
Abstract
Aim:
To evaluate the marital profile, family size, fertility rates, and perception about various aspects of marriage among the couples, with one of the partner having schizophrenia and compare the same with a group of couples, with one of the partner having recurrent depressive disorder (RDD).
Methodology:
A total of 76 married patients with schizophrenia and 58 married patients with RDD were evaluated by using a semistructured interview, which covered information about the duration of marriage, number of children, different aspects of marital and sexual life like perception about marriage, mental illness, sexual compatibility, and other variables.
Results:
A significantly higher proportion of patients with schizophrenia had onset of illness prior to marriage, when compared to the patients with RDD. There was no significant difference between the 2 groups in terms of mean number of children, number of spontaneous abortions, and medical termination of pregnancies. The mean numbers of postnatal deaths were significantly higher in the group in which one of the partners was diagnosed with schizophrenia. Compared to spouses of patients with RDD, higher proportion of the spouses of patients with schizophrenia reported sexual incompatibility since the beginning of the marriage and lack of full satisfaction with sexual life. Compared to patients with RDD, higher proportion of patients with schizophrenia were worried about their children developing mental illness and believed that people with mental illness should not marry.
Conclusion:
To conclude, this study demonstrates that compared to the spouses of patients with RDD, spouses of patients with schizophrenia have higher negative perception about the marriage.
Introduction
Marriage is a social commitment, which is associated with multiple emotional and social demands. 1 The need to get married does not go away with development of a severe mental disorder like schizophrenia. The association between marriage and schizophrenia has been studied in the form of marital rates, marriage as a stressor for onset/relapse of illness, impact of marriage on the course and outcome of illness, outcome of marriage in patients with schizophrenia, marriage as a protective factor from developing mental disorders, perception about impact of marriage on mental illness, marital functioning/satisfaction among patients with schizophrenia (and or their spouses), sexual dysfunction/satisfaction among patients with schizophrenia (and or their spouses), number of children among patients with schizophrenia, and impact of schizophrenia on spouses, etc. 1
In terms of marital rates, data from the developed countries reflect that compared to the marital rates among normal subjects or those with other psychiatric disorders, marital rates are lower among patients with schizophrenia.2-7 The lower marital rates are more common among male patients. 8 The lower marital rates are attributed to poor premorbid adjustment impacting the heterosexual relationships, younger age of onset of illness, symptomatology, and socio-occupational disability. 8 However, studies from developing countries, especially India reflect that a large proportion of patients with schizophrenia get married. A cohort study from India involving 76 patients with first episode schizophrenia, followed up for 10 years reported that 70% of patients eventually got married. 8 Further all those subjects who were unmarried at the time of follow-up were below 40 years, with a further possibility of getting married. 8 Further, the authors reported good marital outcome was associated with high marital rates, having children, shorter duration of illness at the time of inclusion, presence of auditory hallucinations at intake. Poor marital outcome was associated with unemployment, drop in socioeconomic level, presence of flat affect, and self-neglect for a prolonged period. 8 A study from Ethiopia reported marital rate of 70.5% among patients with Schizophrenia. 9 Another cross-cultural study, which evaluated marital rates among patients of schizophrenia from India and United States of America reported that males were more likely to be single compared to females in the United States. However, in India, there was no difference between the subjects with respect to marital rates. 10 In terms of factors associated with marriage, a 13-year follow-up study suggested that “currently single” status (ie, single, separated, or divorced) is more frequently associated with onset of illness before 25 years of age. 11 A study from China reported urban rural difference in the rate of marriage among female patients with psychosis. Compared to rural female patients, those from urban locality were 2.7 times more likely to be unmarried. The authors further noted that the marital disadvantage was noted among urban females who had early onset of illness. No such differences were noted for males. 12
There is some evidence to suggest that among patients with schizophrenia fertility and reproduction rates are also low. 13 Studies from the West suggest that male patients with schizophrenia have reduced procreation rates compared with female patients. 10 The cross-cultural study that evaluated patients of schizophrenia from India and United States of America also found males to more often being childless compared to females, whereas no such gender difference was seen in Indian sample. 10
Little is understood about the impact of living with a spouse with mental illness. Very few studies have focused on the spouse of patients with schizophrenia. In a cohort study of 76 patients, authors reported that of those who got married, in 80% of cases the marriage was intact. 8 However, it is suggested that an intact marriage does not necessarily reflect a harmonious marriage. The presence of a child could place some obligation on the couple to stay together and in its absence the marriage could breakdown easily. 8
A study from Ranchi evaluated the marital adjustment among patients with schizophrenia, depression, and bipolar disorder and their spouses and showed that compared to patients of affective disorders, patients with schizophrenia had significantly higher rate of marital maladjustment. However, compared to patients, spouses reported lower rates of marital maladjustment. The marital maladjustment in patients was associated with poor quality of life. 14 Another study from the same center compared the marital adjustment of patients with schizophrenia, bipolar affective disorder (BPAD) and substance dependence reported poor marital adjustment in 60% of patients with schizophrenia, which was lower than observed in patients with BPAD (70%), but higher than that noted in patients with substance dependence (50%); however, the differences were not statistically significant. Compared to patients with substance dependence, patients with schizophrenia have significantly poorer sexual adjustment. 15 However, these studies do not provide information about specific aspects of marital and sexual problems.
