
Abstract
Introduction:
Existing research literature has shown that the dynamics of depressive traits in adolescents are influenced heavily by various psycho-social factors such as peer pressure and addictive tendencies.
Purpose:
The study was conducted to investigate the interrelationship between internet addiction and peer pressure on adolescent depression.
Methodology:
The sample of adolescents (N = 94) in the age range of 13–18 years was collected using a stratified random sampling design. Three major psychometric tools were administered to the sample, namely, Internet Addiction Test, Peer Pressure Inventory, and Hamilton Depression Rating Scale. Correlation and inferential analyses were done on the acquired data.
Findings:
The sample reflected moderate tendencies to have peer pressure, internet addiction and depression. It also showed a significant positive correlation between internet addiction and depression, an insignificant positive relationship between peer pressure and depression along with a significant effect of sex on adolescent depression but insignificant sex differences on peer pressure and internet addiction.
Limitations:
The descriptive nature of the study reveals less about the causal relationships between the variables.
Implications:
The study encourages parents to redefine their roles and parenting styles while dealing with adolescents.
Introduction
The field of adolescent psychology is currently developing a new definition of adolescent mental health that is based on the description of a wide range of patterns of adaptation to the biological, psychological, and social challenges of adolescence. This article’s main focus is on how psychologists currently comprehend the extent and variety of these developmental routes, aptitudes, and adaption profiles. 1 It is common for adolescents to experience significant mood swings, depression, and excitement back-to-back. Explosive arguments with relatives, friends, and the law are regarded as usual. This widely held opinion is largely based on theoretical work done by the psychiatric clinical community in the 1950s and early 1960s.2–4
In the simplest of terms, adolescence can be defined as the transitional phase in a person’s life that is characterized by changes in various aspects of the individual’s physiological, cognitive, and affective domains.
Physiologically, bodies go through a series of rapid changes that result from attaining puberty. Adolescents also experience cognitive development in addition to physical development, the most notable of which includes a growing recognition of their own mental processes. We also talk about the school system, which takes up a lot of adolescent time, and the expanding influence of the internet on adolescent relationships, learning, and lives. 5
Adolescent adaptability and growth profiles derived through empirical research are being used to inform current viewpoints on adolescence, which are no longer only focused on theoretical interpretations of what should happen during puberty. Most importantly, the current understanding of adolescence does not come from a single mental health perspective. Instead, it is thought that a wide range of teenage behaviors, attitudes, social interactions, and developmental trajectories are important when conceptualizing adolescent mental health.
Adolescence is also considered a landmark in the developmental course that shows a range of affective disturbances due to various biopsychosocial factors. One of the primary mental illnesses with the highest prevalence is depression, and it is now widely acknowledged that depression frequently starts in adolescence and progresses throughout life. 6 Depression is a multidimensional state of emotional disturbance that has been assigned as the fourth most common factor in premature mortality and disability worldwide. 7 The epidemiology of depression in this age group is supportive of this finding. Between 20% and 50% of teenagers self-report significant, subsyndromal levels of depression, according to cross-sectional investigations of adolescent self-reported depressed symptoms (ie, less than a clinically significant depressive disorder). 8 Self-reported depression symptoms have also been the subject of prospective longitudinal research,9–12 which has revealed that the average levels of depressive mood and symptoms rise significantly from relatively low rates in childhood to much-increasing degrees beginning in middle adolescence.
Our research attempts to provide an understanding of adolescent depression as a function of two socio-cognitive predictors, namely peer pressure and internet addiction. Peer pressure is characterized as the pressure to think or act in accordance with particular peer-prescribed norms and is one of the key characteristics of adolescence. It serves as the major method of disseminating group norms and upholding group members’ allegiances. 13 Peer relationships are a crucial part of teenage socialization 14 and help individuals establish a sense of identity. 3
To put it very simply, addiction can be defined as the overuse and abuse of some substance or service that might eventually lead to pathological consequences. Using the internet to accomplish a task within a reasonable amount of time without experiencing mental or behavioral discomfort is considered healthy internet use. 15 On the other hand, internet addiction is typically described as an uncontrolled urge to use the internet excessively, a depreciation of days consumed offline, severe anxiety, and hostility when deprived of the internet, and progressive degeneration of community and personal functioning. 16
It is obvious that nonusers and substance users of all kinds vary on a variety of levels. These variations could be genetic, 17 personality-related, 18 or social differences in social situations and reactions.18,19 The fact that some aspects of people’s lives are constantly different between users and nonusers has emerged, despite the fact that the specific nature of the variations in social situations is still far from obvious. Particularly these areas include peer and family influence, 20 academic achievement and expectations, 21 family structure, 22 religious belief, 23 peer and family expectations, delinquency, 24 and delinquency statistics.
