
Abstract
Aim:
To assess the profile of patients availing the marital and psychosexual clinic (MPC) services through the telemode at a tertiary care center after the imposition of lockdown and compare the same with the profile of the patients attending the outpatient services, in-person MPC services during the prelockdown period.
Materials and Methods:
It was a retrospective study in which comparisons were made between patients availing the MPC services from March 24, 2020 to March 23, 2021 with the profile of patients during the period of March 24, 2019 to March 23, 2020 (ie, COVID period—lockdown).
Results:
A total of 112 patients availed the MPC services during the COVID study period compared to 307 patients in the pre-COVID period. However, when the proportion of MPC cases among the total walk-ins was compared, during the COVID period the proportion of MPC cases increased by almost 1.75 times. During the COVID time period, there was an increase in the patients who were significantly younger (P = .002), females (P = .003), more from urban locality (P = .035), and being referred by self or caregiver (P = .001). In terms of specific diagnosis, as compared to the pre-COVID timeframe, significantly higher numbers of patients were diagnosed with premature ejaculation (PME) and PME + erectile dysfunction while the services were being provided through the telemode.
Conclusion:
The present study suggests an increase in the proportion of patients seeking help for marital and sexual issues while the services are being provided by telemode.
Introduction
COVID-19 pandemic and the subsequent lockdown led to the closure of routine psychiatric outpatient services both in government and the private sector in India.1, 2 To provide continuity of mental health care, telepsychiatric services were started in almost all hospitals and health-care centres.3–5 Studies from various parts of the globe have reported an upsurge of mental health issues during the lockdown period.6, 7 Similarly, there had been concerns with regard to marital and psychosexual problems during the pandemic.8, 9 Studies have reported an increase in marital problems and domestic violence in females9, 10 and a rise in the prevalence of erectile dysfunction (ED) in males. 11 Additionally, there have been concerns with regard to the impact of COVID-19/SARS-2-CoV infection on male sexual functioning and its potential for sexual transmission.12, 13 Therefore, it is pertinent to understand the marital and psychosexual problems during the lockdown period. Further, there is a need to understand the impact of the pandemic on the utilization of psychosexual clinic services, which has not been studied.
The Department of Psychiatry, PGIMER, Chandigarh had been running the Marital and Psychosexual clinic (MPC) since June 1987, which caters to the marital and sexual issues of the patients. Patients with sexual problems and marital discord are registered in the MPC clinic at the walk-in level and subsequently undergo detailed evaluation and treatment. During the lockdown period, the routine outpatient services were discontinued from March 21, 2020 to October 31, 2020 and later again discontinued from April 11, 2021 to July 4, 2021. In view of the discontinuation of the routine outpatient services, telepsychiatry services were started in April 2020. During the pandemic, the telepsychiatry services of the Department of Psychiatry, PGIMER, Chandigarh were the only source of providing outpatient teleconsultations which were modified in line with the existing telepsychiatric guidelines of India. However, when the routine outpatient services started working, the majority of the new patients were seen through the telepsychiatry services as the routine outpatient services were restricted to seeing a small number of patients. As the discussion of sexual issues requires lot of confidentiality, it is important to understand the comfort level of the patients and their partners to discuss these issues through teleconsultations. The teleconsultations for marital and sexual issues can work in both the directions. First, patients may be hesitant to discuss the issues, because of the apprehension that the information may be available to others, due to lack of security in the various platforms used for providing the medical care. On the other hand, patients and their spouse may feel more comfortable discussing their sexual and marital issues by sitting at their home, without the hassle of traveling and fear of being seen by others in the psychiatry outpatient services. This may reduce the stigma associated with seeking medical help. Hence, it is important to understand the impact of change in the mode of providing services to patients with marital and sexual problems. In this background, the present study aimed to assess the profile of patients availing the MPC services through the telemode at a tertiary care center after the imposition of lockdown and compare the same with the profile of the patients attending the outpatient services, in-person MPC services during the prelockdown period.
Materials and Methods
The Department of Psychiatry, Postgraduate Institute of Medical Education and Research, Chandigarh maintains all the records of the patients registered in the outpatient department (OPD). For this study, the data pertaining to the outpatient records of patients registered in the MPC were retrieved.
The patients registered in the MPC clinic are first evaluated by a Senior Resident and were later evaluated in detail by a Junior Resident and discussed with a consultant. During the lockdown period, through telemode also, the same pattern was followed, that is, the patients were initially evaluated by a Senior Resident by voice/video calls and started on the treatment. After the initial evaluation, the patients were given a date for the detailed evaluation. Then the patients were evaluated in detail by a Junior Resident and discussed with the consultant. The evaluation by the Junior Resident was done by voice/video calls. However, the detailed evaluation by the consultants was done by the video calls, which could be recorded with the consent of the patients. Subsequent follow-ups are done by the Residents and the Consultants by voice/video calls.