In India, different beliefs are associated with marriage and mental illness. One of the common beliefs includes marriage as a cure for mental disorders including psychoses. 16 This possibly gets reflected in high rate of marriage among patients of schizophrenia. Despite high marital rates, little is known about the procreation rates among patients with schizophrenia. In general, the perspective of spouse of patients with schizophrenia is infrequently evaluated. Accordingly, this study aimed to evaluate the marital profile, family size, fertility rates, and perception about various aspects of marriage among couples with one of the partners having schizophrenia and compare the same with couples with recurrent depressive disorder (RDD).
Methodology
This study involved patients with schizophrenia and RDD and their spouse, attending the outpatient services of a tertiary care hospital. The study participants were recruited after they provided the written informed consent. The study was approved by the Ethics Committee of the Institute. The data presented in this article is part of the larger study, which evaluated the marital functioning, sexual satisfaction, and sexual dysfunction among patients with schizophrenia and their spouses. Data on marital and sexual functioning have been published earlier 17 and details of the methodology are provided in this article. We would briefly discuss the methodology here.
The study included 76 couples with one of the partners with schizophrenia and 58 couples with one of the partners having RDD. To be part of the study, the couple were required to be aged ≥18 years and married for at least 1 year. Additionally, patients were required to have illness for at least 1 year and participants being able to read Hindi and/or English. Presence of comorbid substance dependence, organic brain syndrome, and intellectual disability led to exclusion of the patients.
The diagnosis of schizophrenia and RDD was confirmed by using Mini-International Neuropsychiatric Interview. 18 The study was limited to the patients in clinical remission and clinically stable. Clinical remission was defined by using the criteria proposed by Andreasen et al 19 for schizophrenia and a score <7 on the Hamilton Depression Rating Scale (HDRS) for depression. 20 Clinical stability was defined by lack of worsening of symptoms or relapse of symptoms or ≥50% hikes in medication dosages in the 3-month period prior to intake. Residual psychopathology was evaluated by using Positive and Negative Syndrome scale for Schizophrenia (PANSS) 21 and HDRS 20 in patients with schizophrenia and RDD, respectively.
Additional inclusion criteria for spouses were free from any diagnosed physical or psychiatric morbidity (other than tobacco dependence) and able to read Hindi and/or English. Details of the marriage were evaluated by using a semistructured interview, which covered information about the duration of marriage, number of children, number of spontaneous abortions, number of medical termination of pregnancies, sexual compatibility, attitude toward marriage, satisfaction with marriage, whether people with mental illness should marry or not, care provided to children, etc. The information on these variables was obtained separately from the patient and the spouse. In addition, the couple was evaluated for sexual compatibility and satisfaction with sex life, the care provided to children, worries related to children developing mental illness in future and attitude toward marriage of people with mental illness. Additionally, spouses were asked further regarding their perception about marriage in terms of feelings of being cheated, thought of separating from the spouse and their perception about marriage and mental illness.
Data Analysis
Statistical Package for Social Sciences (SPSS-14) was used to analyze the data. Descriptive analysis in the form of frequencies, percentages, mean, and standard deviation was done. The study groups were compared by using Student’s t-tests, Mann-Whitney U tests, and chi-square tests.
