
Abstract
Studies have shown physician homophobia as a barrier to health care, with LGBTQIA+ patients being more likely to delay or avoid getting care due to fear of harassment or discrimination.
Objectives:
Our aims and objective in this study were to determine the attitudes and opinions of the various medical and surgical teaching faculties and compare them for gender differences, if any, toward the LGBT community.
Methodology:
It was a cross-sectional study done among 129 teaching faculty between November and December 2019 at Sri Devaraj Urs Academy of Higher Education and Research, a rural tertiary medical college in southern India with regular and ongoing postgraduate training in all medical and surgical specialties, with assessment done using a structured and validated instrument, Riddle homophobia scale, meant for the assessment of attitudes and beliefs toward the LGBT community.
Results:
Most of the teachers in both the medical and surgical groups reported favorable positive attitudes/beliefs with statements like homophobia and heterosexism are wrong, and there is no need for the LGBT people to undergo reparative surgery; they deserve the same rights and privileges as everyone; however, there were negative attitudes and opinions reported with the statements like the LGBT people did not choose their sexual orientation and teachers themselves need to undergo introspection to be able to be supportive toward them, which is a significant source of concern. There were no differences in attitudes and opinions based on the age groups of the teachers of both the groups. Male teachers, when compared to female teachers (male:females—84:45), reported more favorable beliefs (t2/p value= 6.316/.0043) toward the LGBT community at p value ≤ .05.
Conclusions:
The teaching of sexuality, especially on the LGBT community, to medical professionals, especially teaching faculty, needs to be perceptive to the issues faced by people with different sexual orientations and identities.
Both the medical and allied sciences and the surgical and allied sciences teaching faculty had negative attitudes of repulsion and pity with uncertain attitudes toward taking a stance against the anti-LGBT community. Medical college teachers should be trained periodically with workshops and continued medical education programs regarding the sexual orientation of the LGBT community so that a practice with a non-judgmental approach and holistic treatment is delivered.Key Messages
Introduction
Rampant bias and discrimination toward the LGBTQ1A+ community exist, in society and healthcare, despite having come a long way in acceptance and inclusion. LGBTQ1A+ stands for lesbian, gay, bisexual and transgender, queer, intersex, asexual; with the 1+ indicating diverse other identities. 1 Lesbian and gay denote same-sex physical/romantic attraction; the former indicates women and the latter indicates people of all gender identities, but is usually associated with men. 2 The term bisexual denotes physical/romantic attraction for both men and women, while “queer” is an umbrella term used for non-conforming identities. In the fourth term, transgender people are those individuals whose gender expression does not conform to the sex assigned at birth. 3 Finally, asexual people, in general, are those who feel no sexual attraction at all; this is different from celibacy, in that celibacy is a deliberate choice. 1
These are all independent of each other: biological sex (gender assigned at birth), gender identity (a person’s innate identification as a man/woman/transgender/other), gender expression (external manifestation of gender identity which may or may not conform to societal norms) and sexual orientation (one’s physical, romantic, or other attraction or non- attraction to other people). 2
Homophobia is the fear, dislike, and hatred of same-gender relationships or those who love and are sexually attracted to the same gender. Homophobia includes prejudice, discrimination, harassment, and acts of violence brought on by fear and hatred. It occurs at all levels starting from schools on personal, institutional, and societal levels.
Heterosexism assumes that all people are or should be heterosexual and excludes the needs, concerns, and life experiences of lesbian, gay, and bisexual people giving advantages to heterosexual people. 4 Failure to grasp the concept that these are separate things leads to discrimination in society and the legal and healthcare systems. 5
In the Diagnostic and Statistical Manual of Mental disorders (DSM)-5 (2013), “gender dysphoria” replaced “gender-identity disorder,” and it explicitly stated that “gender non-conformity is not itself a mental disorder.” 6 It shifts the focus entirely to the distress many transgender people face due to gender non- conformity. It is more this distress and not their identity which leads them to seek medical, surgical, or psychiatric help.