All psychiatric diagnoses are made per the International Classification of Diseases-10 (ICD-10) 14 criteria.
For the purpose of this study, the records of all patients availing the MPC services from March 24, 2020 to March 23, 2021 were retrieved. Comparisons were made with the patient profile in the pre-COVID period, that is, from March 24, 2019 to March 23, 2020 (ie, COVID period—lockdown).
The study was approved by the Institute Ethics Committee. The data was anonymized prior to the analysis.
The data was analyzed using SPSS software, version 20.0. Descriptive statistics were applied.
Comparison of categorical variables was done by using Chi-square test or Fischer’s exact test. For continuous variables, mean and standard deviation were calculated and comparisons were made by using the Student t-test or Mann-Whitney test. All P values were two-sided, and P values of <.05 were considered statistically significant.
Results
When we compared the data of same time frame, that is, March 24, 2019 to March 23, 2020 with the COVID pandemic and subsequent lockdown period/telemode consultations (March 24, 2020-March 23, 2021), the number of MPC cases in the walk-in drastically reduced from 307 to 112. However, if one looks at the proportion of the MPC cases vis-a-vis, the total number of walk-in (March 24, 2019-March 23, 2020: 307 out of 15,420 [total number of OPD registrations] = 1.99%; March 24, 2020 to March 23, 2021: 112 out of the 3,203 [total number of teleconsultations] = 3.49%), the proportion of patients with MPC problems who sought help when the services were provided by the telemode increased by almost 1.75 times.
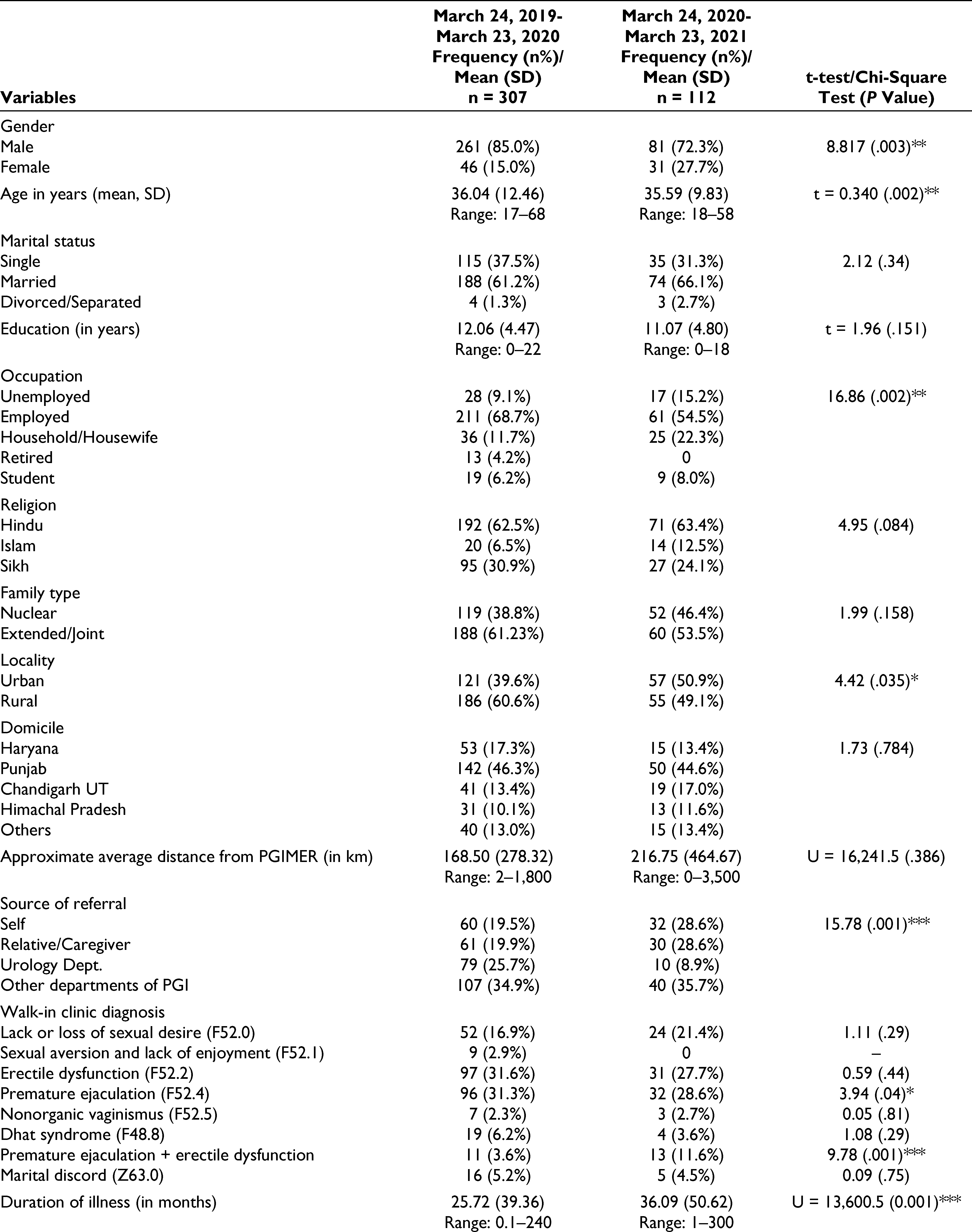
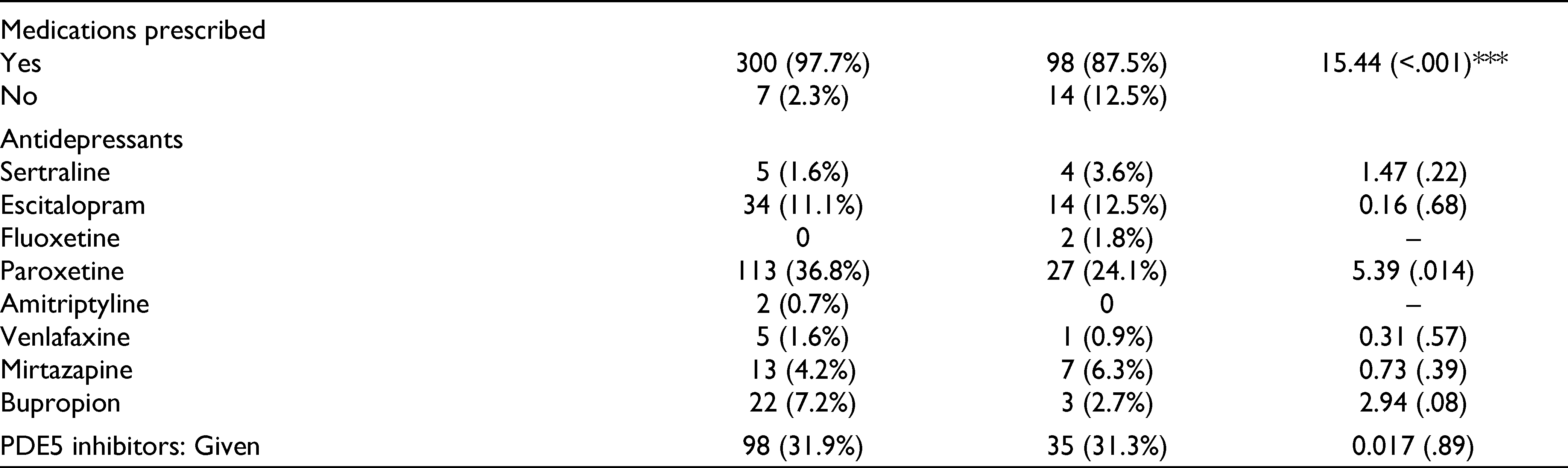