Methods
Hypothesis
In this particular study, we tried to explore multiple hypotheses. Those are listed as follows:
There is no statistically significant correlation between the levels of internet addiction and depressive syndrome severity. There is no statistically significant correlation between the subjective experience of peer pressure and depressive syndrome severity. There is no statistically significant sex difference in depressive syndrome severity. There is no statistically significant sex difference in the levels of internet addiction. There is no statistically significant sex difference in the subjective experience of peer pressure.
Sample
Sample size: 94 teenagers and young adults.
Sampling technique: Stratified random sampling.
Inclusion criteria: The following inclusive criteria were used:
Age: 15 to 18 years. Sex: Male and Female. Academic qualification: Minimum class 8th pass. Duration of involvement in social media within a day: Individual must use social media for at least 3–4 hours every day. Frequency: The person makes at least 10 visits to these social media platforms each day. The number of peers within a group has an effect on the individual: We considered groups of 2–6 people, which we may define as small groups since as adolescents get older, they prefer to engage and hang out with fewer people. Type of social media considered: Any digital system, platform, website, or application that enables users to produce and share information as well as engage with one another is referred to as social media.
Measurement Tools
Internet Addiction Test (IAT)
The existence and degree of internet dependence among people are assessed using the 20-item IAT. 25 The IAT was created by Dr Kimberly Young, a professor at St. Bonaventure University and the director of the Centre of Internet Addiction Recovery, to evaluate internet addiction and compulsive behaviors in various test scenarios. The 20-item test assesses compulsivity, escapism, and reliance in addition to the traits and behaviors linked with compulsive internet use. Additionally, questions determine whether an addictive behavior affects social, vocational, or personal functioning.
Scoring: On a scale of 0–5, each object is given a rating. There is a 100-point maximum. The IAT offers a range of total scores, with a higher score indicating a more serious level of internet compulsivity and addiction. Total scores between 0 and 30 points are thought to represent typical internet usage; scores between 31 and 49 suggest a mild level of internet addiction; scores between 50 and 79 reflect a moderate level, and scores between 80 and 100 indicate a serious reliance on the internet.
Reliability: The scale’s internal consistency or reliability according to Cronbach’s alpha was good to moderate (α = 0.54–0.82).
Validity: The validity of the scale was further demonstrated by the fact that there was a positive link between the average general and private internet usage and the 6 criteria. Both overall internet use and the total IAT score (r = 0.22, p = 0.05, one-tailed) and personal internet use (r = 0.3, p = 0.01, one-tailed) were found to be positively correlated.
Peer Pressure Inventory (PPI)
Brown and Clasen 26 created this scale based on 5 dimensions: (i) peer compliance, (ii) parental participation, (iii) peer involvement, (iv) school involvement, and (v) misconduct. The 53 elements on the scale gauge how much peer pressure is present in various contexts.
Scoring: Each item receives a value between −3 and +3, with “No Pressure” receiving a score of 0. The mean of the item scores is used to calculate the subscale scores. A letter identifying the subscale with which the item is related and a number indicating the item-to-scale correlation correction are displayed in the “No Pressure” box in place of the zero scores. Nothing in this box indicates that the item is not related to any of the 5 subscales. Peer conformity is represented by the letters C, F, P, S, and M, which stand for peer conformity, family involvement, peer involvement, school involvement, and misconduct, respectively.
Reliability: The scale displays internal consistency (α = 0.75–0.92).
Validity: The felt pressure scores within each group for peer involvement, school involvement, and misconduct closely matched an independent assessment of each peer group, which is one sign of the validity of the PPI.