A five-judge bench of the Honorable Supreme Court gave the verdict on September 6, 2018, stating that section 377 violated the fundamental rights. 7 The Supreme Court passed another landmark judgment (NALSA judgment) on April 15, 2014, upholding the legal rights of individuals to self-identify their gender as male/female/transgender, without having first to avail medical and surgical treatment. 8
The Disparity Model Toward Minorities
According to the “Minority Stress Model,” members of sexual or gender minority groups may experience distal stressors (like the experience of discrimination and violence) and proximal stressors (like the expectation of rejection, concealing true identity, and internalized homophobia). 9 This model is linked to poor mental, sexual, and physical health and decreases access to health care for minority populations. 10 LGBT individuals are 2.5 times more likely to experience depression, anxiety, and substance misuse than heterosexual individuals. 11 Twenty percent of sexual minority adults have attempted suicide compared to 4% for the general population. 12 Poor psychosocial health has further led to sexual risk-taking and a higher prevalence of HIV in these populations. 13
Negative attitudes prevent optimal utilization of healthcare services. Studies have shown physician homophobia as a barrier to health care, with LGBTQ1A+ patients being more likely to delay or avoid care due to fear of harassment or discrimination.14–16 There are limited studies from India, but they detail the discrimination faced by the members of the transgender community; for instance, there are reports of trans women given male gowns and admitted in male wards.16,17 In one study, participants (postgraduate medical and dental residents) ranked the Internet and newspapers higher than medical textbooks as sources of their ethics and knowledge. 18
Understanding the perspectives of teaching faculty and their perceptions toward the LGBT community can negatively affect their clinical practice, and as teachers imparting training to the future specialists in their respective specialties. This study kept in mind the limited resources with minimal access to the correct information, especially non-psychiatric clinicians and teachers. The study aims to assess the attitudes and opinions of teaching faculty toward the LGBT community and compare among the medical and surgical teaching faculty, especially in a rural tertiary medical college in southern India.
Methodology
The Institutional Ethics Committee approved this cross-sectional study proposal of the Institute. After obtaining approval, the study participants were the teaching faculty of both the medical and surgical departments with their allied subjects of Sri Devaraj Urs Medical College & Research Hospital, Kolar, and they provided written informed consent. We omitted teachers with a history of undergoing psychiatric treatment or drug dependence apart from nicotine. As per National Medical Commission (NMC) guidelines, we did not consider senior residents as teaching faculty for the study.
Half an hour of free time was identified for each of the units of the respective clinical departments, and we collaborated with the senior resident of the respective unit on that day of data collection.
Data collection went on for a few weeks. It was made sure that there would be no discussions between the specialists who had finished filling the questionnaire at different points of time, and confidentiality was maintained.
A semi-structured proforma sheet was first given to collect information about their social and demographic details and clinical experiences with the LGBT community. Later we administered the primary tool meant for the study, the Riddle’s scale.
The primary tool of the study was the Riddle homophobia scale, which Dorothy Riddle developed. It is an eight-term uni-dimensional Likert-type interval scale with nominal labels and no explicit zero points. Each term is associated with a set of attributes and beliefs; based on the attributes they exhibit and the beliefs they hold, individuals are assigned a position on the scale.
The scale used is divided into two parts: the “homophobic levels of attitude” (the first four statements of the scale served the purpose that Riddle originally had in mind, and the next four state the “positive attitudes” toward the LGBT community).
She devised the scale to explicate the continuum of attitudes toward gays and lesbians and assess the current and desired institutional culture of an organization or a workplace.
Statistical Analysis
Statistical software, namely, Statistical Package for Social Sciences 22.0 and R environment ver.3.2.2 (Boston, USA), was used for the present study’s descriptive statistics and inferential statistical analysis. Using Microsoft Word and Excel sheets, graphs and tables were generated. 20 The P-value of less than 0.05 was considered significant.
Results
Study Participants
Among the study participants, 84 were males, and the remaining 45 were females. Of 84 males, 60 (65.94%) belonged to surgery and allied sciences, and the remaining 24 belonged to medicine and allied departments. Out of 45 females, 32 (71.12%) belonged to the surgical group, and the remaining 13 (28.89%) were faculty from the medical group (Table 1).
Findings of the Salient Social-Demographic Profile of the Teachers.
