
Abstract
E-health and telehealth are rapidly evolving areas of intervention that may show high potential for use with LGBTQIA+ individuals. Research on the therapeutic utility of these with respect to mental health is limited, particularly in India. SAAHAS (Sexuality, Acceptance, Awareness, Health, and Support) is a queer-affirmative, cognitive behavior therapy-based group therapy model of intervention for LGBTQIA+ individuals. We describe here our facilitator experience with expanding the offline group therapy model to online platforms using Google Meet, with an analysis of attendance and modalities of engagement and a description of our therapy notes and themes of discussion. We describe facilitator experience of continued therapeutic support through WhatsApp by analyzing the chats and thematic coding of the same. We also describe here our attempt at using social media for community mental health outreach through dissemination of mental health messages on Instagram and Facebook; data was analyzed using engagement metrics. Observations of the utility and limitations of these video conferencing and social media platforms and suggestions for effective use are provided.
Introduction
SAAHAS (Sexuality, Acceptance, Awareness, Health and Support) is a therapy group for LGBTQIA+ individuals in Mumbai, that is run by two queer mental health professionals. It works with a queer affirmative cognitive behavior therapy (CBT)-based framework, and has been demonstrated to show preliminary promise in bringing about positive mental health outcomes for participants. 1 We have outlined here some ways in which we used video conferencing and social media platforms to provide therapeutic continuity. We used Google Meet for our regular sessions and found some challenges as well as some benefits in the adaptation, which are described here. We used WhatsApp for therapeutic discussions between sessions and describe here how peer and facilitator support were provided using this platform. Instagram and Facebook were used as platforms to disseminate some key mental health information to the LGBTQIA+ community. We describe our experiences and outline some recommendations for mental health professionals who wish to work with this group on how to use social media platforms for actual therapy, between session therapeutic contact, and community mental health messaging.
Research on Social Media Based in the Health Field
Past research has suggested that the Internet and social media have significant value for LGBTQIA+ individuals—they provide safe and accessible spaces to explore and express their gender and sexual identities, help them to access affirming psychosocial support and establish connections, and are platforms for them to find resources and acquire information about gender, sexuality, and mental health.2-4
Social media, e-health (web-based), and telehealth (phone-based) platforms as modalities for interventions are a relatively new area of study in the field of health care. Some of their benefits include their accessibility across geographical barriers, ease of use and convenience, reduction of patient wait-time and costs incurred; LGBTQIA+ individuals may also perceive these to be safer than offline public health platforms because of the discrimination and stigma that they often face while accessing health care in offline spaces.2,5-7 Online spaces may also be less transitory than online spaces. 8
There is evidence for chat-based platforms like WhatsApp and WeChat being used effectively for different health care purposes, for example, online social support to promote smoking cessation9-10 and for survivors of domestic violence 11 ; these platforms have been found to be useful as aids to clinical decision-making and patient care, as well as patient learning, and have generally been found to rate high on user satisfaction.12,13
Social media has many potential applications for enhancing community public health outreach, but there is much lesser research documenting the actual usage of the same. 14 Some advantages of the social media include the ability to target new and diverse audiences, the ability to receive feedback immediately, increase engagement, and also build communities. 13 Among specific social media platforms, Instagram and Facebook have been used effectively for dissemination of public health messages and social support.4,12,15
Despite the preference for online health support espoused by LGBTQIA+ individuals, there is relatively lesser research about the efficacy of online health care interventions with LGBTQIA+ individuals. Some guidelines have been laid out for the same. 16 We found some programs utilizing e-modalities such as QueerViBE which uses online video tutorials to build stigma competence, 17 and Rainbow SPARX which provides computerized CBT. 18
In India, a study examined the use of Internet dating platforms such as Planet Romeo and Grindr and Facebook groups such as Pink Kolkata Party in community building, identity formation, and negotiating intimacies and friendships. 8 Another study explored the online platforms used by SAATHI (online library, mobile counselling, e-conferencing, and forums, and a Facebook group), with respect to HIV prevention and destigmatization. 19 An ethnographic study examined the online and offline community created by GayBombay through their website. 20 Some studies examined the use of blogging in queer community building,21,22 and social media advertising in promotion of awareness about LGBTQIA+ issues. 23 We did not find research focusing on online video and chat platforms (particularly Google Meet and WhatsApp) as modes of therapeutic intervention for mental health, or any social media (Instagram, Facebook in particular) for community mental health promotion of LGBTQIA+ individuals in India.
