
Abstract
In India, the prevalent stigma and taboos regarding sexuality prevent adolescents from acquiring information about sexual and reproductive health. This review assessed the school-based interventions for adolescents designed to enhance their sexual health knowledge, attitudes, and behaviors. Studies were gathered from 4 online databases: PubMed, DOAJ, Google Scholar, and ScienceDirect. Relevant studies conducted in India among adolescents, published in peer-reviewed journals between 2000 and 2020, available in the public domain and written in English, were considered for the review. 14 studies were selected through database searches that fulfilled the eligibility criteria. Findings highlighted that school-based sexuality education positively influences adolescents to develop their knowledge, attitude, and behavior related to sexual and reproductive health outcomes. Sexual and reproductive health (SRH) programs and interventions are limited to small-scale experiments conducted in a few schools. The researchers recommend educating adolescents about pregnancy prevention, sexually transmitted infections (STIs), sexual hygiene, and reproductive health. Comprehensive reproductive health education programs should be implemented in every school setting to ensure that all school-going adolescents are convinced of the importance of sexual and reproductive health.
Introduction
International concern about young people’s sexual and reproductive health (SRH) has risen in recent years. 1 Despite tremendous advances in implementing SRH services in most countries, young people continue to be disproportionately served by these services. 2 In the United States, one in every 4 sexually active teens has a sexually transmitted illness, and 3 million females between the ages of 15 and 19 are subjected to unsafe abortions each year. 3 According to the sustainable development goals (SDGs; target 3.7), universal access to reproductive health care should be achieved by 2030. However, the availability of SRH information and services in many low and middle-income countries (LMICs) is restricted.4, 5 In a survey of 70 LMICs, nearly all nations indicated that only 10% or fewer of all teenage women visited a health center in the previous 12 months and received family planning information. 6
In the Indian cultural context, sexuality, sexuality education, and public discourse on sexuality are stigmatized and taboo. 7 SRH is a crucial factor in achieving the global developmental goals related to poverty, gender equality, and education for positively altering the destiny of future generations.8–10 Adolescents account for one-quarter of India’s population, making it the country with the largest adolescent population in the world. 11 According to World Health Organization, adolescents fall into the age group of 10 to 19 years. 12 Access to reliable information and services related to SRH is vital for adolescents’ health and well-being,13, 14 as this phase of life marks an individual’s initial explorations in sexuality.15, 16 Good SRH is possible only through a respectful and positive approach toward sexuality, sexual rights, and sexual relationships free from violence, discrimination, and coercion.
Studies indicated that the knowledge of adolescents regarding SRH is relatively low.17, 18 High teenage pregnancy rates indicate high levels of unprotected sexual activity among adolescents.19, 20 Early marriage, high in India, has adverse effects on women’s reproductive health status. 21 Many teenagers do not have accurate information on contraception or pregnancy prevention, and sexu ally transmitted infections (STIs). 22
Girls are subject to severe discrimination in India. 23 Menstrual hygiene, which is crucial in predicting the occurrence of reproductive tract infections, has been highlighted as a potential risk factor for SRH among adolescent girls in India. 24 While experiencing trouble with menstruation, girls keep missing school, self-medicating, and refining from social contact rather than seeking medical advice. 25 These girls are often steered by limited knowledge from mothers who, because of low literacy and socioeconomic status, lack awareness of reproductive health and hygiene.26, 27
