
Abstract
Background:
The patient’s understanding of the illness may mediate beliefs towards its treatment. There is a paucity of studies examining the relationships between these variables in depression. This study was conducted to know the relationships between explanatory models and attitude to medication in depression.
Methods:
494 patients with depression in remission were assessed with sociodemographic proforma, Drug Attitude Inventory, and Mental Distress Explanatory Model Questionnaire.
Results:
A favorable attitude toward medication was observed in 57.49% of participants. Mean scores on MDEMQ subscales Stress, Western Physiology, Non-Western Physiology, and Supernatural were 32.96, 21.87, 10.06, and 47.55, respectively. Statistically significant associations were found between attitude towards medication and the patient’s marital status (more negative attitude with single status, χ2 = 11.72, df = 3, P = 0.008) and occupation (more negative attitude among unemployed patients, χ2 = 4.17, df = 1, P = 0.041). The scores of explanatory models did not differ based on positive or negative drug attitude.
Conclusion:
Though explanatory models are not linked to patient attitudes toward medication, patients who are single or unemployed have a negative attitude toward medications. Such negative attitude may impair compliance and worsen patient outcomes.
Keywords
While illness-related causal attributions do not appear to be associated with patients’ attitudes toward medication in depression, unemployed and unmarried patients may have negative attitudes toward medication that should be addressed appropriately.Key message:
Of all mental illnesses, in India, depression is the most common and leading cause of disability-adjusted life years (DALYs).1, 2 Noncompliance is common in patients with depression, increasing the risk of recurrence, morbidity, caregiver burden, and avoidable medical costs.3, 4, 5 Only one-fifth of depressed patients seek treatment, while the rest suffer.6, 7, 8 The World Health Organization recommends performing additional research on variables affecting compliance, to understand depression better. 4
Explanatory models (EMs) are causal attributions made by patients, their families, or practitioners for a specific episode of illness. Culture, prior knowledge of causation, perception, experiences, and traditional beliefs influence EM, impacting treatment. 8 The EM is shaped by Indian culture and traditional ideas, distinguishing it from its western counterparts.9, 10 The commonest EM of depression in India is “stress” and “supernatural,” followed by Western physiology and Non-Western physiology.9, 10, 11, 12 EM affects treatment-seeking behavior and coping.13, 14, 15 Despite nonmedical EM’s prominence, a study found a link between these models and drug adherence. 12 However, small sample size constrained the Indian studies on EMs.
In India, pharmacotherapy is a commonly used evidence-based treatment for depression. 16 Medication use results in developing a wide range of attitudes about it (drug attitude), which are determined by knowledge of the illness, adverse drug events, and stigma. A positive attitude toward medication is associated with a longer duration of drug usage and increased use of over-the-counter medications. 17 On the other hand, negative attitudes toward drugs are associated with partial or complete avoidance, which results in a relapse of the disorder.18, 19, 20 Petelinšek and Korajlija reported that patients’ negative attitudes toward medication might reach over 80% due to various factors, including preferences for Ayurveda and Homeopathy.21, 22, 23 According to a study, Indians have a mixed attitude towards medication, 24 similar to observation among Australians of a negative attitude for the risk of dependency, and a positive attitude for improvement. 25 However, these studies were constrained by their small sample sizes and limited to individuals experiencing their first episode of depression.
In India, very few studies have been conducted on the relationship between EM and drug attitudes. There is no discernible link between EM and attitudes about medication.26, 27A western study demonstrated a biological model for having a favorable attitude toward antidepressants and a psychological model for having a negative attitude toward them. 28 Given that depression is India’s most prevalent mental disorder, research is warranted to examine such a link. This information may assist physicians in gaining a better understanding of patients’ perspectives on depression and its treatment, enabling more targeted interventions that improve overall outcomes. We hypothesized that nonmedical models are associated with a negative attitude toward drugs.
