
Abstract
Background:
Infertility is one of the major causes of mental health issues among couples. Interestingly, a large percentage of this infertility cannot be always explained in terms of a medical diagnosis. Psychological distress has long been suspected as having an important impact on infertility. However, the exact nature of association between psychological factors and infertility has been a subject matter of scientific debate. For modern urban women, there is an additional obligation of balancing work and home responsibilities; this dual role inevitably leads to stress. In this context, an important yet less-explored area of infertility is the role of work-related stress on female infertility.
Aims:
This study tries to investigate the mediating role of certain psychosocial constructs viz (a) Self-efficacy related to work-family conflict—measured in terms of “work-family conflict self-efficacy scale” by Cinamon (2003), (b) perceived occupational stress—measured in terms of “work-to-family conflict scale” by Netemeyer et al (1996), (c) decision-making in family—measured in terms of “decision-making scale” by Blood and Wolfe, (d) perceived infertility stress—measured in terms of “fertility problem inventory” by Newton et al (1999) in 25 urban working women of the age range 28 to 40 years who have been experiencing medically unexplained infertility for at least 1 year; the severity of infertility being measured in terms of duration of involuntary childlessness.
Results:
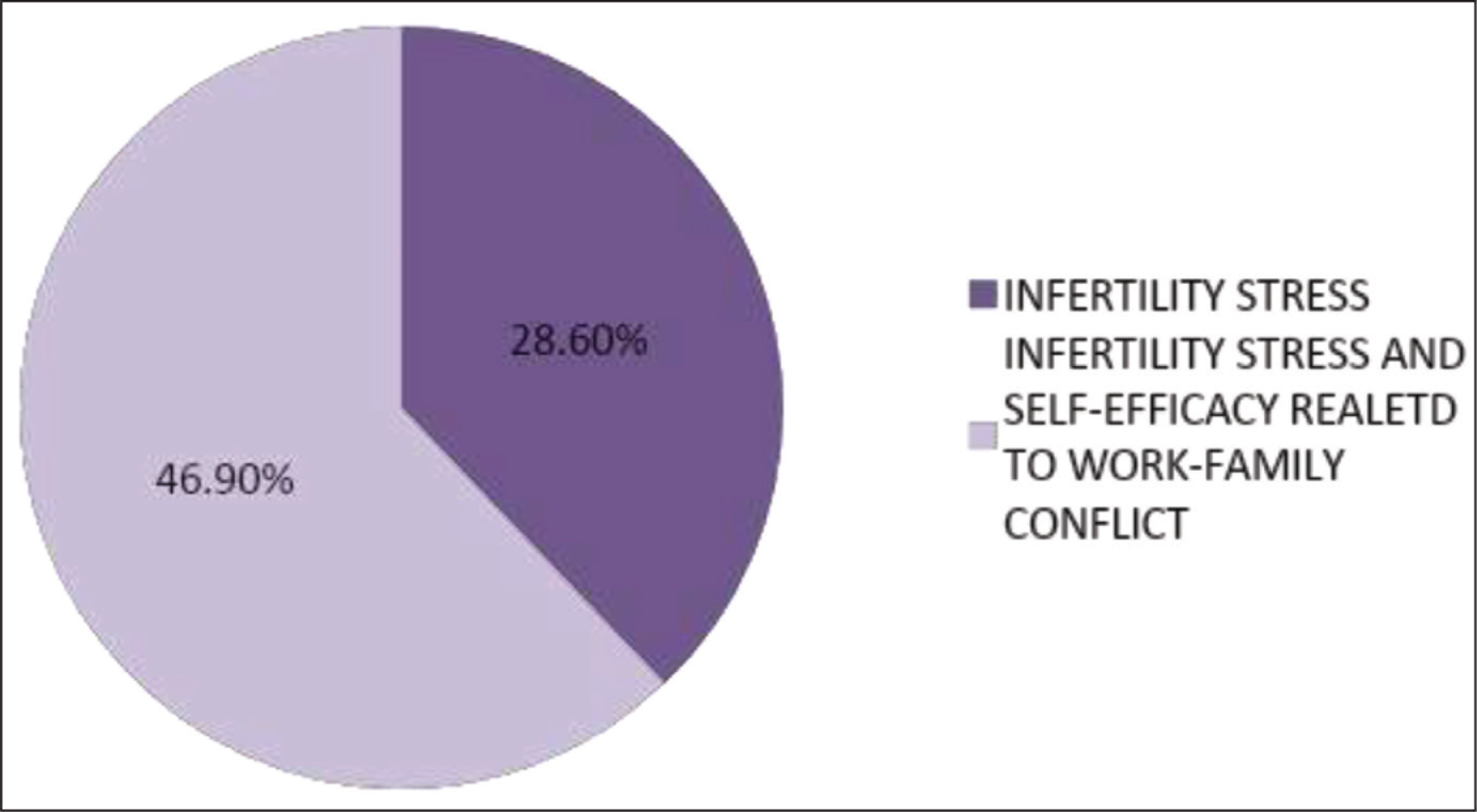
The analysis reveals that severity of medically unexplained infertility can be explained in terms of “self-efficacy related to work-family conflict” and “perceived infertility stress”; 28.6% of variation in severity of unexplained infertility being contributed by “self-efficacy related to work-family conflict” and 46.9% of the variation in the severity of unexplained infertility being contributed by a conjunction of “perceived infertility stress” and “self-efficacy related to work-family conflict.”