Additionally, STIs pose a significant health risk to sexually active individuals. 28 In general, the studies have shown low understanding and familiarity with STIs except for human immunodeficiency virus (HIV) infection. 29 Inadequate awareness about STIs leads to delays in diagnosis and treatment.30, 31
Young people are more susceptible to abuse. Child sexual abuse involves a wide range of activities, such as fondling, inciting a child to engage in sexual contact with another person, sexual intercourse, and other forms of sexual display, as well as the involvement of a child in illegal activities like prostitution or the production of pornographic materials. The Protection of Children from Sexual Offenses Act (POCSO), passed in India in 2012, aimed at safeguarding minors from various sorts of sexual abuse, harassment, and pornographic imagery and mandates reporting to any instances of child sexual abuse. 32 It is a gender-neutral law. Section 43 of the act mandates that the federal government and each state government take all reasonable steps to publicize the act’s contents and offer training to government personnel to guarantee its implementation. 33 However, it is regrettable that it does not include any instructions for educating teenagers about sexual health issues. Globally, around 35% of women experience violence in their lifetime. Based on the Crimes in India Report, 2019 by National Crime Records Bureau, there is a 7.3% hike in crimes against women compared to the previous year. 34 As a consequence of violence, women experience poor social, mental, and physical well-being and health. 35
The advances in technology and widespread use of the internet have changed how young people learn about sexuality, bringing exposure to potential threats such as internet bullying, sexting, and online abuse. 36 Smartphones are emerging as a new way of seeking information on sexuality by surfing through pornographic content. 37
Knowledge is a vital prerequisite for lowering sexual health risk. 38 Formal sexuality education programs significantly enhance sexual health knowledge, attitude, and behavioral change. 39 Sexuality education helps minimize menstrual discomfort, shame, and the likelihood of potentially adverse consequences from sexual behavior, like unintended and unexpected pregnancies and sexually transmitted diseases (STDs).40, 41 Similarly, sexuality education helps to promote a respectful and positive attitude toward sexuality, gender, and relationships. With comprehensive sexuality education, convenient medical facilities, and enhanced socioeconomic conditions, a holistic approach is most likely to promote SRH among adolescents.42, 43
Sexuality education is not a recent endeavor to support young people’s sexual health and well-being. Schools act as a space for generating and communicating knowledge about sexuality among adolescents. 44 Sexuality education at schools acts as a social vaccine by propagating the authenticated information, thus inhibiting the disseminating of wrong information on human sexuality among adolescents. 45 In addition to being the place where many adolescents congregate, schools are also controlled settings that are excellent for the cost-effective implementation of any interventions targeting adolescents.16, 46 Nevertheless, many teachers rarely discuss sexuality in classrooms. 47 In this scenario, this review aims to collect, sum up, and critically evaluate the peer-reviewed scientific studies on the school-based interventions implemented by nongovernmental organizations, medical institutions, voluntary organizations, and individual researchers on SRH and their outcomes associated with SRH knowledge, attitude, and behavior among adolescents in India. Further, an attempt has been made to understand the content/topics, target population, human resource involved, duration, and the delivery methods utilized in these interventions.
Methods
This review is intended to amass an extensive range of published studies that have used different methodologies to explore the effectiveness and variables affecting SRH education of adolescents in school settings.