Results
Sociodemographic Profile of Patients and Spouses
The mean age of patients of schizophrenia was 40.86 (SD: 8.43) years and the mean age of patients with RDD was 43.44 (SD: 7.69) years. The mean education in years was slightly more than 10 for both the groups, with no significant difference between the groups. In both the groups, more than half of the patients were females (schizophrenia: 55.3% and RDD: 69%), educated less than or equal to matric (schizophrenia: 52.6% and RDD: 51.7%), currently not on paid employment (schizophrenia: 55.3% and RDD: 51.7%), from lower middle or lower socioeconomic status (schizophrenia: 61.8% and RDD: 60.3%), Hindu by religion (schizophrenia: 75% and RDD: 62.1%), and from non-nuclear families (Schizophrenia: 53.9% and RDD: 55.2%). Majority of the patients in the either group were from rural background (schizophrenia: 82.9% and RDD: 77.6%). When both the groups were compared on all these demographic variables, there was no statistically significant difference between the groups.
The mean age of spouses of patients with schizophrenia was 40.87 (SD: 9.92) years, and the same for spouses of patients with RDD was 44.43 years, with no significant difference between the 2 groups. The mean duration of education in years was slightly more than 10 years for both the groups. More than half of the spouses for both the groups were educated beyond matric and about two-third in both the groups were on paid employment. Although spouses of patients in either group were in the caregiver role for about 10 years, compared to spouses of patients with RDD, spouses of patients with schizophrenia were spending significantly more number of hours in caregiving [3.95 (SD: 1.51) vs 2.06 (0.46); t-test value = 10.31, P < .001***].
Clinical Profile of Patients With Schizophrenia and RDD
Compared to patients with RDD, patients with schizophrenia had significantly lower age of onset [29.83 (SD: 8.52) vs 33.65 (7.8); t-test value = 2.67, P = .009**]. However, both the groups did not differ in terms of duration of illness in years, duration of treatment in years, and duration of current remission. The mean PANSS score at the time of assessment was 44.66(10.43) for patients with schizophrenia, and the mean HDRS score for patients with RDD was 4.15(1.04).
Marital Profile