Materials and Methods
This cross-sectional study was conducted at an outpatient psychiatry department in a tertiary care center in South India. The study population consisted of remitted depression patients who lived in the community and visited the study center for follow-up between March and November 2020. An Institutional Ethics Committee approval was obtained before conducting the study.
The estimated sample size for this study was 194. Sample size was estimated using correlation sample size calculating formula: [(Zα+Zβ)/C]2 + 3 (Zα = The standard normal deviate for α; Zβ = The standard normal deviate for β); C = 0.5 × ln[(1+r)/(1–r)] 29 ; assuming α = 0.05, β = 0.20, and r = 0.20. A total of 624 consecutive patients were screened; 494 met the eligibility criteria, consented to participate, and were included in the study.
Patients of either sex were eligible for inclusion if they were 18 years or older, had been diagnosed with depressive episodes according to the International Classification of Diseases, Tenth Revision (ICD-10), were in remission according to the treating psychiatrist, and had a < 8 score on the Hamilton Depression Rating Scale
30
(score more than 8 indicates the presence of depression). In this study, remitted depression was considered, as the altered mental state associated with depression may influence attitudes toward medications and causative attributions for illness. Subjects with a history of chronic physical disease, unexplained medical complaints, mental retardation, or dementia were excluded, based on the information provided by patients on diagnoses made by any physician and the case record file. Subjects having a score of >7 on the General Health Questionnaire-12
31
were also excluded. This tool has been used to screen for mental health problems. The cutoff mentioned above has been used as a criterion for having a mental health problem in the Indian population.
31
Because a score greater than the cutoff indicates the presence of mental health problems, it may affect attitudes toward medications and causative attributions of illness; hence, they were excluded from the study. The following tools were used to evaluate all participants who met the selection criteria, in the following order:
Sociodemographic pro forma designed for this study: The pro forma consisted of sex, education, religion, marital status, residence, occupation, socioeconomic status, any preference for a specific medication, and history of self-medication. Drug Attitude Inventory (DAI): It was used to assess drug attitudes.
32
It is a self-administered inventory that assesses drug attitudes based on opinions about prescribed medications. The DAI is a 10-item true/false scale with a +1 for a correct response and a –1 for a wrong answer. The sum of the total determines the final DAI score. A positive overall score indicates a favorable attitude toward medication, whereas a negative overall score shows a negative attitude. The instrument has been used in the Indian population before.
20
In this study, the tool was administered in English. All participants who were not fluent in English were assisted in completing the inventory by a trained mental health professional. Mental Distress Explanatory Model Questionnaire (MDEMQ): It was used to ascertain the patients’ perceptions of the causal attribution of their mental illness. It has 45 items, each with a 5-point (1–5) assessment. Each item has a response option of “not likely at all” to “highly likely.” The items can be clustered into four explanatory categories (with a possible score range)—Western Physiology (9–45), Non-Western Physiology (4–20), Supernatural (19–95), and Stress (13–65). The lowest possible score is 45, and the highest, 225. The tool has acceptable reliability and validity.
33
This tool was chosen for this study because it examines many EMs comprehensively, Indian subjects participated in the initial validation of the scale, and it is easily administered. In addition, this tool has been used in the Indian community.
12
The data were analyzed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, N.Y., USA). Analysis of demographic variables and EMs was done with descriptive statistics. Crosstabulation analysis was performed to determine the relationships between demographic variables and DAI score, whereas the Mann–Whitney U-test was utilized to determine the relationships between drug attitude and EM score. The level of statistical significance was 0.05.
Results
A total of 624 people were assessed, with 494 of them giving their consent and enrolling in the study. The demographic characteristic of the study sample was characterized by the majority being Hindu, female, employed, from rural domicile, and from lower socioeconomic status. The mean age was 38.55 (SD = 13.37) years. More subjects had a preference for modern medicine, a history of self-medication, and a positive attitude towards medication. The MDEMQ subscales Stress, Western physiology, Non-Western physiology, and Supernatural had mean scores of 32.96, 21.87, 10.06, and 47.55, respectively (Table 1).