Conclusion:
The findings imply that urban educated women tend to place more psychological emphasis on “motherhood,” and “perceived deficit in attaining motherhood” seems to be the important source of personal stress for these women in comparison to stressors emanating from occupational hazards and family dynamics related to decision-making.
Introduction
Despite advancement in the understanding of neuroendocrinology of reproduction, many couples across the world suffer from involuntary childlessness. According to the National Fertility Association (2017), it can be estimated that 1 in 8 couples have trouble getting pregnant or sustaining a pregnancy. The relationship between psychological stress and infertility has always been a contentious issue. But interestingly, more often than not, discrete medical cause behind infertility is not identified, leading to the speculation that psychological factors might also act as antecedents of infertility. Contemporary societies have seen an influx of women workforce in traditionally male-occupational bastions. But women, more specifically women hailing from traditional milieu, are still expected to give primary importance to stereotyped feminine obligations like household chores, motherhood, and so on. These social coercions insidiously impede the woman’s experience of well-being and may be manifested in terms of a woman’s inability to bear a child. In many societies, the lack of ability to bear a child is associated with social ostracization and stigma. This inevitably leads to feelings of shame, guilt, and poor marital quality and may also manifest in terms of mental health hazards like low self-esteem, depression, anxiety, loneliness, and so on. Thus, it is reasonable to assume that among the multitude of psychosocial factors which might act as sources of trepidation, for the modern urban woman, occupation-related stressors play a significant role in their fecundity. Research on women’s health has inadvertently neglected the role of these surreptitious psychosocial determinants of female infertility.
This study thus aims to explore the role played by psychosocial factors mediating a woman’s lifestyle in the family and workspace in the existence of medically unexplained infertility.
Materials and Methods
Participants
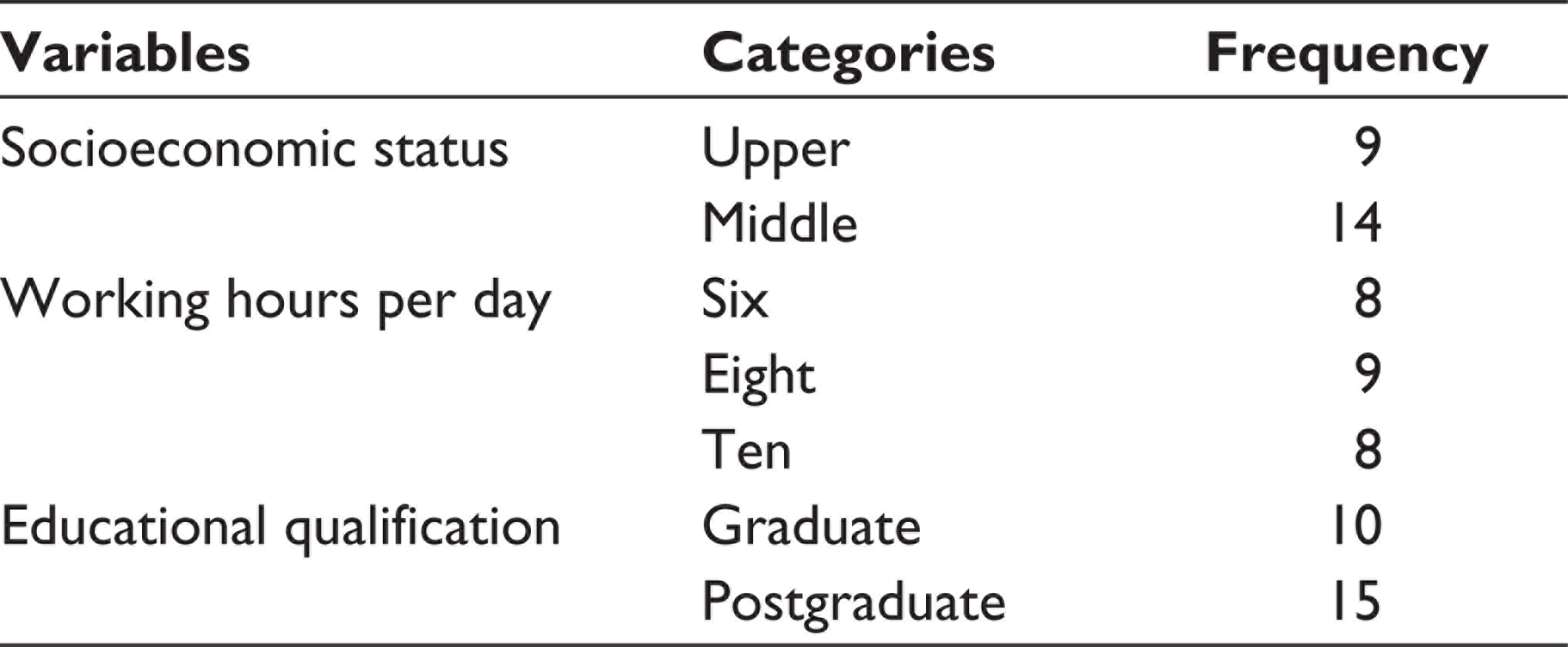