Search Strategy
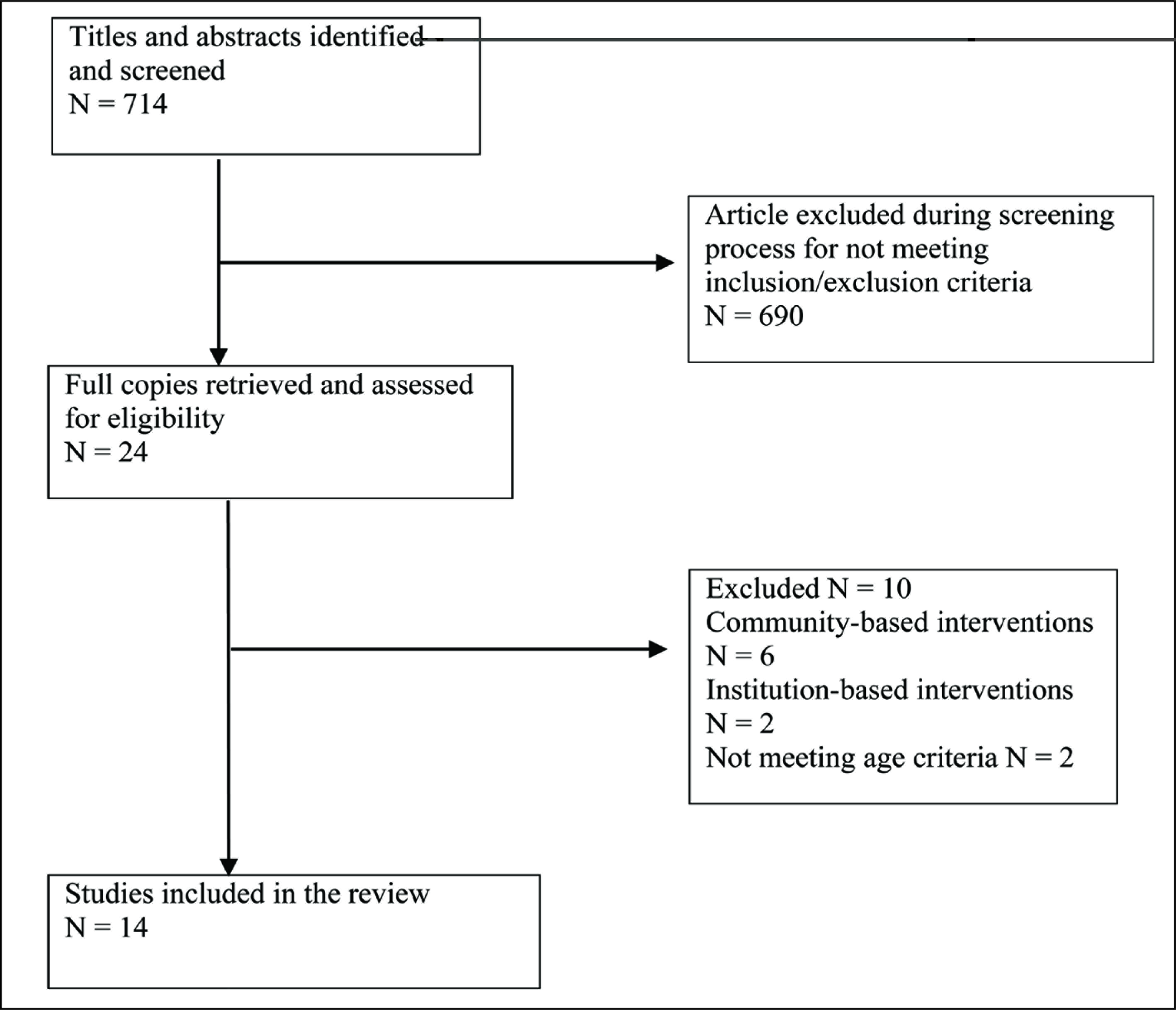
The review explored many studies related to SRH outcomes at schools; however, only those papers that were compatible with the study objectives remained for final review. Studies for review were collected from 4 online databases: PubMed, DOAJ, Google Scholar, and ScienceDirect. The following keywords were used for searching: sexual health or reproductive health, adolescents or teenagers, intervention or education or program, school, and India. The titles and summaries of the studies found through the search strategy were screened against inclusion and exclusion criteria (Table 1). Setting these parameters allowed receiving 714 articles. The duplicates were removed, and abstracts were scrutinized for relevancy. 14 articles that were identified meeting the inclusion criteria were chosen for the final review (see Figure 1).