Sociodemographic and Clinical Features and DAI Scores
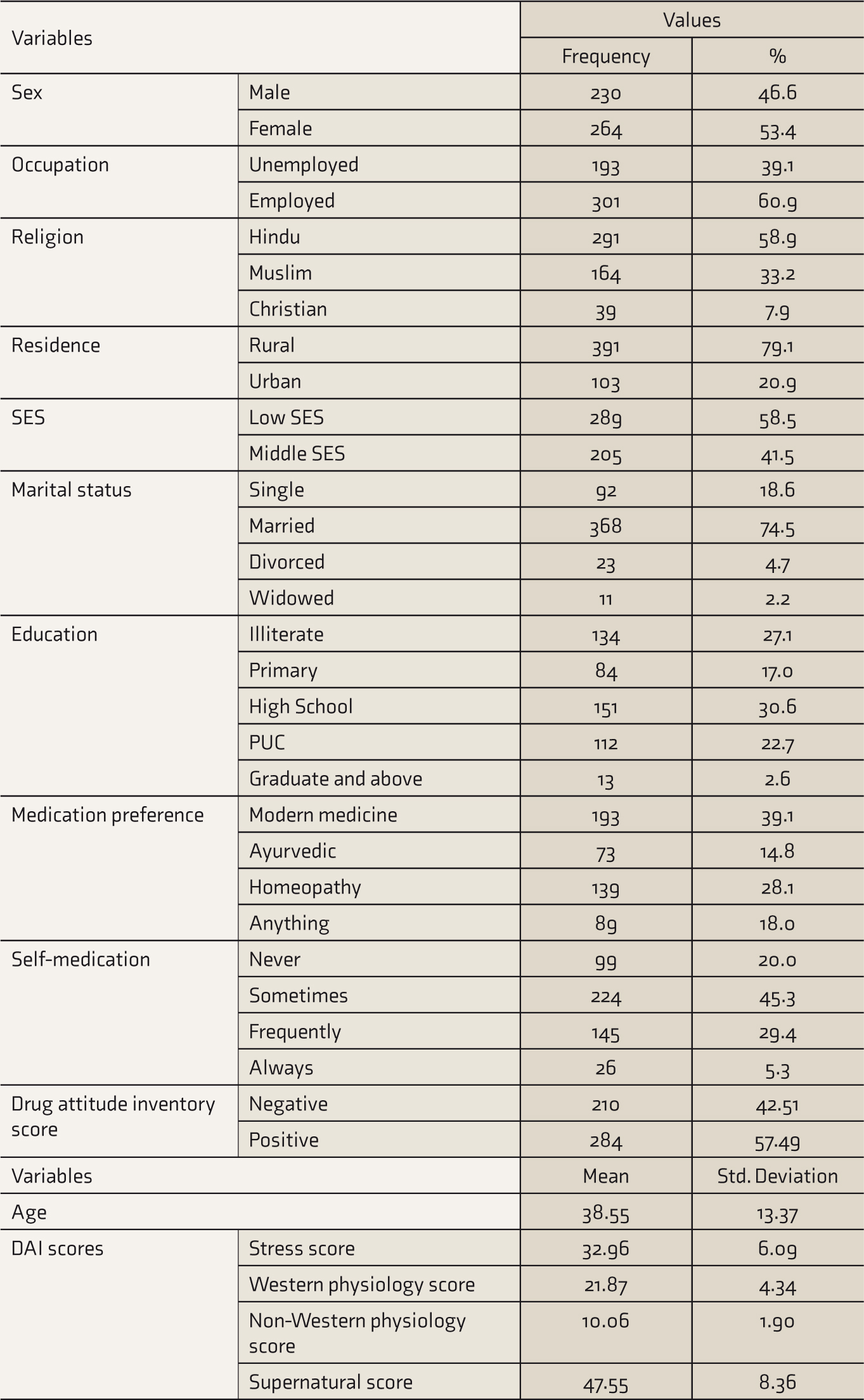
DAI: drug attitude inventory; SES: socioeconomic status.