The details of demographic profile and clinical diagnosis of the patients registered with the MPC services that were provided care through telemode are given in Table 1. When the patient profile was compared with the profile of patients who registered in 2019 to 2020, it is evident that there was an increase in the patients who were significantly younger, females, more from urban locality, and being referred by self or caregiver. Further, more patients from longer distance from the institute (in km) were able to seek help from the MPC clinic when the services were provided through the telemode. In terms of specific diagnosis, as compared to 2019 timeframe, significantly higher numbers of patients were diagnosed with premature ejaculation (PME) and PME + ED while the services were being provided through the telemode. Those registered through telemode had longer duration of illness (in months) and more number of patients were not prescribed medications. The profiles of antidepressants/SSRIs and PDE5 inhibitors being prescribed in both the time frame were almost similar with no significant differences.
Demographic and Clinical Diagnosis of the Registered Patients in MPC Services During the COVID Pandemic.
In terms of recording of sessions, majority (89%) of the patients provided consent for the sessions to be recorded. In few cases of marital discord, although the partners had temporarily separated, they were prepared to join for the conjoint sessions through the tele-consultation mode from different locations. In some of the therapy sessions, it was also possible to make a partner join first and the second partner later on, so that they could be heard separately too.
Discussion
COVID-19 pandemic has emerged as a major crisis for all strata of public. The closure of regular outpatient services has left the patients in lurch. As evident from studies on the upsurge of marital and psychosexual problems during the pandemic,8, 15–17 it is essential to understand the profile of the patients consulting the MPC services during the pandemic.