Currently, given the background of the Covid-19 pandemic, online therapeutic interventions are particularly important. LGBTQIA+ youth may have found the pandemic stressful due to confinement to unfavourable work environments and isolation from their usual identity-affirming social connections, and may be likely to seek out resources and community online at this time. 24 This article aims to bridge this gap in research, documenting experiences of providing online interventions as a part of expansion of the SAAHAS group as well as using social media platforms for promotion of community mental health.
Introduction to Year 2 at SAAHAS
We started SAAHAS in 2018 as an offline therapy group meant for LGBTQIA+ individuals. The first year’s experiences, including details about group formation and group building processes, safety measures, and participant recruitment and socialization protocol, have been described elsewhere. 1 For the purpose of safety, potential participants who filled in the recruitment form met the facilitators for a face-to-face interview, where mutual expectations, safety measures, group rules, confidentiality, and the limits to the same, were discussed, and only following this, were they allowed to attend group sessions. We took informed signed consent for offline and online participation in the group, and for the use of anonymous data for research purposes and publication.
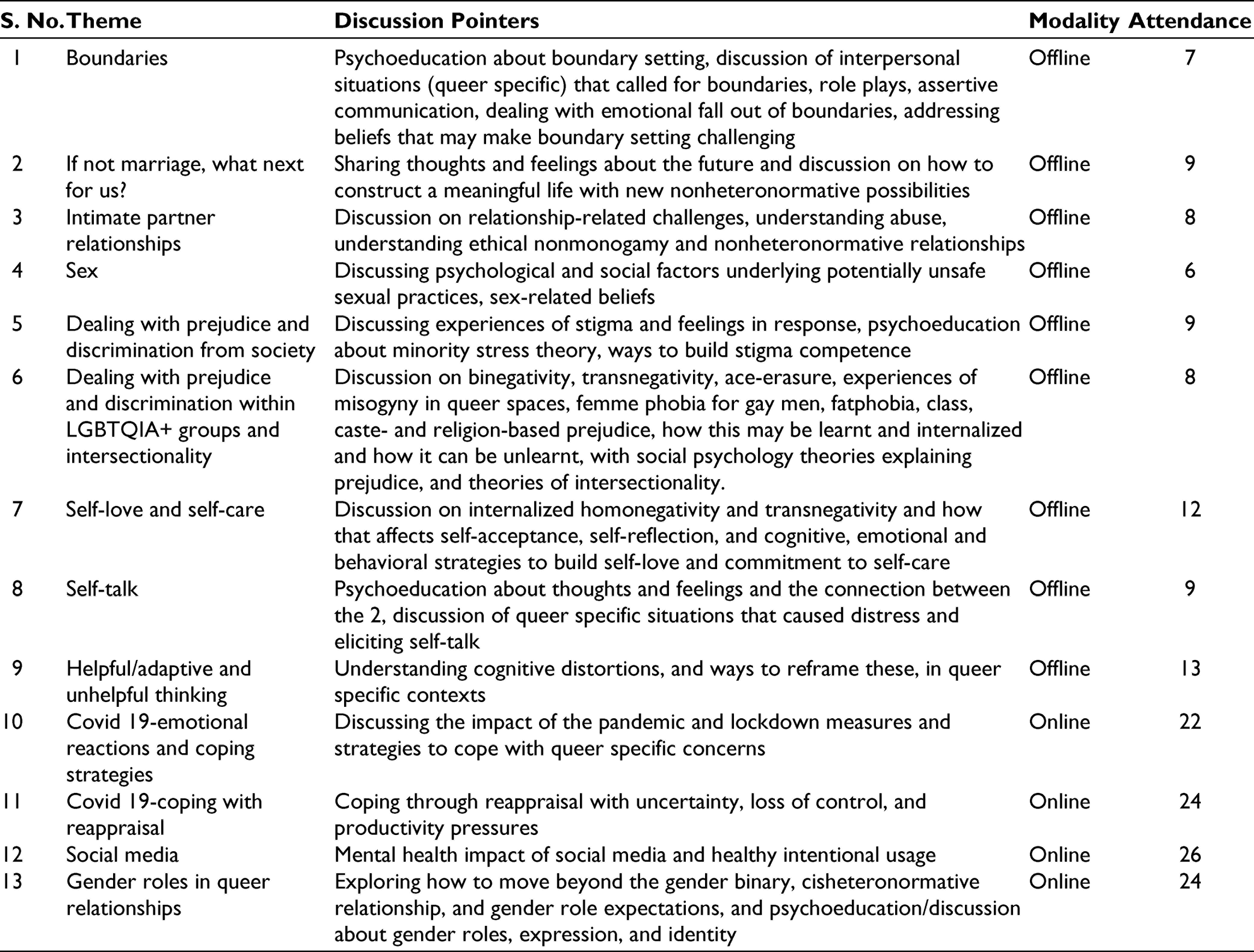
We had a total of 52 participants over 2 years who attended at least 1 session, and we had 25 new participants in the second year. A total of 67.31% of our participants were cis men who were gay or bisexual, while 13.46% were cis women who were lesbians, 15% were transgender and nonbinary, and 5.77% were questioning. In the first year at SAAHAS, we had observed that 78% of the participants were cis gay or bisexual men, and sexual minority women and trans individuals showed lower participation, possibly due to the “politics of access.” 1 To remedy this, we had 1 session geared specifically toward marginalized communities within the LGBTQIA+ community, communicated specific content geared toward transgender, and bisexual individuals on our social media, and we specifically disseminated information about the group on LBT only platforms; participation of transgender and non-binary individuals, and of lesbian and questioning cis-women, was found to have increased by 33% following these attempts. Participant ages ranged from 19 to 48. We tried to