The details of the marriage and family size of the study participants are given in Table 1. Compared to patients in the RDD group, a significantly higher proportion of patients with schizophrenia had onset of illness prior to marriage. The mean number of postnatal deaths were significantly higher in the group in which one of the partners was diagnosed with schizophrenia (Table 1).
Details of Marriage and Family Size of Patient With Schizophrenia and RDD
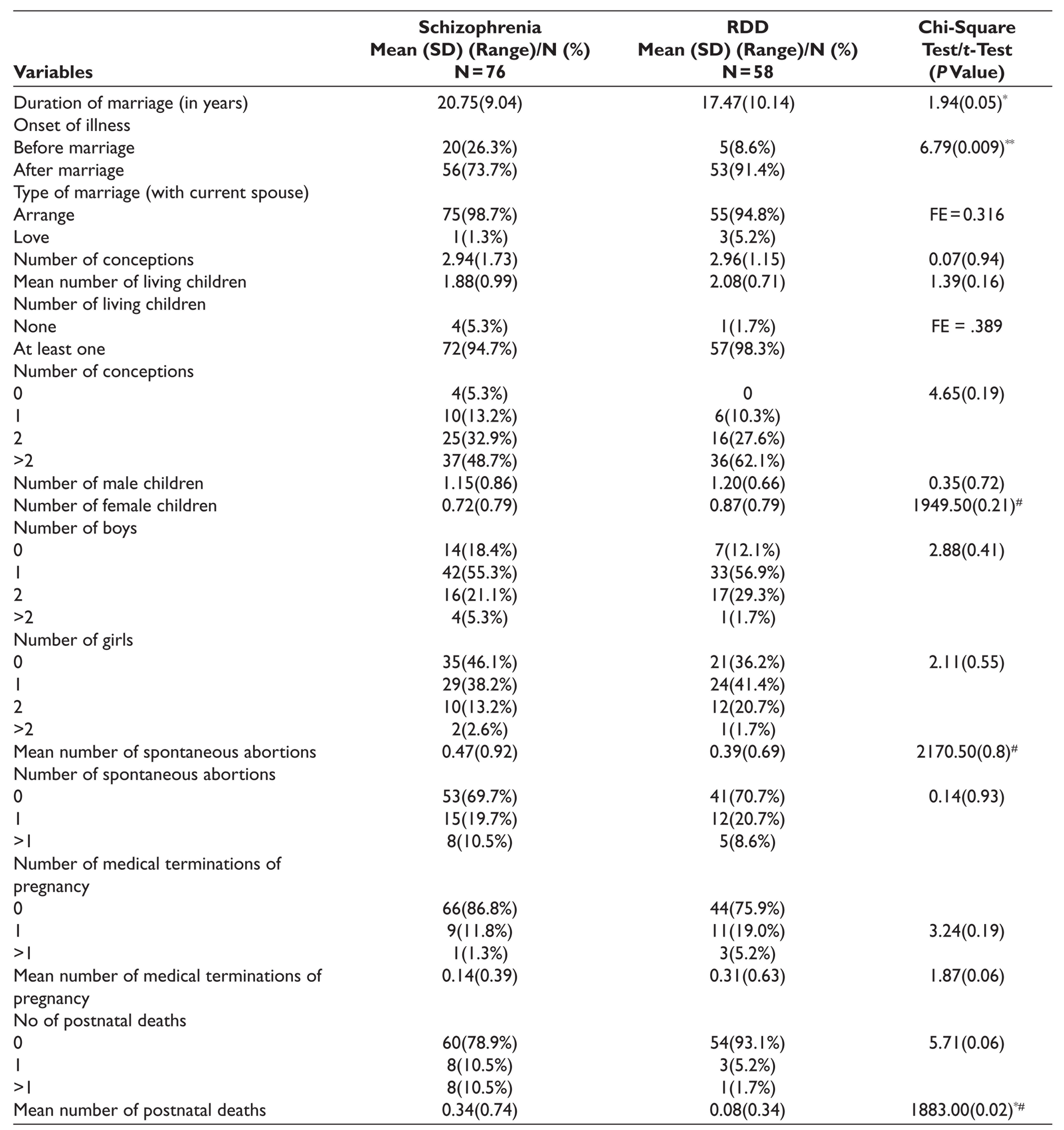
FE = Fischer exact value; *P ≤ .05; **≤.01. #Mann-Whitney U value.
When male and female patients with schizophrenia were compared, it was evident that, compared to females, in a significantly higher proportion of male patients the onset of the illness was prior to marriage (44.1% vs 11.9%; chi-square value: 10.05; P = .002**). There were no statistically significant differences between males and female patients with schizophrenia on any of the other variables. When those with schizophrenia, with onset before and after marriage, were compared, significantly higher proportion of those who had onset before marriage had no living children (15% vs 1.8%; chi-square value: 4.4; P = .04*) and no boy child (35% vs 12.5%; chi-square value: 7.83; P = .05*). There were no statistically significant differences for any of the other variables.
When similar comparisons were done for patients with RDD, no significant differences were noted in terms of influence of gender and onset of illness, before or after marriage.
Sexual Adjustment as Perceived by Patients and Their Spouses
In both the groups, very few patients and their spouses reported sexual incompatibility since the beginning of marriage. More than two-third of the patients in either group reported lack of satisfaction with their sexual life. Compared to spouses of patients with schizophrenia, higher proportion of spouses of patients with RDD reported full satisfaction with their sexual life, this difference between 2 groups was statistically significant (Table 2). No significant difference was noted between male and female patients with schizophrenia and also RDD on any of these variables. Similarly, no significant difference was noted between those with onset of illness before or after marriage for both the groups on any of these variables.
