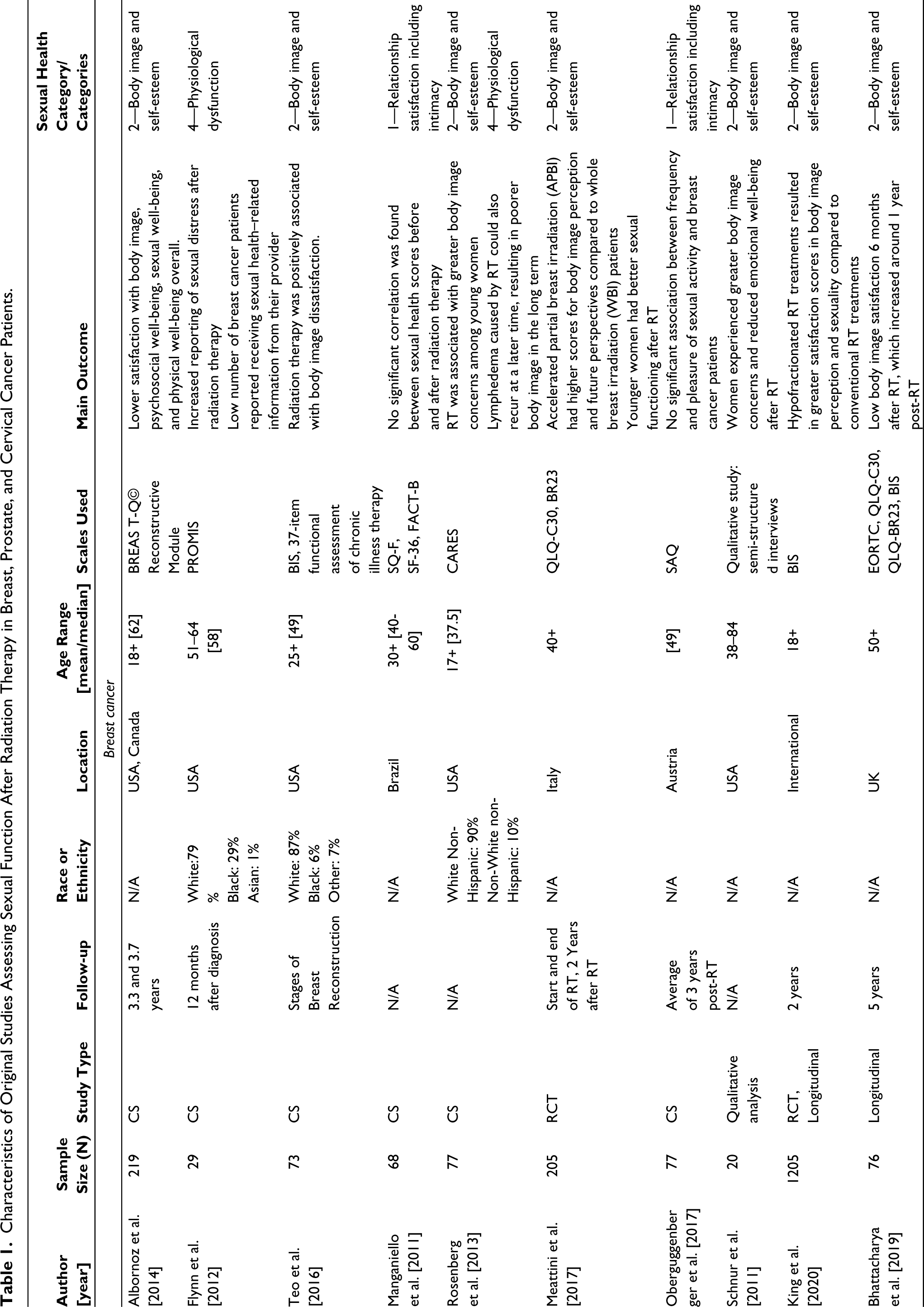
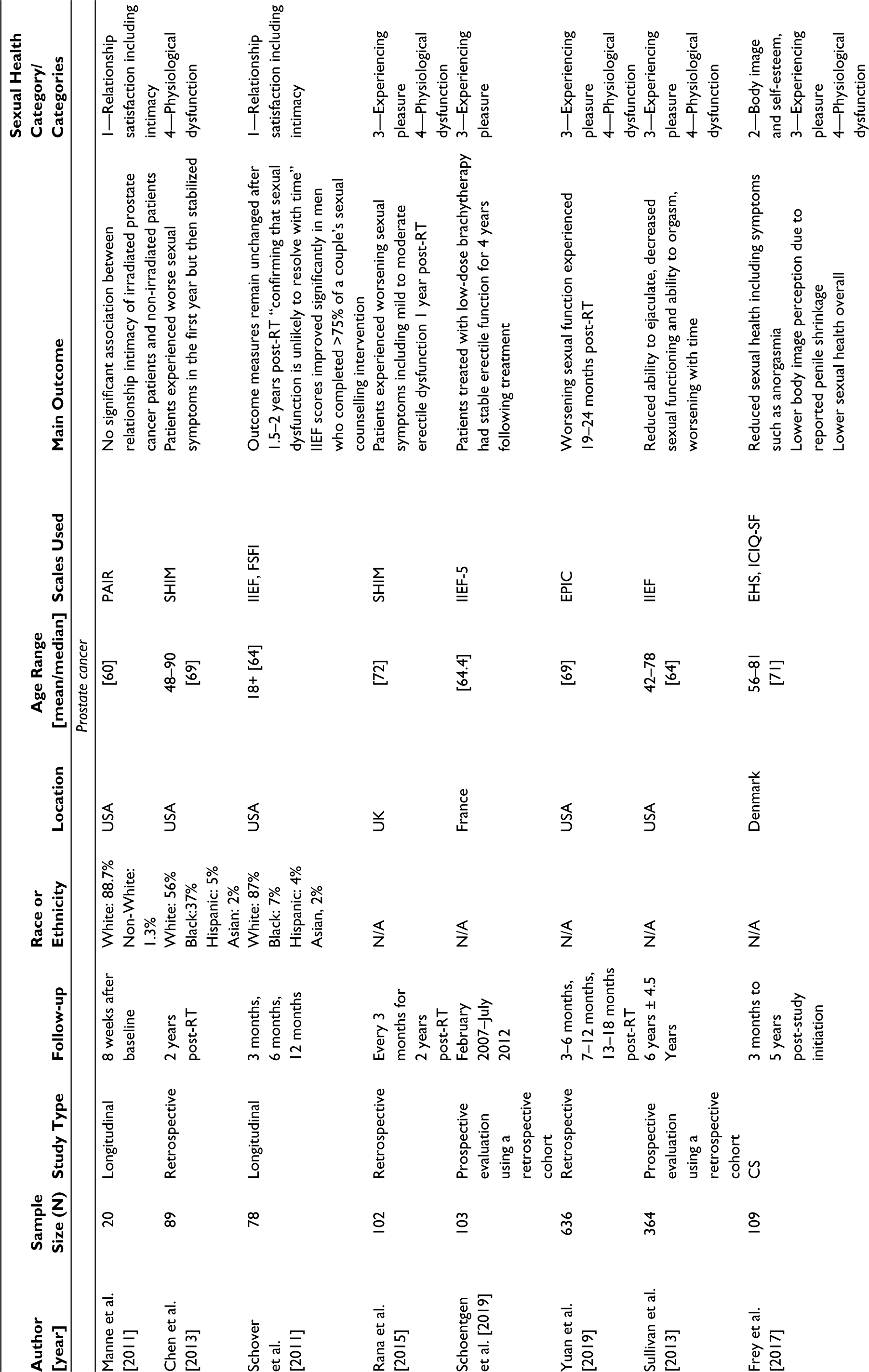
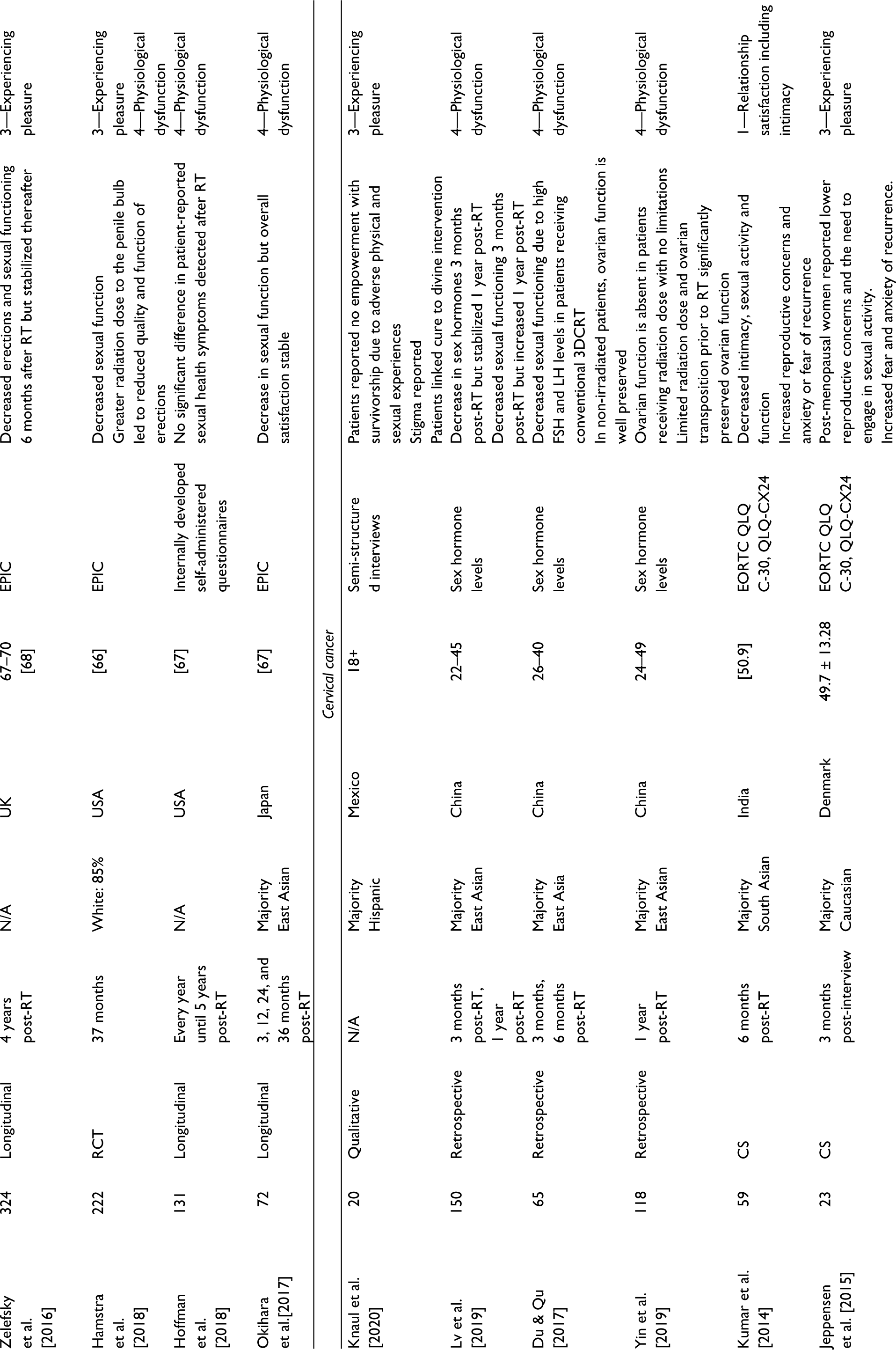
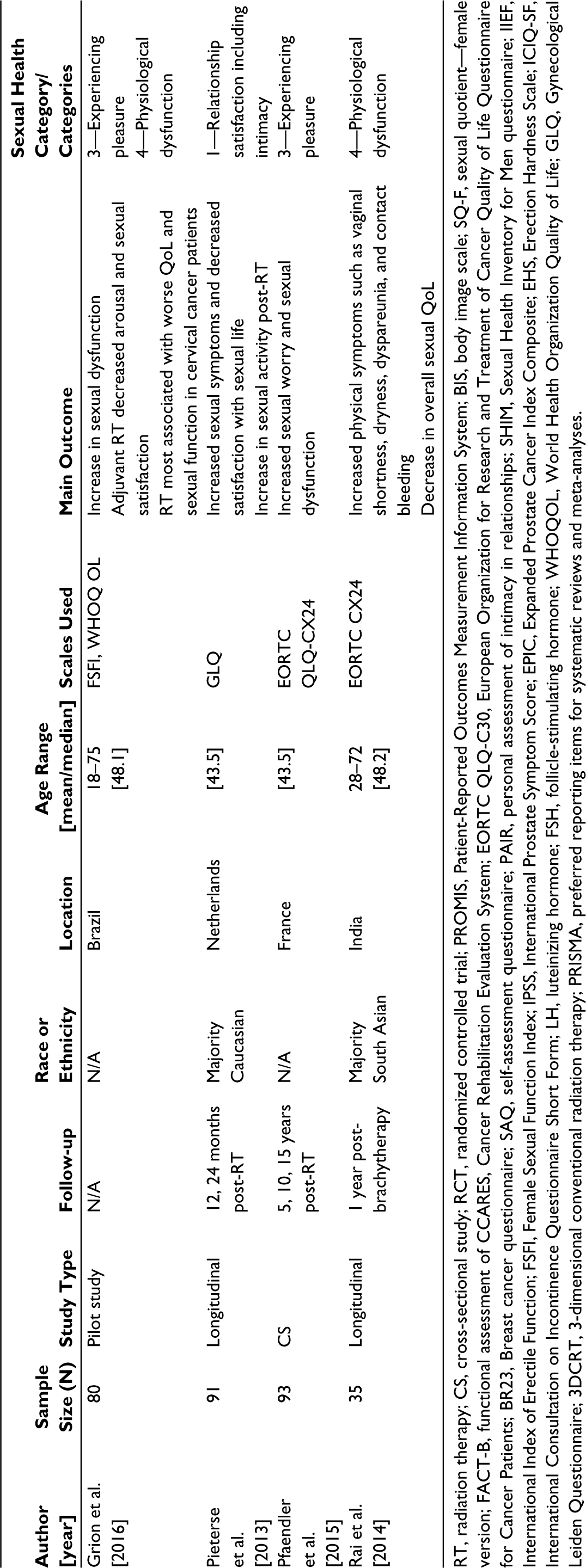
RT, radiation therapy; CS, cross-sectional study; RCT, randomized controlled trial; PROMIS, Patient-Reported Outcomes Measurement Information System; BIS, body image scale; SQ-F, sexual quotient—female version; FACT-B, functional assessment of CCARES, Cancer Rehabilitation Evaluation System; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Cancer Patients; BR23, Breast cancer questionnaire; SAQ, self-assessment questionnaire; PAIR, personal assessment of intimacy in relationships; SHIM, Sexual Health Inventory for Men questionnaire; IIEF, International Index of Erectile Function; FSFI, Female Sexual Function Index; IPSS, International Prostate Symptom Score; EPIC, Expanded Prostate Cancer Index Composite; EHS, Erection Hardness Scale; ICIQ-SF, International Consultation on Incontinence Questionnaire Short Form; LH, luteinizing hormone; FSH, follicle-stimulating hormone; WHOQOL, World Health Organization Quality of Life; GLQ, Gynecological Leiden Questionnaire; 3DCRT, 3-dimensional conventional radiation therapy; PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Data Items