Hamilton Depression Rating Scale (HDRS)
HDRS is the most popular clinician-rated scale for determining the severity of depression in patients with a depressive disorder who have already received a diagnosis. The original version by Hamilton 27 contained 17 elements that dealt with recent depressive symptoms. Later, a 21-item version (HDRS21) was created, which includes 4 questions that were designed to subtype depression but are occasionally, wrongly, used to score severity.
Scoring: The scoring system differs across versions. A score of 20 or above (showing at least severe severity) is typically required for entry into a clinical trial. For the HDRS17 used in this study, a score of 0–7 is generally recognized to be within the normal range (or in clinical remission). The item for measuring guilt is scored as follows as an example. 0 = absence, 1 = self-approach, 2 = thoughts of guilt or dwelling on past transgressions or sinful acts, 3 = present disease is retribution, and 4 = hearing accusing or denunciatory voices and/or encountering threatening visual hallucinations.
Reliability: When used to assess internal reliability, Cronbach’s alpha statistic would indicate a value of 0.70, which reflects a sufficient level of reliability. The scale’s Pearson’s r value, which should be at least 0.70, ranges from 0.82 to 0.98 for interrater reliability, and from 0.46 to 0.99 for interclass reliability (should be at a minimum of 0.60). The scale’s retest reliability, which ranged from 0.81 to 0.98, indicated that it is dependable.
Validity: HDRSis a tool for measuring and defining depression. The scale’s fundamental components have not changed in more than 40 years, despite the development of several extended versions, thus, we can assert that it has content validity. In a meta-analysis of 19 trials including a total of 1,150 patients, Edwards et al 28 examined the HDRS and Beck’s Depression Inventory’s predictive validity. As evidence of the HDRS validity, it was found more change-sensitive than the Beck Depression Inventory.
Statistical Analysis
For the descriptive analysis of the data, mean, standard deviation, and product-moment correlations were computed, and t-statistics were carried out to test the hypotheses considered.
Results