Details of Sexual Life as per Patient With Schizophrenia and Recurrent Depressive Disorder (RDD) and Their Spouses
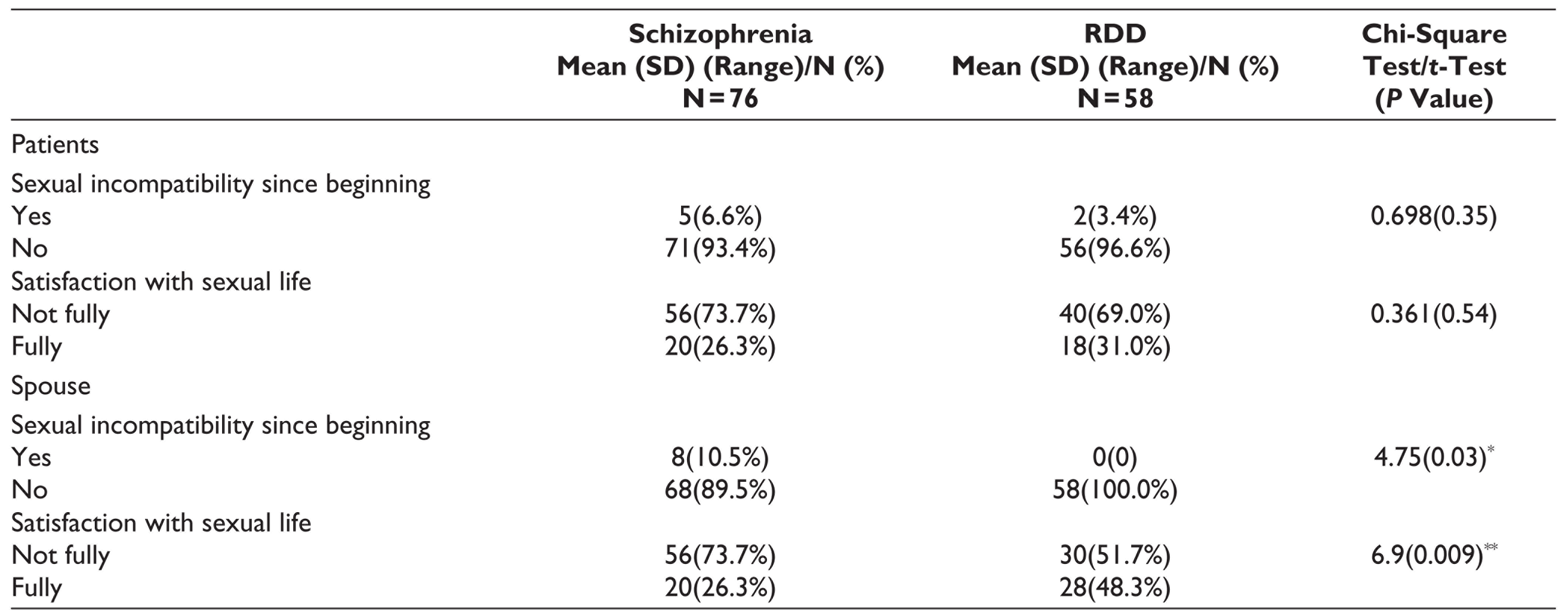
*P ≤ .05; **P ≤ .01.
Attitude Toward Marriage and Perception of Marital Functioning as per Patient With Schizophrenia and Recurrent Depressive Disorder (RDD) and Their Spouses
Most of the patients in either group were fully satisfied with the care provided to the children by their healthy spouse. Significantly higher proportion of patients with schizophrenia were worried that their children may develop mental illness and higher proportion of patients with schizophrenia felt that patients with mental illness should not get married. Compared to spouses of patients with schizophrenia, significantly higher proportion of spouses of patients with RDD were satisfied with the care provided to children by their spouses. Compared to spouses of patients with RDD, higher proportion of spouses of patients with schizophrenia felt cheated, were worried that their child(ren) may develop mental illness, felt like separating from their spouse, believed that patients with mental illnesses should not get married, and believed that marriage can worsen mental illness. Majority of the spouses of patients in either group believed that marriage can be a treatment for mental illness, marriage can be a cure for mental illness, and marriage can help in improving mental illness. A small proportion of spouses of patients in either group accepted of having extramarital relationships (Table 3).