When available, the following data items were extracted and assembled into Table 1: (a) general study information, such as the title of the study, DOI, follow-up time, year of publication (i.e., 2011–2022), study design, geographical location (i.e., developed vs. developing country) and number of patients analyzed; (b) patient demographics, such as age, sex, race, and eligibility criteria; and (c) results on sexual health. Geographical location was included for a global approach as we study correlations and differences between demographics, diversity, cultural taboos, and sexual health.
Results
Study Selection and Characteristics
Breast Cancer
Of the 10 studies used to analyze BC, 7 were cross-sectional,16–22 one was a qualitative study, 23 and two were longitudinal.24, 25 Five studies were conducted in the United States,16–18, 20, 23 one in Canada, 16 one in Brazil, 19 one in Austria, 22 one in the United Kingdom, 25 one including participants from multiple countries, 24 and one in Italy. 26 The scales used to evaluate sexual functioning in the 11 studies are summarized in Figure 1.
Cervical Cancer
A total of 10 studies that discussed the sexual impact of RT in cervical cancer patients were selected. Of these, three were retrospective analyses,27–29 three were cross-sectional studies,11, 30, 31 two were longitudinal,32, 33 one was a clinical trial, 34 and one was a qualitative study. 35 Three studies were conducted in China27–29 two in India,30, 32 one in France, 11 one in Denmark, 31 one in the Netherlands, 33 one in Brazil, 34 and one in Mexico. 35 However, two studies did not follow up on their participants.34, 35 The scales used in CC-related studies are summarized in Figure 2.
Impact of Radiation Therapy on Sexual Function Categorized by Site.
Prostate Cancer
Twelve studies relating to the sexual effects of RT treatment on PC patients were aggregated, which contained five longitudinal studies,36–40 two retrospective analyses,41, 42 two prospective studies,43, 44 one cross-sectional study, 45 and one randomized trial. 46 Seven studies were conducted in the United States,36, 37, 39, 42, 44, 46, 47, two in the United Kingdom,38, 41 one in France, 43 one in Denmark, 45 and one in Japan. 40 The scales used to assess various QoL and sexual functions by researchers are summarized in Figure 3.
Categorizing the Impact of Radiation Therapy on Sexual Health Among Breast, Cervical, and Prostate Cancer; Category 1: Relationship Satisfaction and Intimacy Concerns, Category 2: Negative Body Image and Self-Esteem, Category 3: Inability to Experience Sexual Pleasure, Category 4: Physical Dysfunction.
Impact on Sexual Health
Breast Cancer
Body image perception in BC patients was significantly lower in patients who underwent RT compared to patients who did not (p < .01).16, 18 Additionally, irradiated patients reported significantly lower sexual well-being (p < .01), psychosocial well-being (p < .01), as well as physical well-being (p < .01) compared to non-irradiated patients. Specifically for younger patients with an early stage of BC, RT was reported to be a significant predictor of body image concerns. 20 A higher tumor grade was associated with lowered perceived sexual attractiveness and femininity. 25 Larger breast size was also found to be a predictor of feelings of dissatisfaction with appearance. 25 In another study where BC patients were interviewed, it was reported that RT-induced skin changes (referred to as “skin toxicity”) such as erythema, hyperpigmentation, and ulceration were negatively associated with QoL, body image, and emotional well-being. 23 African American women were reportedly more affected by RT-induced skin toxicity. 23 Patients who received hypo-fractionated whole-breast RT reported better body image and sexuality outcomes than those who received conventional whole-breast RT (p = .0016). 24 For both radiation modalities, body image and sexuality were worse after treatment compared to pre-treatment.