make the group intersectional by explicitly discussing intersectionality in our social media posts and all material used for promotion of the group, and we also addressed intersectionality as a topic of discussion in session 6. Table 1 describes topics of the 13 monthly sessions conducted, summary of the discussion, meet modality, and number of participants. The number of participants ranged from 6 to 26 per session and average number of participants per session was 9.
Record of Sessions for Year 2 of SAAHAS
Regular check-ins with participants about their experiences of online and offline platforms, and meticulous group records and observation notes, formed a part of quality control.
Transitioning to Group Therapy Sessions via Videoconferencing
The last 4 sessions were conducted online on Google Meet during the Covid-19 pandemic. The links for the same were shared on a closed WhatsApp group. While participants reported that they were keen to attend the group meetings, some of them expressed privacy-related concerns as they were confined at home with their parents who they had not disclosed their gender identity and sexual orientation to. Hence, we decided to allow participants to join in either on video, audio, or chat depending on their preference. Out of the 26 participants who attended at least 1 of the sessions, 38.46% joined on video, 26.92% on audio, and 34.61% on chat. Despite initial reservations that this would make the conversation chaotic, we were able to have structured meetings, with disciplined participation, and each participant spoke at least once.
One of the major benefits of online meet was increased participation. We noticed that average participation for the 4 online sessions was higher than for offline sessions at 24 (2.7 times more than the offline sessions), with attendance ranging from 22 to 26. A total of 23% of the participants were not residents of Mumbai and were either new to SAAHAS or were old participants who had migrated to other cities. The convenience of online meet was reported by them as one of the major reasons why participants could attend. In addition, during the time of Covid-19, with higher isolation experienced by individuals and being in an invalidating home environment, these group meets provided an opportunity for discussion with likeminded individuals and affirmation of their identities and their experiences. The sense of solidarity with respect to getting through the pandemic together also came across in the sessions.