The participants of this study consisted of 25 married heteronormative females of the age range 28 to 40 years who have been experiencing an inability to conceive without any apparent medical cause for a duration of minimum 1 year. The mean duration of unexplained infertility of the participants was 5 years (SD = 1.83) (Table 1a). All the participants were graduates and employed and identified themselves as heteronormative and proclaimed themselves as married (Table 1b). Individuals with significant medical (eg, diabetes, hypertension, etc) and psychiatric illnesses were excluded. Also, females whose husbands have been diagnosed of having problems related to fertility were not considered for the study.
Showing the Mean and Standard Deviation of Age and Duration of Infertility of the Sample

Frequency of Socioeconomic Status, Working Hours, and Educational Qualification
Tools Used
The following constructs viz (a) self-efficacy related to work-family conflict—measured in terms of “work-family conflict self-efficacy scale” by Cinamon, 1 (b) perceived occupational stress—measured in terms of “work-to-family conflict scale” by Netemeyer et al, 2 (c) decision-making in family—measured in terms of “decision-making scale” by Blood and Wolfe, 3 (d) perceived infertility stress—measured in terms of “fertility problem inventory” by Newton et al 4 were assessed in the participants. All the scales mentioned above have been previously used in a number of research articles in reputed journals and have been reported to have adequate reliability and validity (ranging from 0.75 to 0.9). Though none of these scales have been standardized in the Indian population, the researchers still preferred them because of the fact that the nature of the items in the scales and the areas explored were relevant to the research question under consideration. At the onset, however, a “socio-demographic data sheet” is used to elicit/exclude significant psychiatric and/or medical diagnosis of the participants and other relevant details such as diagnosed infertility issues of the husbands, and so on. The key researcher was a trainee Clinical Psychologist and was proficient in elicit psychiatric history and conducting Mental Status Examination. As and when required, the supervisor who is also trained in Clinical Psychology, accompanied the key researcher during the evaluation of the mental state of the participants. The history sheet of the participants recorded in the clinics was used to identify significant medical problems. The diagnosis and documentation of medical problems were done by certified physicians associated with the clinics.