Attitude Toward Marriage and Marital Functioning as per Patient With Schizophrenia and Recurrent Depressive Disorder (RDD) and Their Spouses
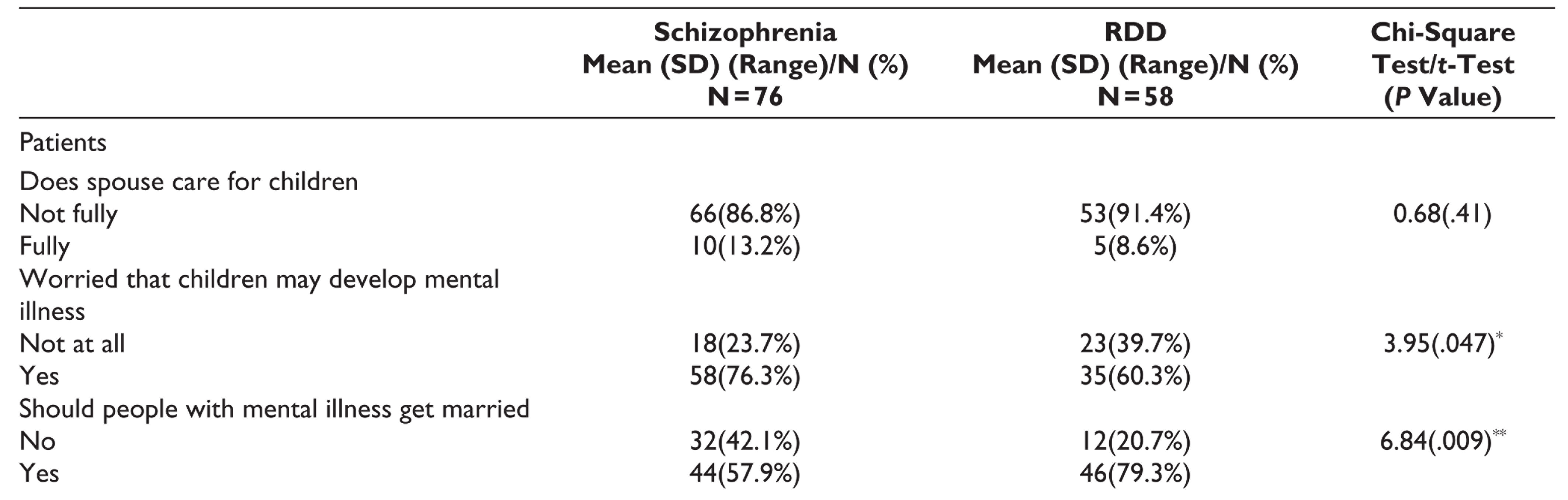
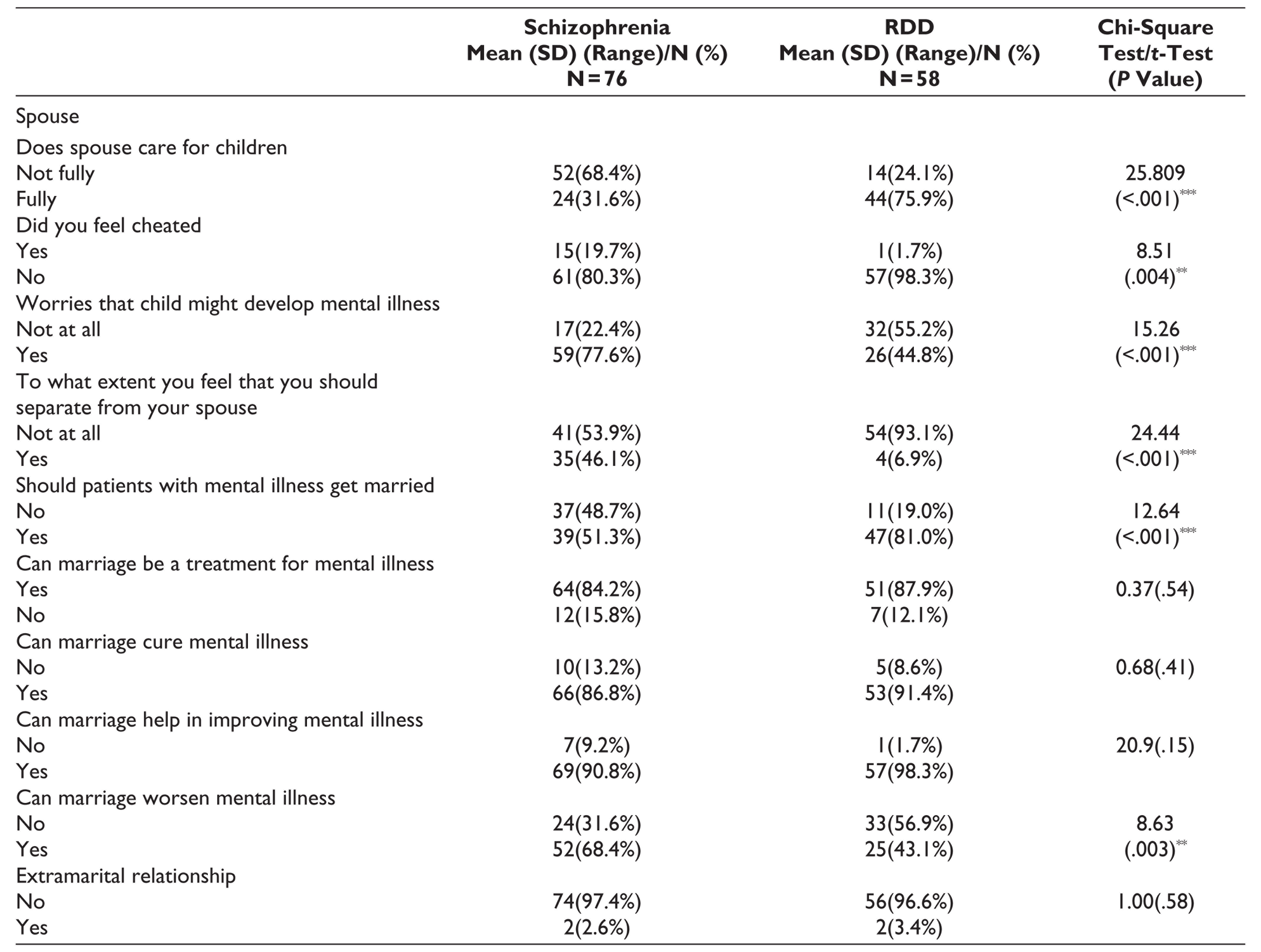
*P ≤ .05; **P ≤ .01; ***P ≤ .001.
When similar comparisons were made for male and female patients of schizophrenia and their spouses, no significant difference was noted on any of these variables between the participants of either gender except that significantly higher proportion of male spouses reported of having a feeling of being cheated (90.5% vs 67.6%; chi-square value: 4.82; P = .02*). However, in the RDD group, when similar comparisons were made for male and female patients and their spouses, no significant difference emerged. When similar comparisons were made for patients and spouses with onset of illness before and after marriage, no significant differences emerge for the patients and the spouses.
In the RDD group, higher proportion of the spouses of patients who had onset of illness prior to marriage thought of separating from the patient (40% vs 3.8%; FE = 0.003**).
Discussion
Compared to the West, higher proportion of patients with schizophrenia, do get married in India. Little is known about the marital functioning, family size, and perception about marriage among patients with schizophrenia and their spouses. Although some of the studies have evaluated sexual and marital functioning of patients with schizophrenia in the Indian context, available data are limited. Accordingly, this study attempted to assess the family size, fertility rates, and perception about various aspects of marriage among patients with schizophrenia and their spouses and compare the same with a group of patients with RDD and their spouses.
The mean duration of being married was significantly longer for the couples with one of the partners having schizophrenia, compared to participants in the RDD group. When compared to the patients in the RDD group, significantly higher proportion of patients with schizophrenia had onset of illness prior to marriage. Higher rates of onset of illness prior to marriage among patients with schizophrenia can be understood from the perspective