Inclusion and Exclusion Criteria
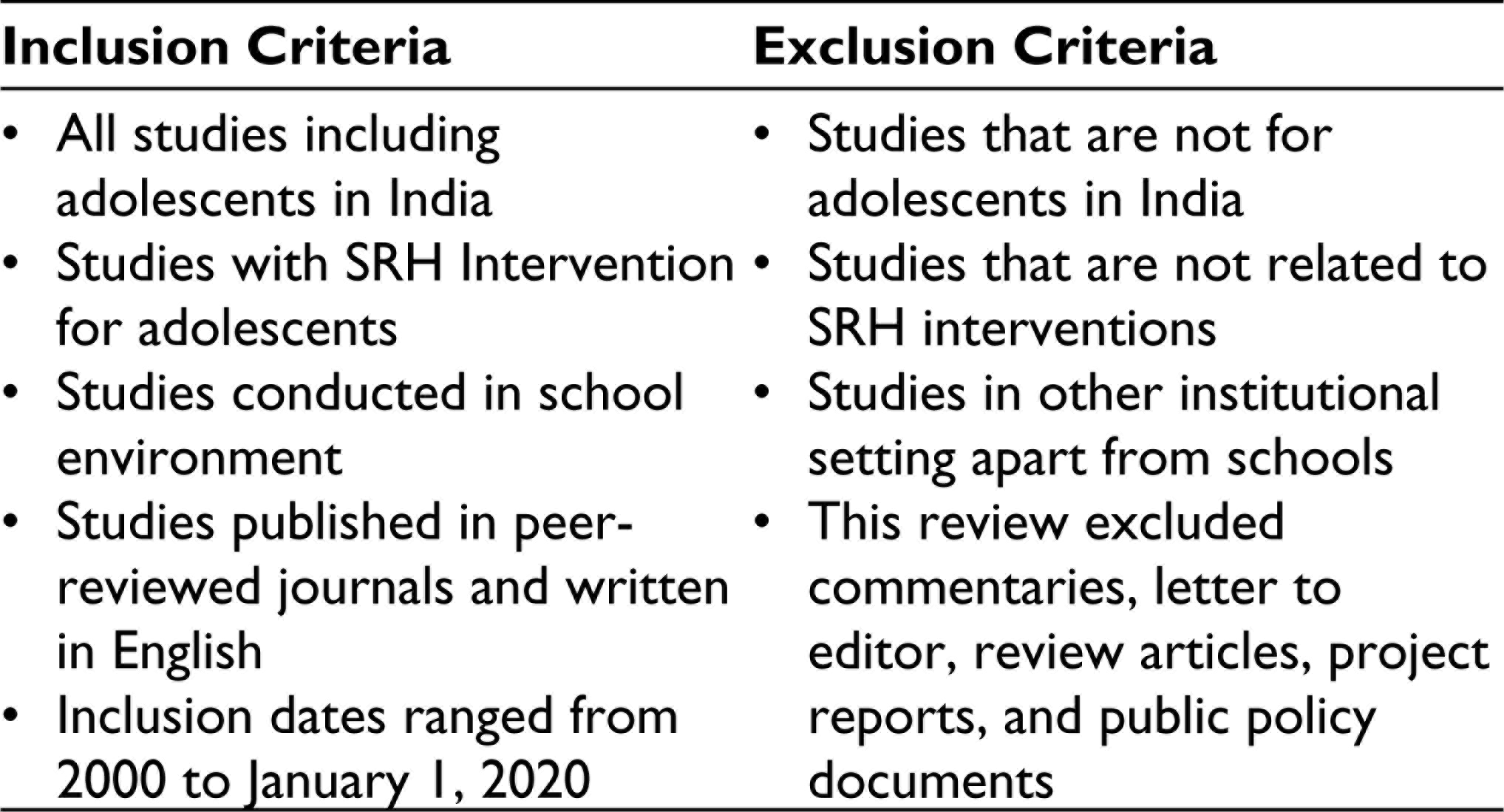
Study Selection Flowchart
Data were extracted and charted based on objectives, study design, execution (intervention package/content, target group, and human resources), findings (outcomes), and limitations. The resultant analysis summarizes the effect of school-based education on sexuality in terms of knowledge, attitude, and behavior outcomes.