2.3 Procedure
The research-related information was gathered from a few infertility clinics in Kolkata, West Bengal, India. The initial process consisted of submitting an application related to the nature, scope of the research, and ethical issues pertaining to the research to the clinic authorities. The fertility clinics from which the participants of the study were recruited had their own research ethics committee which dealt upon the synopsis submitted by the key researcher. On being sanctioned, the researcher met the prospective participants, debriefed them about the purpose of the research, and also about the ethical issues involved. The participants were explained about the absence of any benefit (medical or financial) for participating in the research and the right to discontinue at any phase of research without fear of any detrimental consequences. Only those individuals who gave voluntary consent and who did not express any psychological distress while responding to the questionnaires were included in the study. Stepwise multiple regression analysis was done to find out the contributory role of the psychological constructs in the severity of unexplained infertility, as measured in terms of duration of involuntary childlessness.
Discussion
The major finding of this research has been that 28.6% (P < .05) of the variation in the scores of “medically unexplained infertility” can be explained in terms of variation in the scores of “perceived infertility stress” (Table 2). It has also been found that “perceived infertility stress” and “self-efficacy related to work family conflict” together can explain 46.9% variation in the scores of severity of “medically unexplained infertility” (Figure 1). It is noteworthy that “perceived occupational stress” and “decision-making in family” have not been found to play a contributory role in the severity of “medically unexplained infertility.”
Stepwise Regression Analysis to Show the Predictors of Severity of Infertility in Terms of Its Duration

bPredictors: (Constant), perceived infertility stress, self-efficacy related to work-family conflict.
Pie Chart Showing the Percentage of Variation in the Severity of “Unexplained Infertility” in Terms of Its Duration Brought About by the Predictors
Showing Correlation Among the Variables
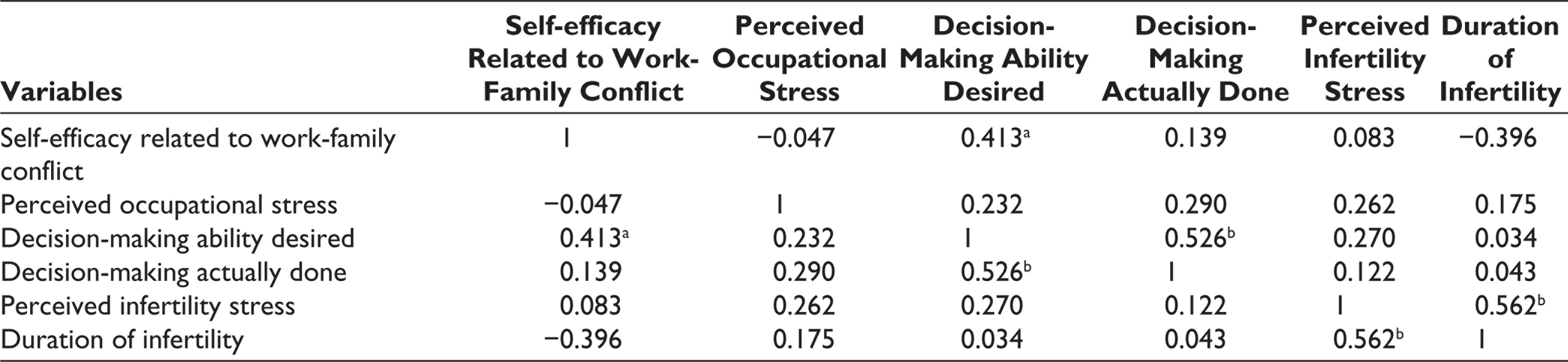
bCorrelation is significant at the 0.01 level (2-tailed).
The findings imply that urban-educated women tend to place more psychological emphasis on “motherhood,” and “perceived deficit in attaining motherhood” seems to be the important source of personal stress for these women in comparison to stressors emanating from occupational hazards and family dynamics related to decision-making. However, “self-efficacy related to work-family conflict” has also been found to be one of the predictors, albeit as an adjunct with “perceived infertility stress” (Table 3). This means that the belief to be able to successfully handle occupational and familial demands also plays a critical role in shaping the self-worth and sense of well-being in urban-educated women.
Greenhaus and Beutell 5 defined “work-family conflict” as a form of inter-role conflict in which work and family pressures are mutually incompatible and are important sources of stress both in the familial and the occupational sectors. 6 It is more than apparent that social context and gender-based socialization experiences may act as facilitators or barriers to women’s experience of self-efficacy related to multiple-role performance. According to Ozer, 7 perceived self-efficacy to blend multiple role demands is directly related to felt physical and emotional strain in women. Similar findings were obtained by Cinamon 8 wherein decreased sense of self efficacy was found to be related to higher anticipated levels of work-family conflict.