Perceived body image was significantly better (p < .01) in people who received accelerated partial-breast irradiation than in those who received whole-breast radiation. 26 No significant difference was found between the two groups regarding sexual functioning or enjoyment, although survey completion rates were low. Another study found no association between RT and sexual quotient, which was considered a test for sexual functioning in females. 19 Similarly, yet another study found no treatment-related association between RT and sexual health when comparing BC survivors with non-BC individuals. 22
Cervical Cancer
Of the 10 studies analyzed for CC, 8 reported some deterioration in sexual health. A decrease in quality of sexual life, either through an increase in sexual dysfunction or a decline in sexual function, was a common finding.11, 28, 30, 32, 34 In a study by Jeppesen et al, CC patients treated with RT experienced significant deterioration in vaginal functioning (p = .029), decreases in sexual activity (55% of women), and increased worry of painful intercourse (p = .081). 31 Women reported experiencing a negative body image and decreased vaginal lubrication, sexual activity, enjoyment, functioning, and worry; however, these results were not statistically significant.31, 33 Rai et al assessed physiological dysfunction in RT-treated CC patients where vaginal shortness (62.8%), vaginal dryness (25.7%), and contact bleeding (28.5%) were reported, contributing to a significantly reduced quality of sexual life. 32 Some studies found initial decreases in sexual functioning within the first three months of receiving RT but found these sexual symptoms to return to baseline functioning levels after a year.27, 33 On the contrary, Pieterse et al reported increases in sexual activity post-RT but decreases in sexual function. 33 Du and Qu found increases in follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels in the first three months post-RT but significant decreases one-year post-radiotherapy (p < .05). 28 A reduction in FSH and LH levels corresponds to decreased sexual functioning. 28 Similar trends in estrogen levels were found with significant decreases three months post-radiotherapy with an increase one-year post-RT (p < .05).27, 28 Some studies reported increases in sexual worry, 11 anxiety, and fear of recurrence.30, 31 Jeppesen et al reported this finding was exclusive to post-menopausal women. 31 Moreover, while Kumar et al reported increases in reproductive concerns, 30 Jeppesen et al found decreases in reproductive concerns for post-menopausal women. 31
Prostate Cancer
Worsening sexual function after RT in PC patients was found in several studies.38–40, 42, 44-46.PC patients treated with stereotactic body radiation therapy (SBRT) generally experienced worsening sexual function one-year post-treatment, but these effects stabilized soon after. 47 Another study reported worsening sexual function one-year post-RT; however, there was a slight improvement in IPSS-I, IPSS-O, and SHIM scores, which remained below baseline scores. 41 Yuan et al’s study assessed EPIC scores in irradiated PC patients. 42 They reported a decrease in EPIC sexual domain scores, which was most prevalent at 19–24 months post-RT. 42 Also, in another study, 72% of PC patients undergoing RT experienced compromised sexual functioning, which worsened with time. 44 Frey et al.’s study reported that 24% of patients experienced anorgasmia and 44% reported a decreased intensity of orgasm. 45 Furthermore, subjective penile length loss over 1 cm was reported by 42% of RT-treated patients. 45
Similarly, Zelefsky et al’s baseline findings reported that 67% of men could experience erections firm enough for intercourse, but by six months post-RT, this rate fell to 22%. After six years, this percentage plateaued at 27%. The most significant adverse effect on sexual function was at six months. 38 In another study, 41% of men reported adequate baseline quality of sexual life (EPICN60 (mean, 77[±8.3]), but 59% experienced worsened sexual functioning three years post-RT. 46 In a study by Okihara et al, sexual function was worse after RT; however, it did not seem to represent a significant factor in determining patient satisfaction. 40
Some studies found little to no correlation between RT for PC and patient sexual health. One study found no association between the effects of hypofractionated RT and conventional fractionation on sexual health. 39 Manne et al 36 and Schoentgen et al 43 reported no significant consequences post-RT treatment concerning sexual function stability. Two years post-treatment, Chen et al deemed patients’ physical and mental health status similar to baseline status (p = .76 and .90, respectively). 47 In another study, the IIEF scores improved significantly in men who completed more than 75% of their treatment. 37
Age
The age range reported in the studies concerning BC was 37.5–64. Two studies looked uniquely at younger populations with an average age of 34.6 and 37.7 years.17, 18 One study classified its sample size into two groups: <50 years old and >50 years old. Out of the 12 studies, only three discussed age-related differences in QoL. One study categorized cervical cancer patients as pre-menopausal and post-menopausal (average age ~51 in the United States). 29 The average age of patients in all 12 studies combined for prostate cancer was 66.7.