A crosstabulation analysis was used to determine relationships between demographic characteristics and DAI score. The majority of the married patients (n = 217) had a positive attitude towards the drug, while single ones (n = 92) had a negative attitude (n = 51). Though statistical significance was found between all marital status sub-variables and attitude toward the drug (χ2 = 11.72, df = 3, P = 0.008), in post hoc analysis, a significant group difference was observed between positive and negative attitude toward the drug and single status only (adjusted P = 0.02). There was also a statistically significant relationship between occupation and the DAI score (χ2 = 4.17, df = 1, P = 0.041), with unemployed individuals having a less positive attitude than employed. However, the adjusted p-value for any occupation subvariable was not statistically significant (adjusted P = 0.08). The relationships between demographic variables and DAI scores have been presented in Table 2.
Relationships of Demographic Variables and Drug Attitude
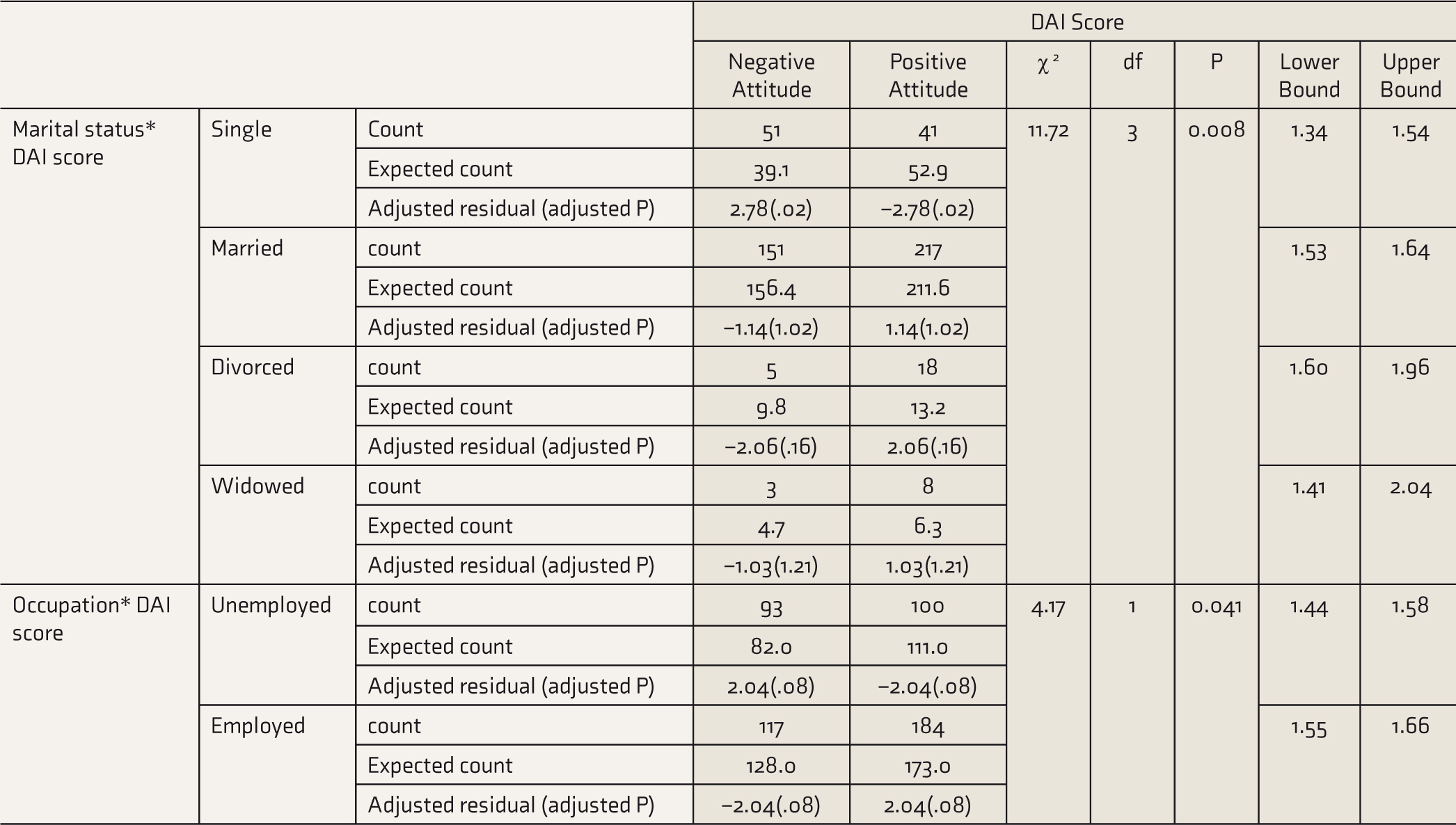
DAI: drug attitude inventory.