As facilitators, we did face some challenges—one of them being that the cohesion of the group may have been compromised by the absence of video for many of the participants. We believed this to be especially true with respect to new participants who hadn’t already formed bonds with the other members. Also, privacy restrictions may have affected the freedom with which people could share concerns, and the quality and stability of the Internet connection across participants fluctuated, leading to some disturbances in the session. Personally, managing the session flow with different points of input—video, audio, and chat, and ensuring that there were no parallel derailing conversations and the session stayed on track—was a bit of a challenge. This was managed by setting clear agendas and having more structured sessions led by facilitators.
Using WhatsApp for Between Session Therapeutic Contact
When we started SAAHAS, we also created a WhatsApp group for all the participants, which was intended purely as a convenient way to coordinate group meetings and disseminate messages for the group. However, over the past year (even before the pandemic), we decided to utilize the group as a means of facilitating between session therapeutic contact.
Our experiences suggest that WhatsApp groups can be a good way of maintaining between session therapeutic contact. Some of the suggestions that emerged from our experience are as follows:
WhatsApp communication was meant as an addition rather than a substitute to regular group sessions, and this was clarified with participants. We took consent of all participants before adding them to the group. Also, we ensured that we only added participants to a WhatsApp group after they attended the first actual group therapy session and became acquainted with other group members. Participants were not allowed to add other members to the group. It is crucial to have clearly defined and explicitly stated guidelines with respect