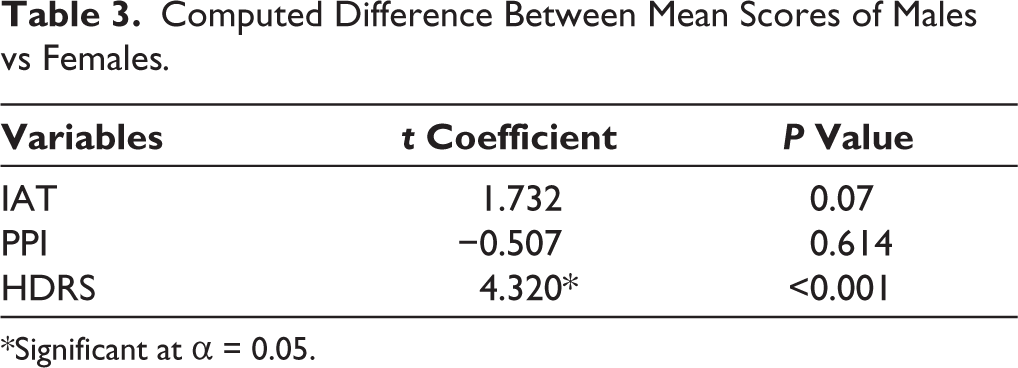
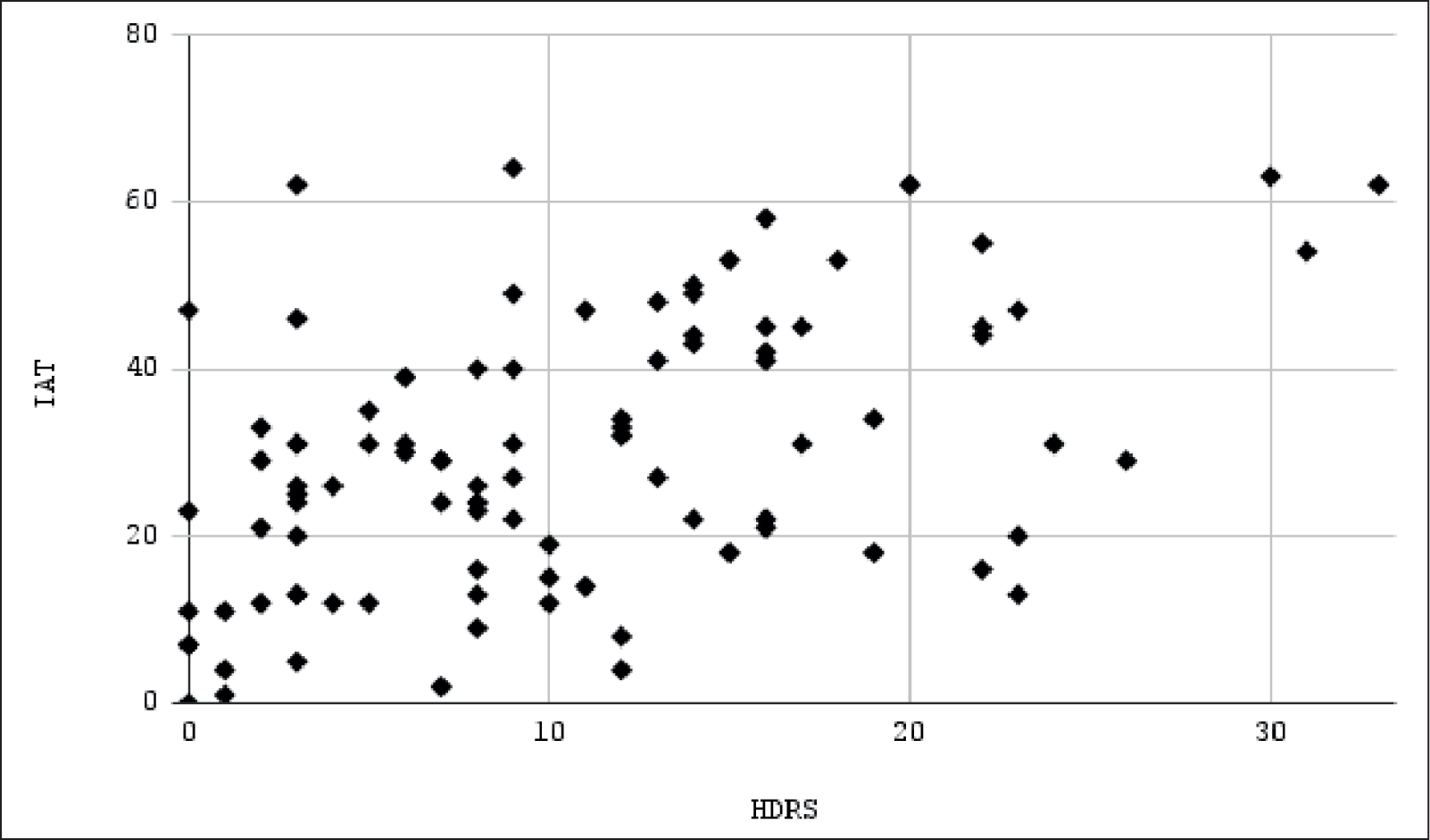
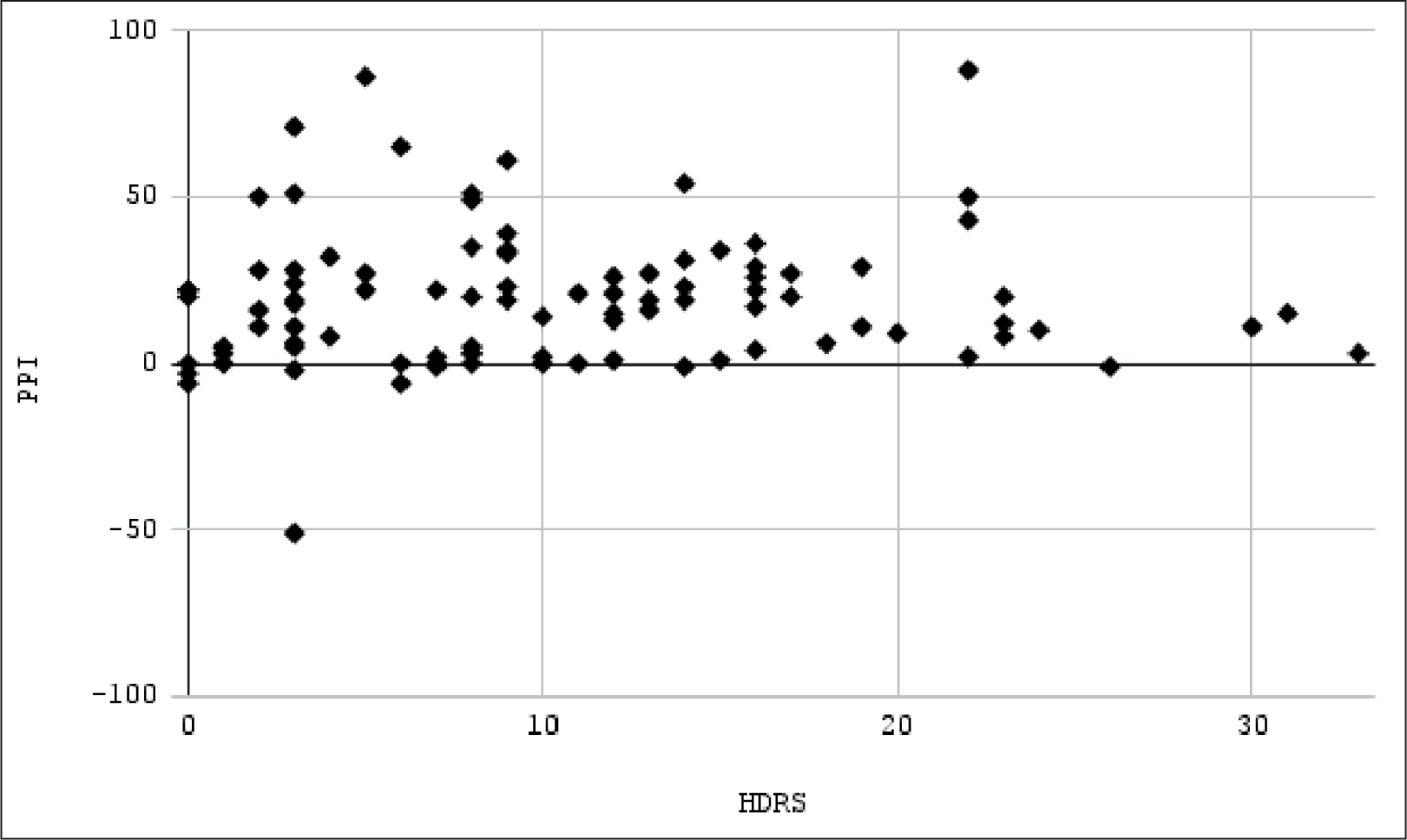
The sample reflected an average Internet Addiction Score of 29.51 (SD = 16.30), and the average score in the PPI was 19.28 (SD = 20.86). The sample also showed a mean HDRS score of 10.52 (SD = 7.76). Pearson’s product moment (r) correlation coefficients obtained were r(IAT, HDRS) (92) = 0.483, p < 0.001, which is statistically significant, and r(PPI, HDRS) (92) = 0.045, p = 0.665, which is statistically insignificant. The effects of sex on Internet Addiction and Peer Pressure scores, t (92) = 1.732, p = 007, and t (92) = −0.507, p = 0.614, respectively, were insignificant, but the effect of sex on HDRS scores, t (92) = 4.320, p < 0.001 was statistically significant.
The results obtained are conceptualized in the Tables 1 to 3 and Figures 1 and 2.
Descriptive Statistics of the Acquired Data.

Computed Correlation Coefficients of the Acquired Data.

Computed Difference Between Mean Scores of Males vs Females.
Scatterplot Between IAT and HDRS Scores (r = 0.483).
Scatterplot Between PPI and HDRS Scores (r = 0.045).