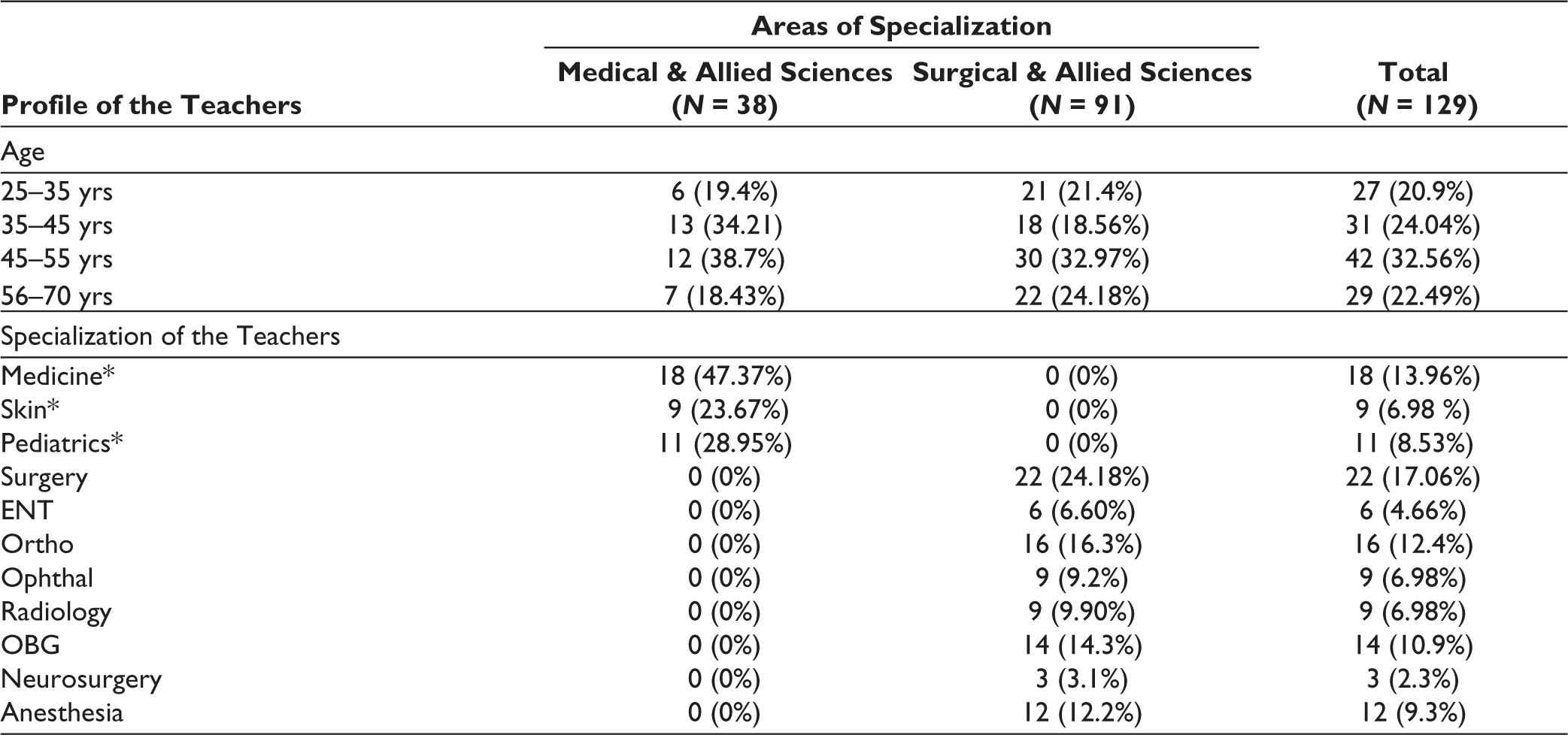
* = Medicine and allied subject teachers.