to the kind of engagement expected and encouraged on the WhatsApp group. Some of our rules included—maintaining confidentiality and not outing individuals without their consent, stating and respecting pronouns, only affirmative statements and no name calling, restricting sharing on the group to content related to LGBTQIA+ mental health, with no irrelevant forwards or messages, and checking in with the facilitators prior to sharing content if they weren’t sure of the relevance. We also had a discussion on etiquette to maintain if group participants wished to talk to specific participants one on one, and rules for the same included no solicitation or cruising. As facilitators, we performed 2 roles. We let the conversation and discussions flow spontaneously and intervened when we felt our inputs were necessary or would be fruitful, ensuring that the discussion stayed affirmative, or in the case of a dispute. At the same time, we also took a more active stance on occasions to lead discussions on issues.
For the purpose of this article, we conducted thematic analysis of our WhatsApp chat conversations. Chats were divided into (a) facilitator-run and scheduled chat sessions and (b) spontaneous group discussions. We analyzed the chat messages and divided these into (a) facilitator inputs and (b) peer support inputs. We further analyzed the nature of these inputs and applied code labels for each separate theme that emerged, where each theme symbolized a specific kind of therapeutic input.
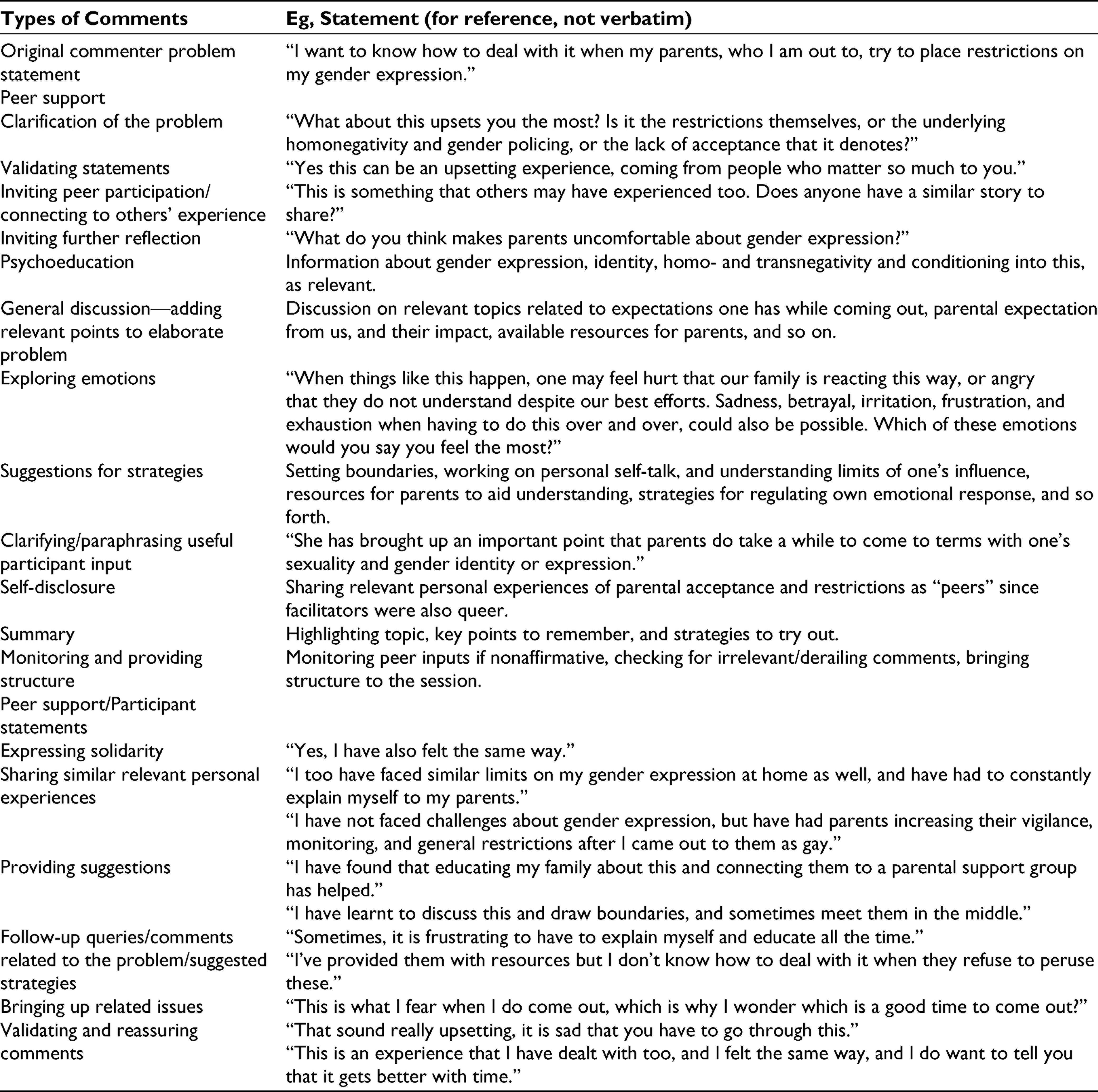
The facilitator-organized chat discussion was held with the participants at a pre-decided time. The chosen topic was based on request by a participant dealing with parental restrictions on expression after coming out to them. Table 2 describes the kinds of inputs provided by the facilitator as well as the participants in the discussion. Around 8 participants were active in the discussion, while the others attended passively.