Findings
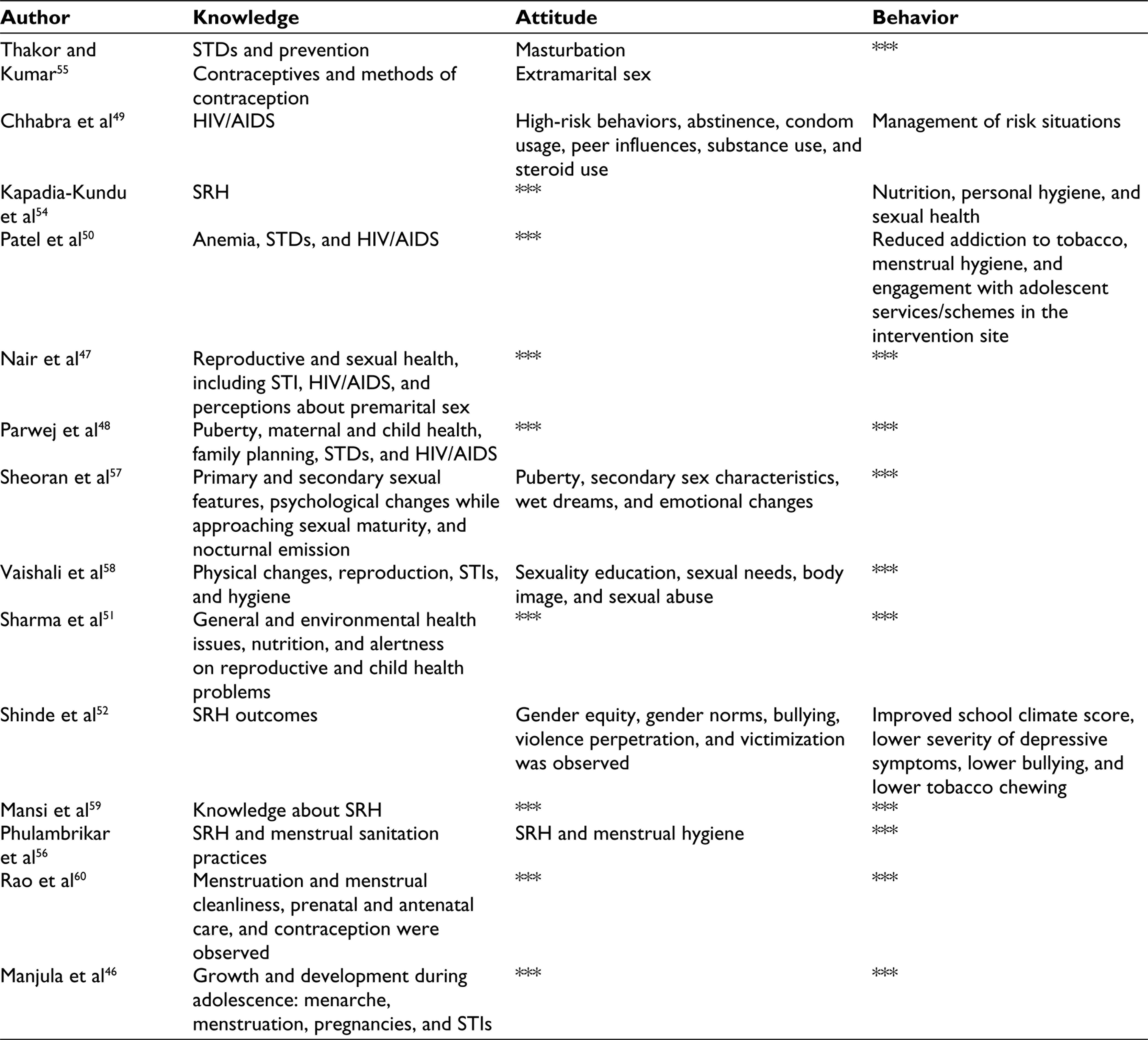
For the review, 14 studies were identified from various regions of India. SRH outcomes in the selected studies were consolidated for analysis (see Table 2). Among the 14 studies reviewed here, 4 were from Maharashtra and 2 were from Karnataka and Gujarat. There were single papers from Kerala, Uttar Pradesh, Chandigarh, Haryana, Himachal Pradesh, and Bihar. While 5 papers considered in this review were published before 2010, 9 were published between 2010 and 2020.