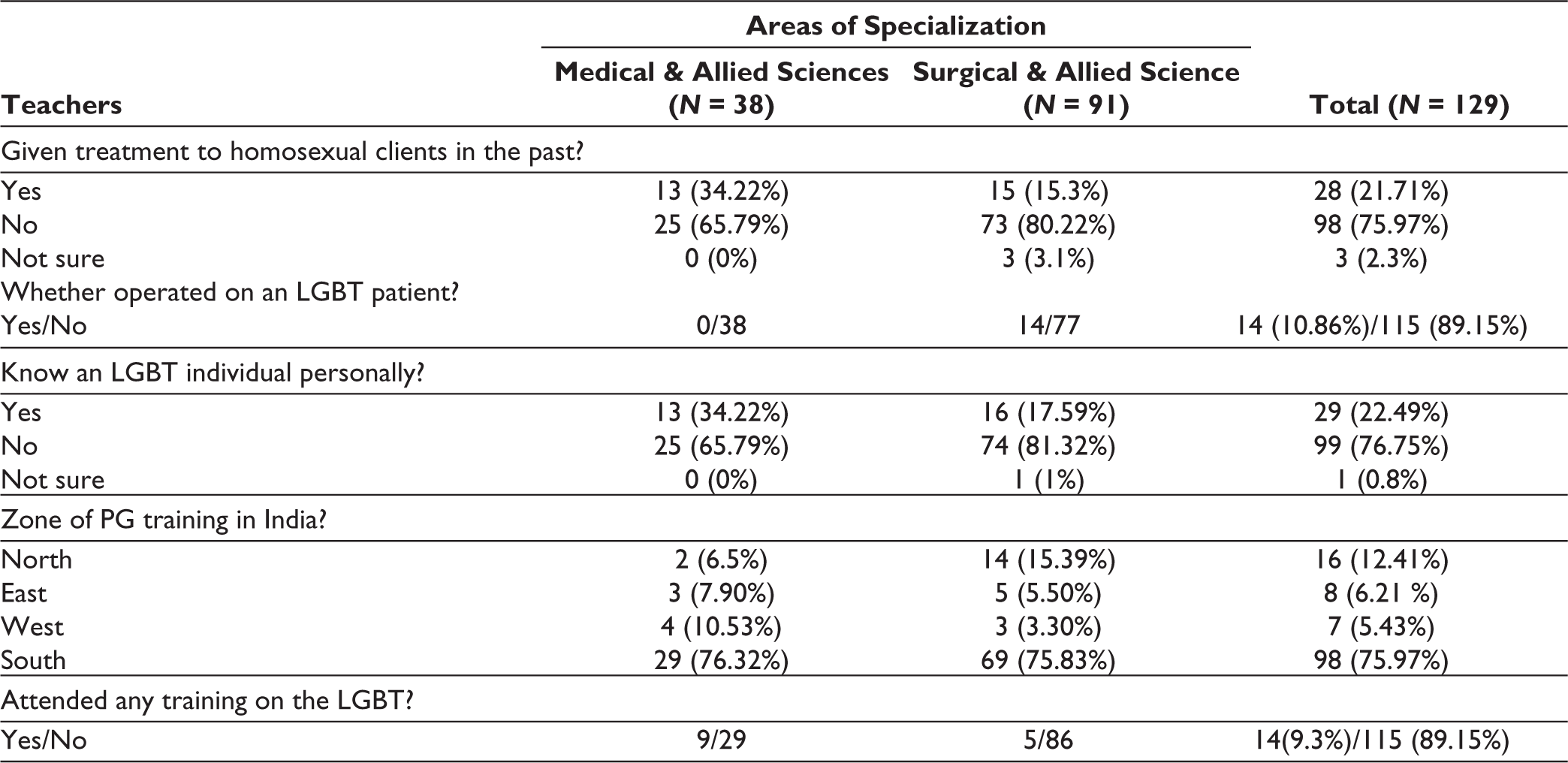
The majority of the teachers in both groups did their PG training in southern India. 34.22% of the medical doctors and only 15.3% of the surgeons reported treating patients with same-sex orientation. 10.86% of surgeons reported operating on transgender people only in non-genital areas. 23.69% of medical doctors and 5.1% of surgical doctors attended lectures/any special training on the LGBT population. 79.97% and 76.75% of teachers did not treat any LGBT patient and did not know anyone from the LGBT community. 89.15% of the teachers did not have training or attended any conference on the LGBT community in their clinical experience (Table 2).
Clinical Experiences of the Teachers Toward the LGBT.
Current Attitudes of Teachers in Both the Groups Toward the LGBT
The majority of teachers reported positive attitudes among the medical and allied sciences with surgical and allied groups with a median score of a minimum “4” (Agree) in items reflecting tolerance, acceptance, support, admiration, appreciation, and nurturance toward the LGBT community (Figure 1).