Mann–Whitney U-test was used to determine the group differences in the score of EMs subscales (Stress, Western physiology, Non-Western physiology, and Supernatural) based on positive and negative drug attitudes. The drug attitude and scores on Stress (P = 0.542), Western physiology (P = 0.623), Non-Western physiology score (P = 0. 233), and Supernatural (P = 0. 397) were all statistically nonsignificant. The relationships between the EMs and the DAI score are presented in Table 3.
Relation Between Explanatory Models and Drug Attitude
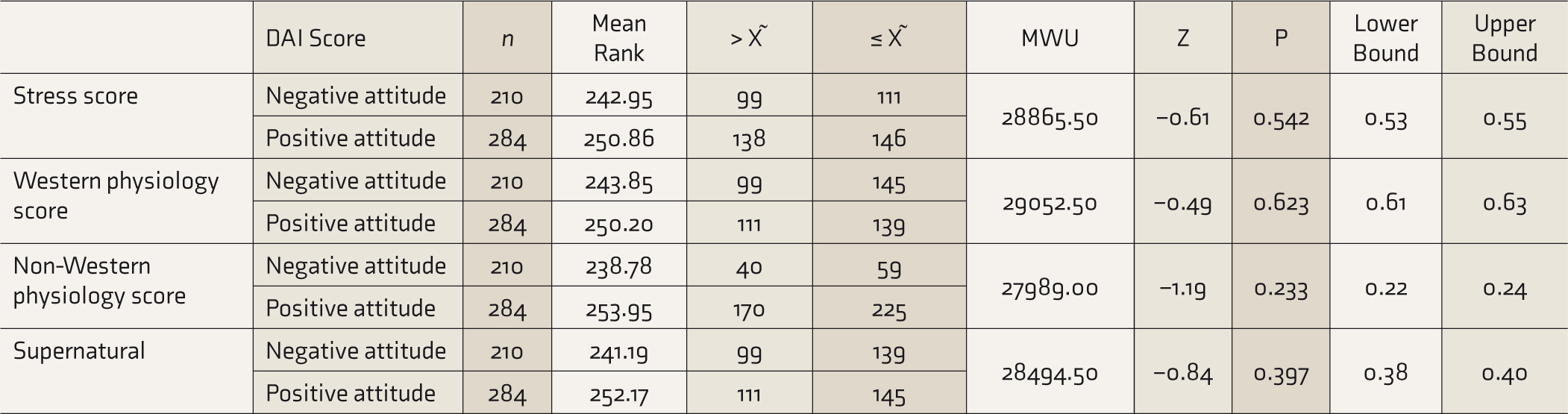
DAI: drug attitude inventory, MWU = Mann–Whitney U, X ˜= median.