All the studies clearly stated the objectives—every intervention aimed to enhance the participants’ knowledge of SRH outcomes. 5 studies assessed changes in knowledge and attitude, such as growth and development, STIs, extramarital sex, pubertal changes among preadolescent boys, personal sexual needs, sociocultural correlations, gender equality/gender norms, bullying, violence victimization, and violence perpetration. 4 interventions focused on behavioral changes, including hygienic behaviors, menstrual hygiene practices, leadership skills, reduction of substance use (tobacco), communication with parents, utilization of services for adolescents, and well-being.
Summary of SRH Outcomes in the Selected Studies
Description of Intervention
Across the 14 studies, the implementation of interventions varied widely. All the
interventions reviewed here dealt with SRH interventions in the classroom
setting. This review considered the following aspects affecting intervention:
The content of the information involved in the
intervention. The means of delivery and human resource utilized for
intervention. The target population groups and the duration of the
intervention.
These variables are elucidated below.
First of all, the content of interventions made it hard to arrive at conclusions; often, the investigations demonstrate varying degrees of comprehensiveness. The interventions’ main emphasis was on development and growth, menstruation, menstrual hygiene, pregnancy, STDs, HIV/acquired immunodeficiency syndrome (AIDS), and birth control, or a mixture of all these. Rarely addressed areas include peer rejection, harassment, relationship issues, gender equality, abusive behavior, constitutional rights, 48 high-risk mitigation, 49 and youth services. 50 However, the scope of school-based interventions was widened to accommodate concepts such as nutritional features, physical well-being, vaccination, environmental safety, 51 and mental health issues. 52
Various intervention deliverance strategies were employed in isolation or combination, comprising lectures, counseling, exhibitions, brainstorming, stories, make-believe situations, group discussions, demonstrations, quiz programs, and adolescent health day celebration. 50 Human resources employed in the interventions comprised school teachers, peer educators, lay counselors, and health professionals such as psychiatrists, gynecologists, family physicians, and public health nurses. The reproductive health education programs among adolescents in Maharashtra and Chandigarh involved peer educators.48, 49 Peer educators and conventional education methods were employed in propagating information, but peer educators’ engagement was less time-consuming. 48 The multicomponent intervention conducted among adolescents employed a low-cost lay counselor and a school teacher. The intervention had fewer effects while being delivered by teachers; however, it had a notable favorable influence on the school environment and outcomes related to health while being carried out through lay counselors. 52 6 studies stated specialized training to the facilitators.48–50,52–54 The quantity and length of implementation of the school-based intervention varied broadly. It varied from a 2-h session 55 to a 2-year longitudinal intervention. 56
The majority of interventions were carried out in the age group of 13 to 18 years. The study of early adolescent (11–14 years) girls in Uttar Pradesh 54 and the preadolescent (12–14 years) boys from Haryana 57 showed a shift in the age group. The Gujarat study centers on adolescents aged 11 to 18 years. 50 7 studies report on interventions for both adolescent boys and girls. 6 papers deal with interventions exclusively delivered for adolescent girls, and one paper documented an intervention that included only adolescent boys. 57 6 studies were conducted among adolescents from rural areas, and 3 were delivered in urban settings.49, 55, 58 An intervention among adolescents in Kerala focused on adolescent boys and girls from urban and rural settings. 53 The intervention conducted in Mumbai targeted adolescents from slum areas. 59 The duration of interventions ranged from 2 h 55 to 2 years. 56
Outcomes
Knowledge
All the 14 intervention studies reported significant improvement in adolescents’ knowledge through school-based sexuality education intervention. Most studies reported a significant level of enhancement in knowledge concerning STIs, HIV/AIDS, bodily changes, anatomy, and physiology of the reproductive system during the adolescent period. 4 studies reported an enhanced understanding of contraception and pregnancy among adolescent boys and girls after the interventions.48, 51, 58, 60 The study conducted among preadolescent boys reported a significant increase in knowledge regarding pubertal changes, including knowledge regarding the idea of puberty, reproductive organs, development of secondary sexual characteristics, nocturnal emissions, and subsequent variations in one’s emotions. 57 School-based sexuality education programs also successfully improved general wellness, environmental health, and nutritional awareness.