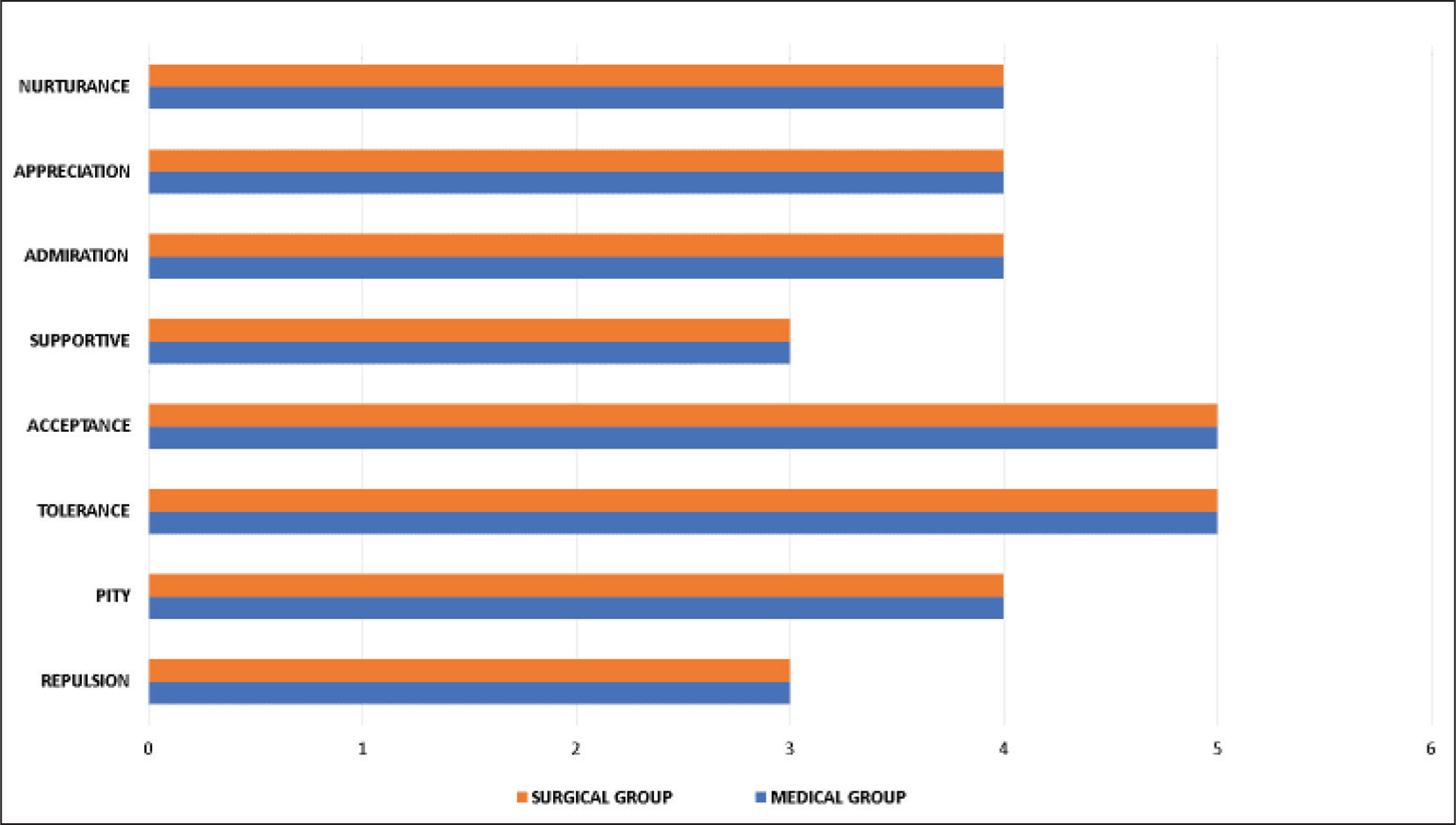
The significant unfavorable belief reported among the teachers was that the LGBT people did not choose to be the way they are inclined. The majority of the doctors in both groups reported a need for self-examination (introspection) to actively support them as an ally.
Uncertain responses to statements whether LGBT people need to undergo reparative therapy reflected repulsive attitudes. The statement that homophobia and heterosexism are wrong reflects a lack of a supportive attitude toward the LGBT in both groups (Figure 2).
Current Beliefs of the Teaching Faculty (Both the Groups)
Both the medical and surgical teaching faculty had a negative unfavorable belief that their personal feelings prevented them from accepting and supporting the LGBT community and accepted having significant gaps in understanding and growth to start accepting them. Despite reporting readiness (with medical group reporting higher readiness than the surgical group) to be an effective ally to the LGBT community, both groups did not have a solid belief to do so actively. There was no statistical significant difference among the teachers regarding the beliefs toward the LGBT community in both groups (Table 3).
Riddle Score-Descriptive Statistics: Current Beliefs Toward LGBT.

* = Indication of values rounded off to 2 digits.