Discussion
These findings explain the sex differences in depression as a clinical construct between the adolescent age group. We successfully found a statistically significant difference between the two sexes, as has been substantiated previously. 29 Females are roughly twice as likely as males to be diagnosed with depression and show twice as many depressed symptoms by the middle of adolescence, and this tendency persists at least until age 55. 30
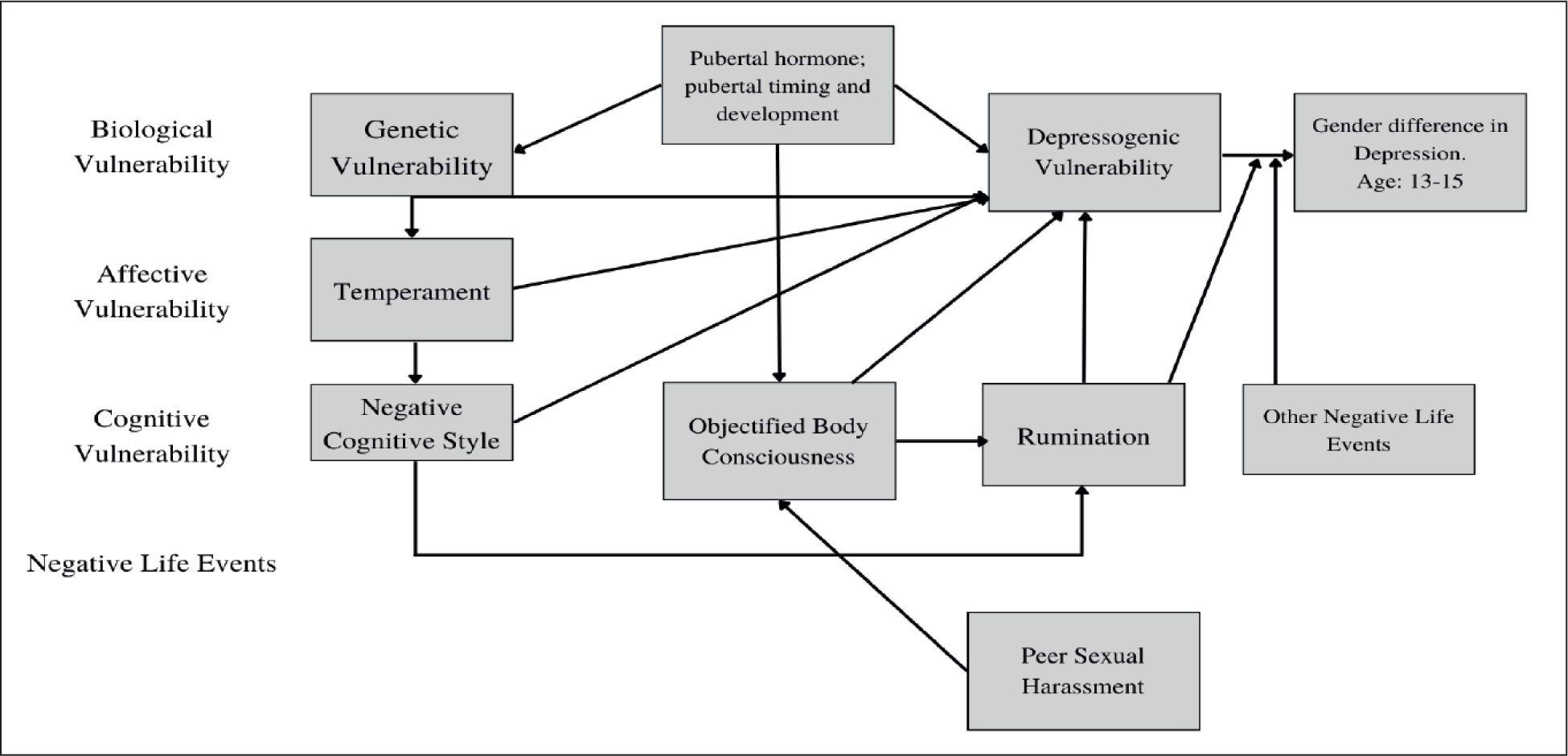
Various models and explanations have been suggested for this. Hyde et al 31 have put out an affective, biological, and cognitive theory to explain how sex disparities in adolescent depression evolve. In a nutshell, the model proposes that Objectified Body Consciousness (OBC), rumination, and negative cognitive style all contribute to cognitive vulnerability to depression. The model’s integrated component of affect postulates that early temperament traits of strong negative emotion are vulnerabilities in and of themselves and also help establish a negative cognitive style. There have been three biological factors put forth: hereditary factors, puberty-related hormones (dehydroepiandrosterone, estrogen, and testosterone), and pubertal timing. Finally, social factors are crucial to the concept because they frequently take the shape of social and interpersonal interactions, such as peer pressure or sexual harassment, parent–child conflict, or dysfunctional parent–child relationships. 31 Figure 3 represents the same.