of age of onset of the 2 disorders. It is well known that schizophrenia often starts in second or third decade of life, whereas depressive disorders start in third or fourth decade of life.22,23 This differential age in onset can explain the significant difference seen in the present study for the association of age of onset and marriage. Very few patients in both the groups had love marriage. There was no significant difference between the two groups, with respect to number of living children, total number of conceptions, mean number of children of either gender, and mean number of spontaneous abortions. However, compared to the couple with one partner having RDD, higher proportion of couple with one partner having schizophrenia had no children or had single child and had history of higher mean number of postnatal deaths. Comparative studies involving patients of schizophrenia and RDD for these variables are not available. Higher mean number of postnatal deaths among couple with one partner having schizophrenia possibly reflect the poor parenting skills, which have been reported to be highly prevalent among patients with schizophrenia.24,25 Higher proportion of couples with one partner having schizophrenia having higher prevalence of “no child” or “1 child” could be due to multiple reasons. This could reflect lower fertility rates or could be a reflection of difficulties in parenting, fear of exposure of pregnancies to psychotropics, and fear of children having mental illness in future.
When male and female patients with schizophrenia were compared, no significant differences emerged on any of these variables. However, when similar comparisons were made for patients with RDD, it was evident that compared to females, in significantly higher proportion of male patients, illness started prior to marriage, and medical terminations of pregnancies were higher when the patient was a female. This possibly reflects the gender bias toward the mentally ill subjects. In routine clinical practice, it is often noted that female patients with mental illness face difficulty in getting a match compared to male patients. These findings possibly provide credence to these observations.