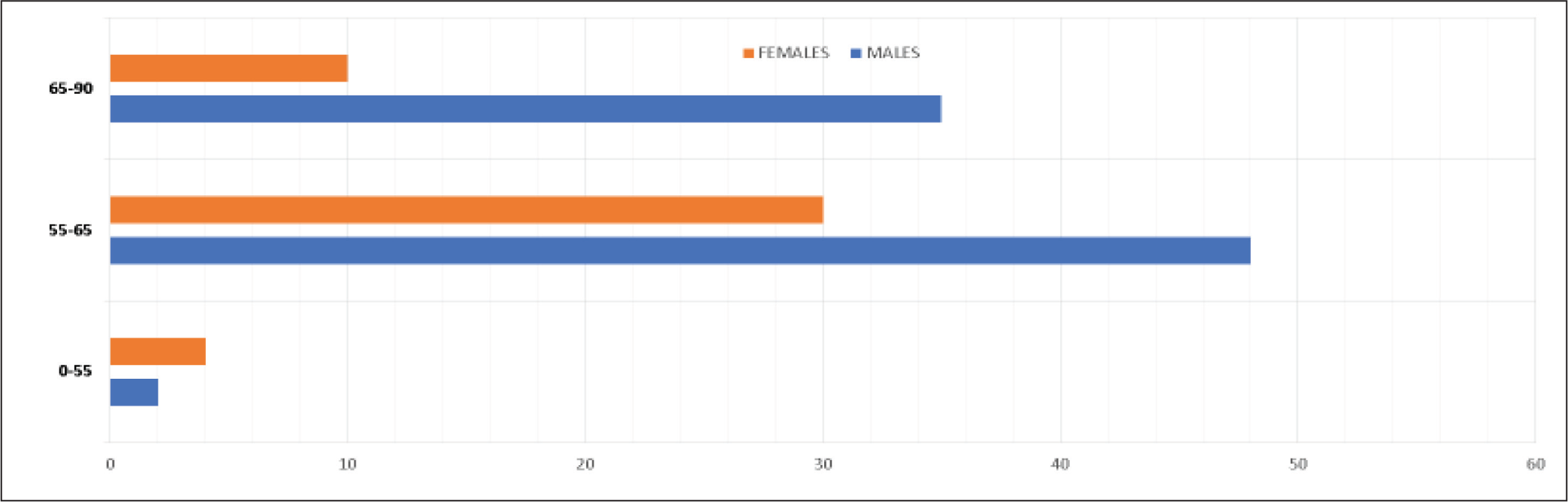
Riddle Score Distribution According to Age in Years Among Teaching Faculty.

Association was significant at a 5% level of significance.
Discussion
The major highlights of this study are that it is an important study in India assessing the attitudes and opinions of teachers training postgraduates in a tertiary multispecialty medical college. A qualitative study in the United Kingdom (UK, 2005) exploring the perspectives of the general practitioners (GPs) on the difficulties they faced when discussing sexual health with lesbian and gay patients in their clinics indicated that non-heterosexual orientation in the patients acted as a barrier, in almost 50% of the GPs. The difficulties were primarily related to the ignorance of lifestyles and sexual practices and also, due to their assumptions about relationships and concerns, the use of language toward the patients with the same-gender orientation. 21 However, in our study, neutral responses (uncertain) for attitudes toward the LGBT of homophobia and heterosexism were found in the teachers’ medical and surgical groups.
This uncertainty could be because of the age of the faculty, as more than half of the teachers’ samples were older than 45 years. They had completed their PG training at least a decade earlier, and 89.15% of teachers did not have any training or attended any conference on the LGBT community in their clinical experience.
Like patients, even the health professionals of the LGBT community reported having faced difficulties in an online survey of 427 physicians from a national healthcare organization.
A snowball study sample from the database at the worksites found 10% and 15% of the LGBT doctors being denied referrals from heterosexual colleagues and faced harassment by colleagues.
Twenty percentage of the LGBT physicians felt socially ostracized, 65% received derogatory comments, and 34% witnessed discrimination of LGBT patients. 36% witnessed disrespect toward an LGBT patient’s partner, and 27% had witnessed discriminatory treatment of an LGBT co-worker. 22
In a three-time survey conducted at the San Diego County medical community in California, USA, 2008, evaluation of the same physicians at different periods found that early year of graduation, male gender, and heterosexual orientation were significant predictors of stigma-associated responses, which showed substantive decline in attitudes toward sexual minorities and HIV-positive people only after 35 years.