Self-perceptions are intricately tied with the importance that a person confers to various social roles he/she is expected to play. This process is termed as “role salience,” 9 “role centrality,” 10 “role commitment.” 11 In almost all societies, women are expected to fulfill family obligations over and above other social roles. In traditional societies like India, the conventional roles of a woman as a homemaker are deeply entrenched in the minds of individuals of either sex. Hence, though there has been a surge in the participation of women in the formal work force in the last few decades, balancing work and family has been a crucial challenge for Indian women. The process of balancing the competing demands of job and family is a major source of stress for women, often manifested in terms of anxiety, depression, or psychosomatic problems like headache, diabetes, hypertension, and so on.12,13 Uma Rani and Bhuvaneswari 14 noted that there exists a high general level of stress in working women belonging to the age group of 29 to 32 years. Wang et al 15 examined relationships between two dimensions of work-family conflict, that is, work interfering with family (WIF) and family interfering with work (FIW) across heteronormative males and females in India and China. They found that there exists a higher degree of negative correlation between work family conflict, self-efficacy, and work satisfaction in women in comparison to men in both India and China. In fact, the fact that sex plays a contributory role in the anticipated levels of work family conflict in the Western society as well was also confirmed by Cinamon. 8 She found that women anticipated higher levels of WIF and FIW and demonstrated lower efficacy in managing these conflicts than did men.
Thus, it is more than apparent that sex influences the way we perceive roles, priorities, and juggling between multiple roles and that heteronormative women differ substantially from men in the manner in which they define, enact, and manage multiple social roles. The intrinsic social coercion to perform domestic responsibilities perfectly, the inequity between male and female roles in the domestic sphere, 16 and socialization experiences of Indian females whereby they internalize these norms and expectations are the potential causes of psychological stress in Indian working women. In fact, there are studies that have reported that owing to this continuous striving to achieve work and family balance, women often do not get adequate time for leisure and recreation. 17
Fouad and her colleagues 18 had commented on the basis of her study that in India, the career and life choices of women are often a reflection of parental and family directives instead of personal choices. Valk and Srinivasan 17 further found that Indian women professionals reported that they were not able to pursue personal interests due to family commitments and that they were open to the choice of “making sacrifices” for the sake of a greater cause, that is, “work-family balance.”
Since the basic question addressed by this research was whether infertility in heteronormative women is associated with psychosocial factors instating a cascade of physiological changes instead of pure biological factors, the researchers have considered only heteronormative females for their study. This does not indicate their disregard toward the transfeminine and the stress experienced by them regarding issues of child bearing. Also, the social markers of women’s emancipation are opportunities for education of women, entry of women in workforce, women spending a significant duration of fertile years in non-child-bearing pursuits, increase in age of marriage and the birth of the first child. Hence, it is desirable that readers note that the purpose of this research is not to reinforce misogynistic attitudes toward women’s independence, but just to highlight that certain psychosocial factors related to the socialization of women also play a role in reduced fertility. In this context, it is also pertinent to highlight that the psychosocial factors identified with reduced fertility in women are not causative agents, but merely have an association.
Conclusion
In an extensive literature survey on the potential effects of stress on female fertility, Palomba and co-researchers 19 found that though it is difficult to unravel a cause effect relationship between stress and female fecundity, a strong correlation exists between measures of quality of life, stress, and reproductive function, more specifically in women who are experiencing problems of infertility.
Though there does not exist any direct or objective measure of human psychological stress and its impact on the physiological system, chronic psychological stress is linked with activation of hypothalamic-pituitary-adrenal axis and the sympathetic-adrenal-medullary axis 20 which initiate a cascade of neuroendocrine changes, potentially damageable for female fertility.21,22 Several studies have underlined a possible relationship between high levels of perceived stress and higher levels of cortisol, and infertility. 23
A woman’s self-perception, irrespective of her education and occupational status, is strongly influenced by social expectations from them, which mostly revolve around roles of a caregiver and motherhood. Decisions related to motherhood accentuate this tension around a woman’s identity. In the process of negotiating between personal choices, social mores, and family obligations, women often fall prey to psychological stress. Thus, it is of pivotal importance to explore the seemingly medically irrelevant psychosocial factors which might subtly and insidiously affect the female reproductive function.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the Departmental Research Committee in matters of ethics. Further, informed consent was taken from all the participants prior to the onset of the research.