Facilitator and Peer Inputs for Facilitator-Driven WhatsApp Discussion
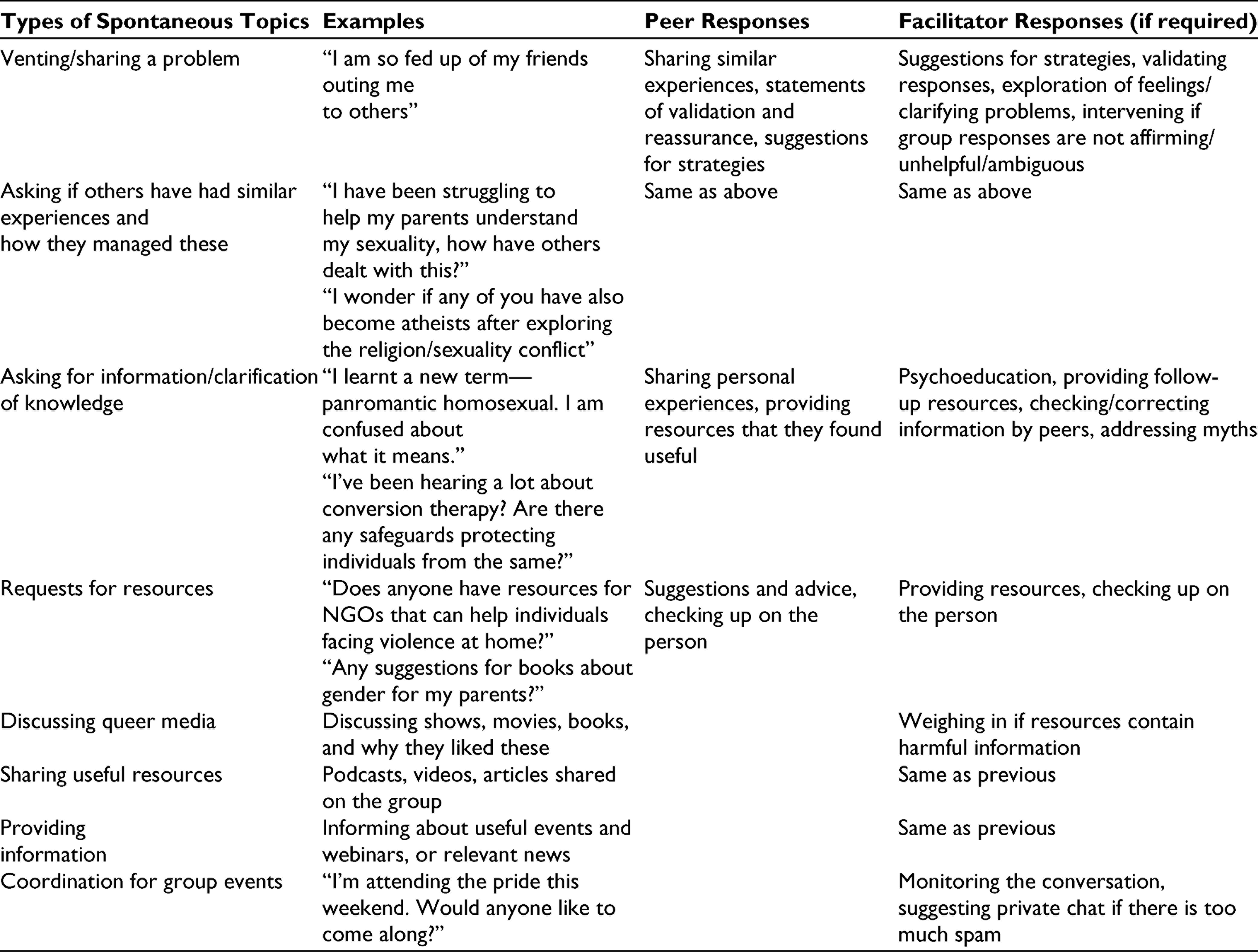
Following this discussion, which was well received, there were also spontaneous other discussions prompted by group members. Table 3 describes the usage of the chat group by the participants, kinds of peer support offered, and kinds of facilitator inputs provided.
Peer Inputs and Facilitator Responses for Spontaneous WhatsApp Discussions
We found that WhatsApp as a platform lent itself to more peer support, and helped to decenter the therapists. It helped to strengthen the SAAHAS group therapy “community,” with contact and support in-between monthly sessions, thereby strengthening social support networks. Besides convenience and the possibility of obtaining instant support rather than having to wait for the next session, further advantages of WhatsApp may be the catharsis from writing issues out on text, and the availability of the conversation for review later 5 ; this may ensure that individuals can remember and refer to the discussion whenever they need to, and even those participants who are passive or unavailable when the conversation is happening can benefit from it later.