A study on medical professionals (2011) 23 of males and religious participants who faced more stigma due to their homosexual orientation was conducted in Europe.
In contrast, our study found that male teachers had a favorable attitude compared to female teachers. However, our sample size in the study had almost double the sample size of males compared to females (84:45). This unequal representation could attribute to the statistically significant difference.
We did not find any statistical significance in attitudes based on the age group among the teachers in our study toward the LGBT community (Table 4). We did not look for any role of religion in doctors toward the stigma of the LGBT community, unlike the European study.
Male faculty reported favorable responses in this study, which could be due to the rural location of our hospital. Transgender people and homosexuals are more comfortable with males than females in their approach, usually for satisfying the sexual pleasure of males, as it is prevalent in our Indian societies. It is a common scenario in all road traffic signals and in trains all over the country, where we find these people asking for money mostly from males only. Why these trans-genders avoid requesting or demanding money from females needs evaluation in a large-scale study. Is it jealousy toward females or fears of being ostracized more from them, a shared public perception that needs evaluation?
Hijras (trans-genders) in South India do not have the same cultural role as their counterparts in North India, and most of them take up sex work to earn a living. Most of them also make a living by singing and dancing at weddings or in welcoming childbirth functions, and the rest of them make a living by begging.
Tamil Nadu and Kerala are the first Indian states to introduce a transgender person (Hijra/Aravani) welfare policy, under which transgender people can access free sex reassignment surgery in government hospitals (only male to female) with proper documentation. 24
According to the studies conducted by Herek in 2002 and 2006, US25,26 reported that older people are more prone to stigmatizing homosexuals and bisexuals than younger people. However, in this study, we did not find any significant difference in attitudes across various age groups of the teaching faculty (Table 4).
Both the medical and the surgical teachers reported uncertain/neutral response regarding the need for reparative therapy for the LGBT community. This uncertainty could be due to the popular stereotypes and myths related to gender minorities among clinicians. This uncertainty among teachers training postgraduates currently is a significant concern as conversion therapy is prevalent for “treatment” of homosexuality, with practitioners asking large sums of money for the same. They offer aversive therapy, electroconvulsive therapy, psychotropic medication, and even religious texts to guarantee time-bound, complete conversions. 27 Such practitioners have also propagated baseless notions about hormonal, genetic, and psychological “reasons” for homosexuality.
In July 2018, the Indian Psychiatric Society stated that “there is no scientific evidence that sexual orientation can be altered by any treatment” and strongly supported the “decriminalization of homosexual behavior.” 28
Conclusion
Health care disparities in sexual minorities can be eliminated if clinicians elicit information about sexual orientation and gender identity from their patients through thoughtful, non-judgmental discussion and history taking. 29
Continued medical educations and online training could be a good way for practicing clinicians to sensitize them to the LGBT issues and bring them up to speed about hormonal and surgical treatments for transgender individuals, prevention and treatment of HIV/other STDs, and other health needs of the community. 5 Clinical services for people with such issues and concerns need to be sensitive to holistic care.
A positive and non-judgmental attitude will go a long way in relieving distress among the LGBT community instead of pathologizing their identities.
Teaching sexuality to physicians and surgeons needs to be perceptive to the issues faced by people with different sexual orientations and identities.
The emphasis should be on education and a change of attitude among the clinicians. Developing and disseminating clinical practice guidelines are also essential. 30
Limitations of the Study
Our study sample was small, with an unequal number of medical and surgical teachers working in a rural setting that caters mainly to a low-income group. The findings cannot be generalized to teachers across the entire country.
The Riddle scale has been considered acceptable face validity as a psychometric scale, but its exact psychometric properties are unknown.31,32
WE DON’T FALL IN LOVE WITH THE GENDER. WE FALL IN LOVE WITH THE PERSON
Footnotes
Acknowledgements
The authors would like to profusely thank the entire teaching faculty who participated in the study, with special thanks to Mr. R. Ravishankar, Assistant Professor, Department of Community Medicine, SDUAHER, for his expert statistical inputs.
Declaration of Conflicting Interests
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical committee approval was taken from Institute ethics committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the participants who were the teaching faculty of both the medical and surgical departments with their allied subjects of Sri Devaraj Urs Medical College & Research Hospital, Kolar.