Population Distribution by Country and Race
Two of 11 BC studies in this review reported the ethnic demographic distribution in its sample size. 18 Flynn et al’s study sample was composed of 87% Caucasian, 6% African American, and 7% categorized as “Other.” 17 In a study by Rosenberg et al, 90% of the study population was described as White non-Hispanic and 10% were described as non-White non-Hispanic individuals. 20
Among the list of included CC studies, one study assessed 73 Dutch individuals. 49 Another study conducted in India assessed 35 South Asian patients. 32 Lv et al’s study included 20 Hispanic patients. 47 The remaining eight studies did not determine study populations by ethnic demographics.
Out of the 12 studies assessing PC patients, only five outlined the racial diversity of the sample group in detail. Manne et al’s study population consisted of 88.7% White patients and 11.3% nonWhite patients. 36 Out of 89 patients, Chen et al found 56 (63%) patients identified as White, 37 (42%) as Black, 5 (6%) as Hispanic, and 2 (3%) as Asian. 47 Another study consisted of a patient population described as 87% White, 7% Black, 4% Hispanic, and 2% Asian. 37 Frey et al studied 109 Danish patients, 45 and Okihara et al 40 studied 72 Japanese patients.
Discussion
Impact of Radiation Therapy on Sexual Health
Breast Cancer
Overall, there was a significant impact on the sexual health of women undergoing RT for BC (Figure 2). Women experienced a decreased quality of sexual life, such as reduced satisfaction or inability to reach pre-treatment satisfaction levels.16, 26 More importantly, sexual health concerns can cause significant emotional distress, such as depression, problems with appearance, stigma, and adverse effects on personal relationships. 26
Cervical Cancer
Overall, there was a clear association between women undergoing RT and sexual health. Many women experienced a decreased quality of sexual life, described as a significant deterioration in vaginal functioning, reduction in sexual activities, and increased worry of painful intercourse.11, 40, 31-35 Likewise, symptoms such as negative body image, decreased vaginal lubrication, vaginal shortness, vaginal dryness, and contact bleeding were also experienced by many cervical cancer patients.32–35 Based on existing longitudinal studies, sexual health concerns continue to exist post-treatment. 33 This deterioration was mainly seen in patients undergoing RT as a modality. Also, some studies reported that complications persisted longer in women treated with RT.50, 51 Jensen et al’s findings reported that RT patients experienced dyspareunia for up to two years, compared to three months in patients treated with only surgery. 50 Likewise, two studies found that women undergoing RT reported more instances of diarrhea, uncontrollable urine discharge, and lymphedema.30, 33 Lastly, high levels of radiation were also associated with impaired ovarian function. Specifically, research published in 1991 had determined that radiation doses as low as 250–300 cGy inhibited ovarian function. 52 Notably, when this dose was increased to 500–1500 cGy, women experienced temporary infertility and hormonal disorders, whereas doses from 2000 to 3000 cGy induced irreversible damage to the ovaries. 52 Ovarian function was also preserved significantly more and longer in women who did not receive post-operative RT. For instance, Peterson et al found ovarian function to be preserved for 126 months without radiation in 98% women versus for 43 months post- RT treatment in 41% women. 53 A review by Pahisa et al also concurred that ovarian function was preserved only in 63.6% of RT patients versus 93% for patients without irradiation. 54 Overall, it was found that RT profoundly impacted the sexual health of CC patients (Figure 2). Our literature search suggests that RT when compared to other modalities poses a significant health burden on women, for which there is limited sexual-health-specific cancer care.