Since humans are social creatures, it takes them a long time to develop in dyadic, small-group, and other group settings. Therefore, it is not unexpected that a growing body of research indicates that having a sense of social belonging makes people happier and healthier. A number of unpleasant emotional states, such as anxiety, despair, rage, and shame, are connected to social exclusion and isolation. 32 According to the literature, belonging to a peer group may both positively and negatively correlate with behavioral issues. 33 However, our data suggest that there is an almost negligible correlational relationship between the social constructs of peer pressure on adolescent depression. But that is negated by some promising findings which have proved that there is indeed a significant relationship between peer pressure and adolescent depression. 34 Such conflicting results can be attributed to the descriptive nature of our analysis or the differences in methodology and tools administered.
While discussing the sex differences in peer pressure, many studies revealed that adolescent males are more prone to deviant peer pressure than female adolescents. The reason is that adolescent males may be more influenced by abnormal peer pressure as they try to live up to traditional gender role stereotypes that associate masculinity with toughness and independence, as is the case for substance abuse and aggressive behavior.35,36 Even though descriptively speaking, our study also reveals a higher mean PPI score for males, the difference is not statistically significant in our case. Any kind of addiction can be considered extreme or deviant behavior, and with respect to that, we see internet addiction as no exception. There is evidence to suggest that adolescent males are more prone to risk-taking than females because their social environments give them more opportunities, such as greater access to delinquent peers and less adult supervision, 37 in addition to the explanation that adolescent males are more susceptible to deviant pressure as a result of gender socialization processes or as a means of better aligning with the masculine ideal. 38 For instance, Boyer and Byrnes 38 examined the frequency of various risk-taking opportunities, such as attending a party with alcohol, and discovered that teenage boys were more likely than teenage girls to report situational opportunities for deviance, which may have contributed to their higher risk-taking behavior. Males may simply have more social opportunities to experience deviant peer influence than females, rather than being more vulnerable to it if they report having more deviant peers than females.37,39
Internet addiction is defined by excessive or uncontrollably impulsive preoccupations, desires, or actions related to computer use or online access that impair functioning or cause suffering. Researchers and the general public have been paying increasing attention to the condition, and this focus has increased in lockstep with the expansion of computer (and internet) access. Males predominate in clinical samples and most pertinent surveys. Onset is said to happen in the late 20s or early 30s age range, and there is frequently a 10-year or longer delay between the first and problematic computer usage. 40 Our study reported no significant difference in sex on internet addiction which is consistent with Aboujaoude et al. 41
Lastly, our study also reported a significant correlation between internet addiction and depression. This finding is consistent with that of Ha et al., 42 who also reported a strong connection between teen depression and internet addiction. The temperament characteristics of the group with internet addiction supported this association. There is a genetic propensity for both pharmacological and behavioral addictions, according to a genetic study. According to the “reward deficit syndrome” notion, people who lack dopamine D2 receptors are more likely to engage in compulsive, impulsive, and addictive behaviors such as pathological gambling, alcoholism, and conduct disorders. 43 This association and coexistence 44 has been explored and reinforced by many other studies as well, 45 some of which are themselves correlational in nature. 46
Conclusion
Levels of depression and internet addiction have a strong positive link while depression also shows a significant difference in symptomatology and development patterns in adolescent males as compared to females.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The research conducted in this study was in accordance with ethical standards and guidelines. All procedures involving human participants were conducted in compliance with the ethical standards for research involving human subjects.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent Statement
Prior to participating in the study, all participants were provided with detailed information about the research objectives, procedures, potential risks, and benefits. Informed consent was obtained from each participant, and the consent process was carried out in Google form. Participants were presented with the form, which outlined the study’s purpose and the voluntary nature of their participation. They were given the opportunity to ask questions and seek clarification on any aspects of the study. Participants were assured that their personal information would be kept confidential and their anonymity would be maintained. Only after obtaining written informed consent from each participant were data collection procedures initiated.