While WhatsApp chats can be a platform for sustaining therapeutic discussion, we do believe that enforcing the rules mentioned above is crucial. It may be a challenge for the facilitator to regulate the discussion and ensure a healthy “signal-to-noise” ratio to ensure accurate learning and fewer messages that are barriers to learning or are irrelevant. While we found that participants typically provided helpful comments mentioned above, we were mindful of comments by participants that could potentially be unhelpful, as below:
Misgendering/using incorrect pronouns. Stigmatizing and pejorative terms—terms suggesting transnegativity, homonegativity, stigma about mental health, classist, communal, casteist, sexist, or ableist language. Judgmental and blaming comments. Advice that was potentially harmful. Information that was incorrect, unscientific, or unverified. Attempts to take over the conversation (rather than giving others room to express their opinions). Derailing/irrelevant comments that could disrupt rather than aid the discussion. Spam—random comments or posts unrelated to LGBTQIA+ issues, mental health, or the topic of discussion.
One of the risks of using WhatsApp is that of privacy—one cannot guarantee that group members do not “out” people (share that they are queer with others without their consent), or share screenshots of conversations. This has to be outlined while taking informed consent, and forming the WhatsApp group after an initial face-to-face group session may build trust between members.
Use of Instagram and Facebook for Community Mental Health
We utilized Instagram and Facebook for community mental health work. Research on the effectiveness of varied social media platforms and the use of metrics designed specifically for the same is an emerging phenomenon in market research, but we attempted to use the same metrics to obtain insights into the impact of our social media outreach communications as a pilot. We focused on reach and engagement metrics. The reach of a post describes the potential unique viewers of a post. Organic reach refers to reach of a post as it is and paid reach is reach after posts are sponsored. Engagement on a post or account describes the measurable interaction with the post or posts on an account, that is, number of likes, comments, shares, and saves of posts. Engagement rates can be calculated in many ways; the formulae used by us here were:
Engagement rate by reach = total of all engagements/reach × 100 Average engagement rate = total engagement rate/total number of posts
Engagement rate by reach demonstrates how many people who saw a specific post or certain group of posts found it/these valuable, which may indicate the utility of the content.
With respect to content, we put up introductory posts, podcasts, and news articles about SAAHAS to recruit participants, posts summarizing what we discussed during each session, posts describing research findings of our related papers in simple terms, along with general articles and posts about LGBTQIA+ mental health, on topics such as mental health indicators, how to choose therapists, do’s and don’ts for allies, mental health concerns of transgender individuals and bisexual individuals, and suicide prevention strategies.
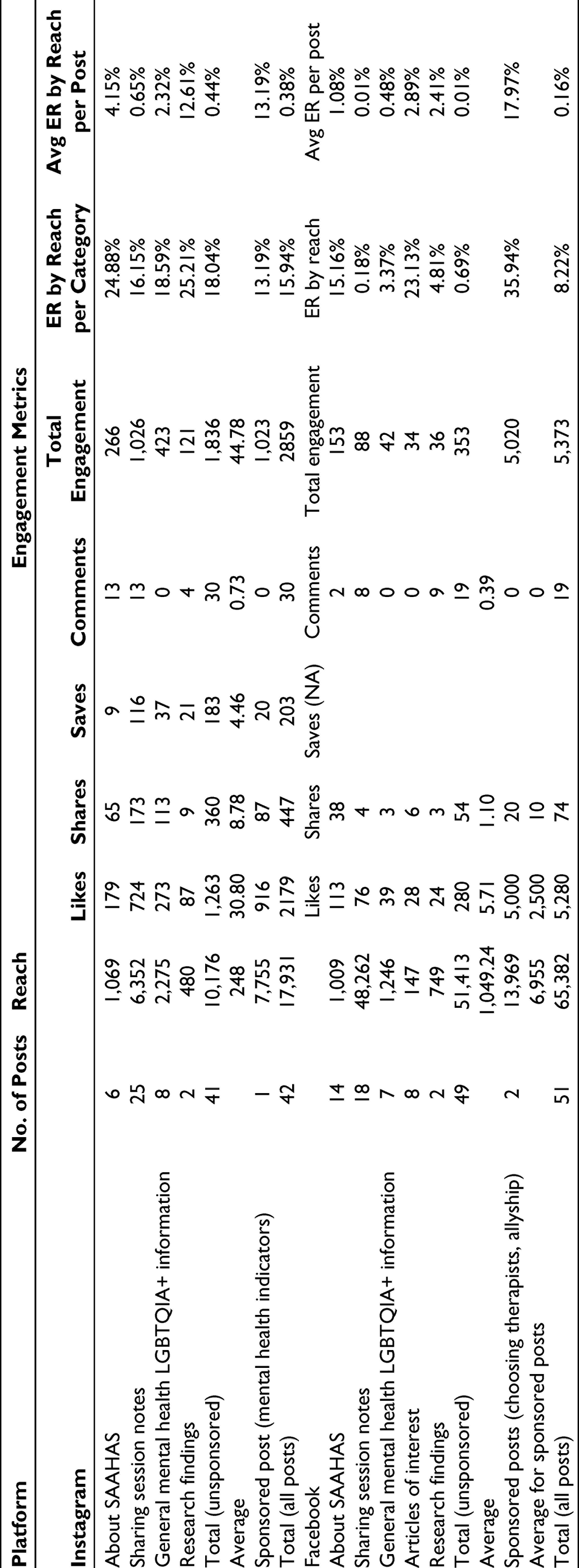