Prostate Cancer
Though there was an improvement in morbidity and QoL, significant negative trends were noticed post-radiotherapy in PC patients (Figure 2). Five out of twelve studies show a significant negative impact on sexual health, where patients reported erectile dysfunction, decreased ability to ejaculate, decreased sexual function, lymphedema, diarrhea, and urinary incontinence.38, 39, 41, 42, 44-46,47 These side effects reportedly peaked for approximately a year and stabilized soon after. According to Agaba et al, erectile dysfunction has explicitly been associated with poor QoL in social activities and overall health. 55 On the other hand, it is not related to physical fitness, feelings, daily activities, or health changes. Furthermore, the impact of negative physical symptoms associated with post-RT treatment on a patient’s mental health is often overlooked. As Lev et al outline, the experience of living with cancer through diagnosis, treatment decisions, the treatment itself, and survival is ridden with psychological distress. 56 Lev et al observe heightened levels of perceived distress in patients due to the physical symptoms of RT treatment (such as urinary, bowel, and sexual tribulations). Consequently, this lowers self-efficacy, leading to immense anxiety and worsening QoL, affecting many facets, such as sexual, social, and physical functions. 56
Age and Its Impact on Radiation-induced Sexual Health Dysfunction
Breast Cancer
In a study by Schnur et al, researchers interviewed BC patients and found lower levels of distress concerning skin changes in older participants. 23 Hoga et al reported that older Brazilian mastectomy patients found that the procedure did not affect their sexual relations as their marriages no longer centered around their sex life. 57 Existing literature supports our findings as the importance of body image, weight, appearance, self-objectification, and body surveillance decreases with age. 58 Alternatively, younger women with BC have been found to face more aggressive tumors, more extensive treatment, and higher chances of major reproductive life decisions being affected, leading to greater distress levels. 59 In contrast, a study by Park et al reported that older women (>50 years) reported worse QoL scores than younger women, especially concerning sexual relations. After correcting for age-correlated variables, however, they found that this QoL difference could be due to younger participants’ higher education level, more jobs, and increased daily activity level. 60
Cervical Cancer
The sexual functioning of CC patients following RT is significantly correlated with age. The age at which women engage in their first sexual intercourse is a known risk factor for CC as damage might be caused to the cervix at a time when it is still developing. This also includes the high risk of HPV infection in sexually active young women between 18 and 30 years of age. This infection at a younger age has suggested a slow progression to cancer in women aged 35 and above. 61 Specifically, the contraction of high-risk oncogenic HPV types at a younger age is an essential determinant in the development of CC. 61 In recent years, the median age of first sexual intercourse for females continues to fall, which may have profound implications for CC incidence. 62 In addition, a longer-term increase in sexual dysfunction and decreased sexual functioning was reported in patients treated with RT.47, 48, 30
Overall, some studies noted that younger (i.e., pre-menopausal) patients experienced more anxiety upon CC diagnosis when compared to older women. Many women feel their lives have “just begun” regarding their careers, family life, and independent goals. For instance, younger patients may have anxiety about raising their young children to childhood. Likewise, young survivors tend to have a greater fear of recurrence and worry surrounding reproductive health and infertility, including the grief of never having a child after diagnosis and treatment. 63
Prostate Cancer
The average age of PC patients in study samples is relatively high (64–70 years). Patients in this age group may value their QoL based on independent function and mobility over sexual competency. 64 Most studies within this age group displayed downward trends in sexual functionality up to one year post-treatment and an occasional improvement after the follow-up period. A limitation to having an older sample might be their unwillingness to participate in research studies or their inability to follow up with research conductors. 65 It is also important to note that due to the limited data available on younger PC patients, acquired data and analysis may be irrelevant to the younger population that experiences PC.
The Impact of Location and Race on Sexual Dysfunction
Breast Cancer
Unlike in upper-middle-income countries, many women in developing countries are diagnosed at a younger age and a more advanced stage, with a median age of 50 years, compared to 63 years. 66 Upper-middle-income countries with higher levels of education than developing countries may contribute to better awareness and coping mechanisms.
Research conducted in India and China found that most BC patients preferred breast-conserving surgery, despite the risk of lower long-term survival, due to perceived social stigma. 67 More research on the association between country classification and its impact on RT-induced sexual dysfunction should be considered.
Regarding race, only two of our studies identified the demographic distribution of their study population; in both, White women represented the majority of the sample size. This should further encourage researchers to study racial trends in the field of RT and to incorporate a multi-ethnic study population in their study for more representative results. Research by Lewis et al found that 45% of their African American BC patients wanted children at diagnosis, yet half did not receive resources and information on fertility. 68 Around 73% felt uncomfortable discussing sexual health concerns with their physicians, and more than half of the study population did not receive sexual health information on cancer care. Black women have higher rates of fertility issues than Caucasian women after BC, yet they often experience delayed diagnoses, fewer chemotherapy referrals, and medical mistrust.68, 69 Data on body image and sexual health within irradiated BC patients among various races is mainly unknown. This prompts further investigation for future research.