As no previous studies have compared the functioning of the MPC services during the ongoing pandemic with the similar timeframe prior to the pandemic, it is not possible to compare the findings of the present study with the existing literature. Hence, we would like to discuss our findings in the context of data which has emerged during the ongoing pandemic.
The present study suggests that although there was reduction in the absolute number of patients with MPC issues presenting during the ongoing pandemic, there was proportionate increase in the number of patients presenting with the MPC issues, when compared to all the patients attending the psychiatric services during the ongoing pandemic when telemode provided the services. The significant reduction in the MPC cases registrations in the COVID study period is similar to the reduction in all types of psychiatric consultations (outpatients, inpatients, emergency visits) during the lockdown and COVID period. 18 However, when analyzed more closely, we found that the proportion of MPC cases out of the total walk-in registrations was 1.75 times greater in the COVID study period than the pre-COVID period. This finding can be interpreted in different ways. First, this could just be a chance finding. Second, this finding suggests an increase in the marital and sexual issues among the general population as has been reported by some of the surveys8, 15, 17 that led to an increase in the patients seeking help for these issues. Third, this increment in number of cases could be a result of impact of the pandemic, as has been suggested by the findings of various online surveys, which suggest there was increase in psychological distress and the pandemic also had an impact on the sexual functioning. 15 Fourth, this rise in the proportion of patients with MPC services could be a reflection of availability of time, as during the major part of the pandemic there was less work pressure or people were working from home. Fifth, availability of time, and the convenience to seek help by sitting at home could have led to more help seeking. Finally, this hike in proportion of patients with MPC issues could be a reflection of a higher level of acceptance of teleconsultation in this group of patients. At the beginning of providing the services through the telemode, we anticipated that teleconsultation for marital and psychosexual problems could be difficult as many patients might not be comfortable in discussing about their sexual problems online. However, in contrast to our anticipation, we found that patients were comfortable in discussing their psychosexual issues through the telemode.
Another important finding from the study is an increase in the proportion of females and housewives/homemakers seeking help from MPC issues. This should not be interpreted as seeking help for sexual issues only, but could be a reflection of seeking help for marital issues. The increase in females among the help seekers during the pandemic could also reflect increase in distress, ease of seeking help, and reduced level of perceived stigma while seeking help by telemode could be some of the reasons for the same. The increase in proportion of persons from urban locality and self-referral possibly reflects the awareness about the services and possibly better internet connectivity in the urban areas. The reduction in proportion of referrals from the urology services could be an outcome of poor consultation liaison between the 2 departments while providing services through the telemode or could be due to the difficulty faced by patients in registering with the services. The study findings further suggest that there was greater number of younger subjects who availed the MPC tele-services. This possibly could be a reflection of more familiarity of the younger people with the current technology being used for seeking teleconsultations. The increase in patients from longer distance from the institute (in km) seeking help through the telemode reflects the advantage of the services being available at the remote location at the click of a button. Overall, it can be said that the demographic profile of patients seeking help through the telemode suggests that providing MPC services through the telemode helps in reaching the unreached and there is a need to systematically understand the utility of such services in future and scale up the same.
In terms of specific diagnosis, as compared to 2019 prepandemic time frame, significantly higher numbers of patients were diagnosed with PME and PME + ED in the 2020-2021 telemode duration. Those registered through telemode had a longer duration of illness (in months) and more patients were not prescribed medications. This profile again suggests that teleconsultations provide better opportunity for them to seek help, who for some reason have not been able to reach to the clinic. The longer duration of illness could also be a reflection of lack of availability of services or awareness about the availability of the services. Further, lower prescription rate could be a reflection of either lack of need for the same or a reflection of need for further ascertainment of the diagnosis before prescribing the medications. This possibly suggests limitation of the teleconsultations, which do not provide an opportunity for detailed physical examination and investigations if required.
Our study has certain limitations. We did not assess the patient and their partners/family members’ experience of seeking help through the telemode. Further, we did not assess the satisfaction of the patients, exact treatment outcome, and number of follow-ups while providing services by in-person method or by telemode. Additionally, telemode facilities were accessible to only those who had access to teleconsultation devices like smart phones/laptop, and so on and this may not be reflective of the general population.
To conclude, the present study suggests that there is increase in the proportion of patients seeking help for marital and sexual issues during the ongoing pandemic. In terms of demographic profile, there is an increase in the proportion of younger patients, females, from urban locality and from longer distance. In terms of clinical profile, those seeking help during the ongoing pandemic have longer duration of illness, more often have both PME and ED and are not prescribed medications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.