As of the date when this article was written, we had 273 followers on the Instagram page and 553 followers on the Facebook page. Table 4 describes post content categories, reach, and engagement metrics on both social media platforms. The reach metrics suggest that through our accounts, we were able to reach out to more than 10,000 individuals via Instagram and more than 50,000 individuals via Facebook, with an average of around 250 and 1,000, respectively, per post on the two platforms. The overall engagement rates by reach suggest that 15.94% of individuals on Instagram and 8.22% of individuals on Facebook who saw at least one of the posts on the accounts, engaged with the content and therefore may have found it useful. An average post was engaged with by 0.38% of the individuals who saw it on Instagram and 0.16% of the individuals who saw it on Facebook. Posts about allyship, choosing a therapist, our research summaries, as well as posts summarizing our sessions on abuse within queer relationships and planning for a future without marriage, showed the most engagement across platforms. While we were able to reach out to more individuals via Facebook, the engagement rates for posts were higher on Instagram than on Facebook.
Instagram and Facebook Posts—Content, Reach, and Engagement Metrics
As a trial, we self-funded the sponsorship of 3 posts, and found that the paid reach was exponentially higher than the organic reach. Thus, to scale up the community mental health outreach, sponsoring posts may be a good strategy, but this may be time limited, and to keep the engagement high, this would need to be accompanied by regular active involvement via stories, polls, more regular posts, careful choosing of hashtags, using carefully curated content, and so on; more research on what helps to increase engagement is needed. Organizations would need to allocate manpower and finances for the same if they wish to use social media for community outreach.
Conclusion
Our experience, although brief and limited, outlines the utility of using video conferencing and social media platforms for mental health of LGBTQIA+ individuals. With respect to intervention, a combination of audio, video, and/or chat may provide flexibility for participants when transitioning to online rather than offline group therapy meets. WhatsApp may be a useful mode of continuity of therapeutic intervention; it may also help to decenter the therapist and harness peer support. With respect to community mental health, we describe how Instagram and Facebook can be effectively used and how engagement metrics may be a relatively novel index to study their effectiveness. We thus aimed to continue offering some support to our usual participants as well as to LGBTQIA+ community members at large by expanding the reach of SAAHAS using online platforms, and shared our experiences of the challenges faced.
Given the increasing globalization, reducing digital divide and increasing use of the Internet, as well as the unique benefits of social media for LGBTQIA+ individuals and for mental health messaging in particular, more rigorous research on these modalities is the need of the hour.
Footnotes
Acknowledgements
The authors would like to thank the SAAHAS members for being a part of our very own queer community, and for allowing us to use their experiences in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.