Cervical Cancer
Both developed and developing countries presented patients that experienced physical dysfunction (e.g., sexual dysfunction). There was a lack of conclusive trends between country classification (developed/developing countries) and the impacts of RT on sexual health. There was insufficient evidence to conclude a clear association between geographical location or race and the sexual health of CC patients undergoing RT. Despite this, some studies did report that patients in developing countries experience a more significant number of difficulties during and after treatment. For instance, Park et al reported that many patients from developing countries experience financial difficulties where an economic burden is a significant determinant of QoL. 70 Developing countries also present more stigma and barriers, especially concerning sexual health. As such, consultation sessions are often filled with shyness, discomfort, and emotional avoidance, hindering optimal healthcare delivery. 31
Lastly, developing countries generally have limited funding for the healthcare sector, which restricts patients’ access to post-treatment programs (i.e., post-treatment counselling sessions and follow-ups). For instance, the lack of survivorship care programs (as seen in Mexico) prevents post-operative counselling for cancer survivors, limiting emotional support and resulting in a more difficult recovery process. 35
Prostate Cancer
More than 90% of studies were conducted in developed nations, with the United States making up 50%. There are fewer studies on sexual health and prostate cancer in developing and Eastern countries. This could be due to a lack of research or cultural factors in Eastern countries that make sexual health taboo, reducing the number of study participants. 44 A higher incidence report in upper-middle-income countries may result from greater data collection through increased accessibility to medical care, including screening, early detection, and active research in this area. The imbalance of resources in healthcare systems can result in the lack of research in specific countries suffering from high rates of PC incidence. 71
With regard to African (SSA), Afro-Caribbean (AC), and sub-Saharan races, men from these communities suffer from the highest PC mortality rates in the world, ranging from 18.7 to 29.3 deaths per 100000 population based on 2012 GLOBOCAN data. 71 Apart from genetic factors, Black men are believed to be at a higher risk of PC due to decreased enrollment in clinical trials and decreased willingness to discuss these trials with their physicians. 72 Black men are more likely to express medical mistrust, lack of awareness, and social stigma. 73 They are also more likely to experience greater delays between diagnosis and treatment.74, 75 Some researchers have also found that Black men find sexual dysfunction a sensitive topic, which deter them from seeking medical care earlier and participating in clinical trials. 75 More than 90% of patients in a study by Woods et al believed that sexual function was important. 75 More research with multi-ethnic patients and diversified populations in clinical cancer trials is needed in developed and developing nations to understand the cultural, genetic, and economic factors.
Strengths and Limitations
A significant strength of our research includes addressing the limited research done to analyze the long-term psychosocial effects of cancer treatments, specifically within the field of RT. This review provides insights into how RT affects the sexual health of patients diagnosed with different types of cancers. Another strength of this study is our multi-site approach to analyzing three of the most common cancers: breast, cervical, and prostate cancer. In addition, we looked at the impact of sexual dysfunction on a patient’s overall well-being and QoL. To our knowledge, no current review has combined these sites and investigated the effects of RT on sexual health. Another strength of this study is the exploration of intersectional factors that impact a patient’s sexual health such as cultural factors, knowledge and awareness, race, geographical location, and age.
One limitation of our study was the limited number of studies that met the inclusion criteria set by our team. To prevent confounding results, the studies included in our review had to only include patients who received RT solely as their primary modality. However, most cancer treatments involve a combination of modalities, such as chemotherapy or hormonal therapy in conjunction with RT. Another limitation of our study is the possibility of self-reported biases in reporting symptoms. Some patients may under-report symptoms by only mentioning those known to be associated with their diagnosis. Minority ethnic groups may also under-report their symptoms due to cultural and social stigma.
Moreover, most studies in our analysis did not stratify results based on various age groups. Without stratification, analyzing trends among age groups became challenging and may have yielded results with lower accuracy and reliability. This information could help identify the trends in QoL among different age groups for cancer patients receiving RT. Another limitation of our study includes the possibility of generalized results that may not represent cultural factors, such as the stigma of sexual health between cultures and decreased access to health care. A lack of research in developing nations, especially in Eastern countries, can be attributed to stigma and taboos regarding sexual health.
Future Implications
Measurements of sexual health can be subjective according to the utilized scale. This can introduce biases into the results, making it difficult to compare sexual health across studies effectively. Our team suggests creating a universal, standardized symptom scale for cancers with similar psychosocial symptoms as a future direction to better operationalize the impact of sexual health. Bräutigam et al notes that radiation oncologists are often unable to discuss sexual health side effects with patients due to lack of competence in sexual health–based care, lack of time, and barriers of age, culture, and religion, which may render patients to feel cautious in bringing up sexual health concerns. 77 As such, increased medical training in providing sexual health–based care can help patients feel more comfortable and increase their overall QoL.
Conclusion
This review found that prostate, breast, and cervical cancer patients receiving RT experienced more significant sexual health symptoms than non-irradiated cancer patients. These patients often experienced lower self-satisfaction and body image, affecting their QoL. Some hospitals have begun opening clinics and forming healthcare teams for cancer-related sexual healthcare. More sexual health resources and initiatives should be prioritized to help provide personalized care across cancer sites.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.