Discussion
The study assessed the levels of EMs and their relationships with attitudes toward medication in patients with depression treated in a tertiary care setting. The findings indicated that a considerable proportion of subjects with single status had a more negative attitude than those married or divorced. Similarly, the unemployed had a more negative attitude, while the employed had the opposite. However, there were no significant relationships between any EMs and the drug attitude scores.
This study’s demographic characteristics were similar to another Indian report on EMs in depressed individuals. 12 Surprisingly, roughly 40% preferred non-evidence-based pharmacotherapy to evidence-based pharmacotherapy. A study that looked at such preferences among people with mental illness (not only depression) came up with a similar result. 34 Such preferences appear to be based on the patient’s perceptions of infrequent adverse effects associated with ayurvedic or homeopathic medicine. 35 The prevalence of self-medication is consistent with a meta-analysis that indicated that a comparable proportion frequently self-medicates for minor symptoms such as headaches. 36 In this study, the Stress score was higher than in the prior report, but the other subscales had lower scores. 12 This could be because the sample size for the study was different. As with the previous report, most respondents had a favorable attitude toward medication, 20 which could be because subjects with a favorable attitude sought the service of the tertiary care center.
Employed individuals had more positive attitude, consistent with a previous report. In a five-year prospective study, Holma et al. observed that employment status predicted a favorable attitude toward antidepressant medication, most likely because it is associated with a larger social network. 37 In addition, employed individuals are more likely to be educated, which has been shown to influence medication perception and the impact of illness12, 38 and improve mental health literacy.39, 40 The treatment may have aided in resolving their employment-related concerns following an overall improvement in symptoms and quality of life. 41 Additionally, the study found that single people have a considerably lower positive attitude about drugs. Similar trends have been reported from India, 20 while some reports did not establish such link. 20 The latter study covered diagnoses other than depression; thus, the disparity in outcomes is likely, as Roopun et al. also had a similar observation. 42 Holma et al. also found no statistically significant association between medication attitude and marital status, despite the latter being related to improved medication adherence. 37
Inconsistent with our hypothesis, this study found no significant relationships between EMs and drug attitudes. This finding contrasts with a previous report conducted in the same geographical location, which found that a sizable proportion of people lack a medical model and would not seek treatment from a psychiatrist. 43 However, it was constrained by small sample size. There does not appear to be a single explanation for this observation. Firstly, the study was conducted in a tertiary care center during the COVID pandemic, and the study sample does not truly represent the community population with depression. Thus, those with a negative attitude toward medication and those with a nonmedical model may have made insufficient effort to go to the tertiary care facility due to the government’s implementation of the COVID-19 safety guideline. Only severe cases may have approached for the treatment in the later stages of illness.9, 41, 44, 45 Those with less severe symptoms may have approached other healthcare resources in accordance with their prevailing EM. Second, because most of the respondents in this study came from rural areas and are therefore more likely to have a nonmedical model of illness, they came to the care center with the expectation of recovery. Depending on their EMs, such as indigenous treatment and faith healers, they may have exhausted their care resources prior to reaching the tertiary care center.46, 47 Third, the improvement they saw in their symptoms may have acted as a buffer against a negative attitude toward medication. Patients who do not respond to medicine may develop a different attitude about drugs. Fourth, the majority were literate and employed, and this may have influenced their health concerns and treatment-seeking behavior to obtain standard health care, as they wanted the symptoms to be addressed quickly, to lessen the impact of illness.
Based on these findings, it is possible to conclude that EMs are unrelated to patient attitudes toward medication. However, unmarried and unemployed patients have a negative attitude. The finding implies that unemployed and unmarried patients should be addressed appropriately for their drug attitude. A negative attitude toward medications may impair compliance, thereby adversely affecting the outcomes of depression treatment. The finding of this study should be taken with caution as it was conducted during COVID-19 pandemic and may not represent the patient population of the nonpandemic normal situation. Other limitations of the study were that it was institution-based, had cross-sectional design, and lacked a control group. More research is needed to corroborate the findings by resolving the study’s limitations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.