There is lack of data on sexual compatibility and sexual satisfaction among patients with schizophrenia and their spouse. In the present study, very few patients and their spouses reported sexual incompatibility since the beginning of marriage. However, compared to spouse of patients with RDD, higher proportion of spouses of patients with schizophrenia reported sexual incompatibility between them since the beginning of their marriage. This may be a reflection of poor emotional expression, poor initiation of sexual act, or actual sexual dysfunction on the part of patients with schizophrenia.
More than two-third of the patients in either group reported, lack of full satisfaction with their sexual life. Very few spouses of patients with schizophrenia reported full satisfaction with their sexual life, whereas about half of the spouses of patients with RDD reported “full satisfaction” with sexual life and this difference between the two groups was statistically significant. Overall it can be said that spouses of patients with schizophrenia face higher level of sexual incompatibility and lower level of sexual satisfaction, compared to spouses of patients with RDD. Accordingly, it can be said that while evaluating and addressing the sexual issues of patients of schizophrenia, a thorough evaluation of spouse also must be done and if required both the partners must be engaged in sex therapy to improve the outcome of couple.
Attitude Toward Marriage and Perception of Marital Functioning
Most of the patients in either group were fully satisfied with the care provided to children by their spouse. Significantly higher proportion of patients with schizophrenia were worried that their children may develop mental illness and higher proportion of patients with schizophrenia felt that patients with mental illness should not get married. These findings possibly reflect the knowledge of patients of schizophrenia about the nature of the illness, risk of genetic transmission, and distress associated with the whole experience of the illness.
Compared to spouses of patients with schizophrenia, significantly higher proportion of spouses of patients with RDD were satisfied with the care provided to children by their spouse with mental illness. Studies from different parts of the world suggest that compared to healthy controls, parenting skills are impaired in patients with schizophrenia. 24,25 Higher level of dissatisfaction with parenting provided by patients with schizophrenia suggests that parenting skills of patients with schizophrenia is more impaired compared to patients with RDD. This could be understood in light of the nature of both the disorders.
Compared to spouses of patients with RDD, higher proportion of spouses of patients with schizophrenia felt cheated, were worried that their child(ren) may develop mental illness, felt like separating from their spouse, believed that patients with mental illnesses should not get married, and believed that marriage can worsen mental illness. These findings possibly reflect the marital dissatisfaction in the spouses of patients of schizophrenia. For patients of schizophrenia, a significant proportion of caregivers are spouses.26-29 Hence, the clinicians must understand their emotional distress and provide support to overcome the same.
Surprisingly, majority of the spouses of patients in either group believed that marriage can be a treatment for mental illness, marriage can be a cure for mental illness, and marriage can help in improving mental illness. These possibly reflect the general cultural belief associated with mental illness and marriage. 30
When similar comparisons were made for male and female patients and their spouses, no significant differences were noted on any of these variables between the participants of either gender except that significantly higher proportion of male spouses of patients with schizophrenia reported of being cheated. This possibly reflects the gender bias which exists in the society, where females are expected to adjust in a marital unit more than the males.
Conclusions
To conclude, present study suggests that among spouses of patients with schizophrenia, factors which are associated with poor marital adjustment included lesser number of children, sexual incompatibility since the beginning of marriage, lack of satisfaction with sexual life, poor care provided by mentally ill spouse to the children, feeling of being cheated in the married life, and a feeling of need to separate from mentally ill spouse, belief that people with mental illness should not marry and worry about children developing mental illness.
Among the spouses of patients with RDD, factors that are associated with poor marital adjustment and sexual satisfaction include poor care of children by mentally ill spouse, feeling of being cheated, worry about children might develop mental illness, feeling of need to separate from the mentally ill spouse, being critical of spouse, being criticized by the mentally ill spouse, getting more upset with criticism, longer duration of being in caregiver role, higher level of psychological morbidity, and higher subjective tension in terms of caregiver burden.
Considering these findings of this study, it can be said that there is a need to assess and address marital and sexual issues among patients with schizophrenia and their spouses. However, these issues must not be underestimated in patients with RDD and their spouses too. Hence, due importance must be paid to the marital and sexual issues between the couple with one of the partners having schizophrenia and address the same.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.