Attitude
Six studies reported attitudinal change after school-based sexuality educational interventions. The study conducted among adolescents of Surat observed an encouraging attitudinal transformation toward extramarital sex and masturbation. 55 Pubertal preparedness program (PPP) intervention among preadolescent boys reported an increase in attitude score regarding the idea of puberty, development of secondary sexual features, nocturnal emissions, and psychological changes. 57 Intervention among adolescents in an urban setting in Maharashtra reported attitudinal changes toward personal sexual needs, sociocultural correlations, sexual abuse, media, and sexuality within friendship; however, the interventions did not induce any attitudinal shift on sexuality. 58 A multicomponent secondary school intervention conducted in Bihar reported attitudinal changes in gender equity, gender norms, bullying, violence, victimization, and perpetration. 52 Intervention on SRH for adolescent girls in rural areas observed positive attitudinal changes in menstrual practices and SRH. 56 “School-based teenage education program (STEP)” intervention among adolescents recorded changes in attitude toward abstinence, condom usage, peer influences, substance use, and steroid use. 49
Behavior
Out of all 14 studies, 4 reported behavior changes. 13 studies that reported behavioral changes related to diet, hygiene, and reproductive health were documented among early adolescent girls from Uttar Pradesh through school-based interventions. 54 The quasi-experimental research of adolescents has affected nicotine dependence, menstrual hygiene practices, and effective utilization of governmental schemes. 50
The multicomponent intervention in secondary schools conducted in Bihar reported changes in school climate, lowered the incidents of self-reported tobacco use, the severity of self-reported depressive symptoms, self-reported violence victimization, and self-reported bullying score. 52 The sexuality health education intervention among adolescent girls reported significant changes in menstruation practices, including the increased use of sanitary pads and decreased use of cloths. The subjects reported that they started to dry menstrual cloths in sunlight and increased the frequency of changing pads/cloths (during school time) and disposal of used pads. 56 In addition to information development, attitudinal change, and behavioral modification, the “STEP” intervention promotes positive attitudes about people infected with HIV/AIDS and raises the level of trust of adolescents in handling risky circumstances. 49
Discussion
This review’s prime objective was to comprehensively understand the impact of SRH interventions on adolescents in the school settings; the final search results yielded only 14 studies that met the criteria for inclusion. The results of interventions were observed to be positively influencing knowledge, attitude, and behavior related to SRH. Interventions based on school settings have a significant role in determining adolescents’ awareness, outlook, and conduct in reproductive health. 61
Among the 14 interventions, all were found to be effective in enhancing the knowledge of adolescents regarding SRH outcomes significantly in the areas of growth, bodily changes, STIs, STDs, contraception, HIV/AIDS, menstruation, hygiene, relationship, and additionally aided in the dissemination of information about general health, immunization, environmental health, 51 nutrition,50, 53, 54 and substance abuse.50, 52 The review demonstrates that school-based interventions were effective in inducing changes in the attitude of adolescents. 6 studies reported attitudinal changes toward extramarital sex, 55 pubertal changes during adolescence, 57 personal sexual needs, 58 gender equity, violence victimization, 52 and high-risk behaviors. 49 Sexuality education was also helpful in making effective behavioral changes among adolescents. 62 4 studies focused on behavioral outcomes such as menstrual hygiene practices, 56 the school climate, tobacco addiction,50, 52 and improved preventive health behaviors. 54
Few previous analogous reviews have made the same conclusions, especially regarding knowledge, attitude, and behavior-related domains. A review study from Nigeria included 7 studies. Among these, 4 studies documented significant improvement in knowledge, 3 reported attitudinal changes, and 3 noted changes in sexual health behavior. 63 The review on school-based sexual health intervention in Saharan Africa included 10 studies, among which, except for 2 studies, all the rest showed the effect of the intervention on knowledge or knowledge and attitude. 4 studies explored the effect of the intervention on actual sexual behavior. 64 A review of middle-income countries revealed that knowledge and attitude on sexuality improved after the interventions. 42
An extensive range of strategies adopted for interventions such as group activities, role-play, peer education, conventional education methods, etc, could augment the success of targeted interventions. The nature of human resources for delivering information was observed to vary, ranging from peer educators and lay counselors to schoolteachers and health care professionals. Hiring lay counselors (members of the local community) is a cost-effective strategy for delivering effective interventions.52, 65 Adolescents are often more comfortable discussing sexual health issues with health professionals than with their teachers. 66
These results show that the interventions were mainly focused on knowledge enhancement/generation and attitudinal change rather than behavior modification. Focusing on improving the level of trust, service-seeking attitudes, and a right-based approach among adolescents is crucial. Adolescents represent a heterogeneous population, and their needs vary widely because of prevailing sociodemographic inequalities.
A good number of interventions were conducted among mid-adolescence and later-adolescence (13–19 years), and fewer studies focused on early adolescents (10–13 years). Participants’ gender, like their age groups, was a source of concern, since many interventions were designed and focused on the sexual health education of girls, while boys were found to be ignored. Also, the results from interventions cannot be generalized to all adolescents. School-based intervention’s effectiveness depends on the content, delivery methods, coverage, and support from the school, teachers, parents, and the target population.67, 68 Evidence shows that education on human sexuality is a felt need for adolescents.69–71 The intervention must be comprehensive, age and culturally appropriate, and longitudinal.
Conclusion
School-based sexuality education has been delivered in India and across the globe through various approaches. The present study was based on SRH interventions for Indian adolescents in school settings. Interventions centered on knowledge, generation, attitudinal, and behavioral changes related to sexuality and reproduction were included in this review. The study found that interventions focused primarily on knowledge enhancement and less on behavioral changes. Sexuality education at schools should offer precise and comprehensive knowledge of sexuality while building the capacity for negotiating sexual behaviors. 72
The findings of this study demonstrate the necessity for standardization and prioritization of indicators for the evaluation of SRH programs. Methodological enhancements in terms of standardizing the concept of sexuality education, using concrete behavioral change interventions, and case-control are thus essential.73, 74 In developing nations like India, cultural and societal factors have a role in early childbearing. Early childbirth is usually associated with marriage. Adolescents may be pushed or coerced into marriage at an earlier age. 6 There are several factors, including social stigmas, shame, and communication gap, that impede communication between parents and teenagers. 75 Hence, program implementers should strive to improve communication between adolescents and their parents. Participatory sexual health education programs might be more effective in addressing cultural taboos, ensuring community ownership, and ensuring long-term viability and sustainability. The fact that there are just a few reviews on SRH in Indian schools reveals that, even today, SRH programs and interventions are confined to trials undertaken in a small number of schools in remote settings. Comprehensive reproductive health education programs should be implemented in every school setting to disseminate information on pregnancy prevention, STIs, sexual hygiene, the prevention of early marriages, and the promotion of better reproductive health among adolescents.
Further research on adolescents’ awareness, behaviors, and attitudes about sexuality and reproductive health is required. 76 Moreover, interventions should extend beyond mere knowledge advancement and assuredly aim to induce a substantial reduction in risk-taking behaviors among adolescents.
Supplementary Material
The supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.