
Abstract
Abstract
Aims: The study aimed to gather the perspectives of women with schizophrenia who had sexual dysfunction (SD) and to assess their perceptions related to discussions about sexual concerns with mental health professionals (MHP).
Settings: Female patients attending the outpatient department of a tertiary care university psychiatric hospital, who were diagnosed to have schizophrenia and in remission, were recruited and assessed for SD. Those who had SD and were willing to participate were interviewed for the qualitative study.
Methods and Materials: A guided interview format was used to gather their narratives. Interviews were transcribed and translated from audio recordings on the same day. The analysis of transcript from 9 patients reached theoretical saturation.
Analysis: The data were retrieved, coded, and systematically organized according to patterns and themes. The manual inductive coding method was used to arrive at the themes.
Results: 4 themes were found for the question assessing their perspective regarding SD and 3 themes on their perspectives regarding the discussion with MHP. Many of them had misconceptions regarding their sexual lives and the relationship between sexuality and their illness. It was evident that hardly any MHP had ever inquired about their sexual functioning.
Conclusion: This qualitative research on women with schizophrenia having SD gives us in-depth knowledge regarding their snags. Results of such studies will help the clinicians pay justifiable attention to these least spoken problems.
Introduction
Sexual dysfunction (SD) is a common problem among women with schizophrenia, but it is often overlooked not only in clinical practice but research as well. 1 SDs can diminish the quality of life, affect self-esteem, and cause interpersonal problems. 2 SD among patients with schizophrenia ranges from 30% to 80%. 3 SD in schizophrenia could be caused by negative symptoms, such as apathy and amotivation, and positive symptoms, such as delusions or hallucinations or side effects of medications.4, 5
Psychiatrists bear an important responsibility in effectively addressing sexual problems. Nnaji et al found that two-thirds of the psychiatrists interviewed do not routinely question about SD in their patients and only 17% felt proficient in assessing SD, even though 88% agreed that good sexual function is important to patients. 6 It is, however, unclear whether clinicians underestimate the impact of SD or they do not know enough about the issue or feel ashamed of talking about these sensitive subjects. 3
Indian studies on SD have focused predominantly on males.7, 8, 9 In cultures like ours, discussion about female SD is still a taboo. 10 Indian researchers have found that female patients from India felt shy and reluctant to discuss SD or matters related to intimacy. 11 On the other hand, researchers themselves found it difficult to discuss such sensitive problems with female patients. 7 A study from India found that the majority of professionals (73.2%) did not enquire about SD in the routine clinical setting and agreed that they lack expertise. 11
Qualitative studies can enhance our understanding of human behavior and health services. They provide a basic understanding of complex situations that cannot be explained by quantitative methods. 12 Qualitative studies are even considered as central to health promotion research. 13
Hence, this qualitative study was designed to address the following key issues:
To elicit and gather perspectives of women with schizophrenia who had SD and understand their subjective experiences of the same. To assess women’s perceptions related to discussions about sexual concerns with mental health professionals (MHP) and their expectations from MHP in this aspect.
Methodology
Female patients attending the outpatient department of a tertiary care university psychiatric hospital, who were diagnosed to have schizophrenia according to International Classification of Diseases, Tenth Revision (ICD 10) 14 criteria, in remission were recruited and assessed for SD. The method of screening, assessment, and ethical clearance was described in detail elsewhere. 15 Among 63 women, 70% of them had SD. An invitation was given to all the patients who had been assessed to have SD, to participate in this study. A semistructured guided interview format was used to gather their narratives. It aimed at understanding the causes that the patient attributed to the SD and the impact that the sexual problem had caused on their marital relationship. Another objective was to explore patient’s experiences related to discussions about sexual concerns with MHP. Patients were encouraged to discuss these issues by using guided questions and prompts. They were encouraged to describe in detail about the factors that had contributed to their SD, and how that has changed their relationship with the partner. Interviews were transcribed and translated from audio recordings on the same day. Analysis of transcript from 9 patients reached theoretical saturation. The interviews were originally conducted in Kannada and Tamil and took place in a separate room ensuring safety, confidentiality, and privacy. Additional consent was taken from the patients for audio recordings. The Institutional Ethics Committee approved this study.
Data Analysis
The analysis was done using manual descriptive content analysis. The data were retrieved, coded, and systematically organized according to patterns and themes. As no prior theoretical framework was chosen to explain, manual inductive coding method was used to arrive at the themes. Both investigators undertook analysis, and reliability was enhanced by double coding the transcripts and comparing the interrater reliability. Codes were grouped together into themes and any differences between the investigators were resolved by discussion to arrive at a common consensus. 4 themes emerged for the first qualitative question and 3 themes emerged for the second question. The narratives were further analyzed in pertinent to these 4 themes to enhance the understanding of the patient’s perspectives.
Results
This will be broadly discussed in two divisions:
Patient’s perspective about the SD Patient’s perspective about the factors governing the discussion regarding patient’s sexual issues with the MHPs
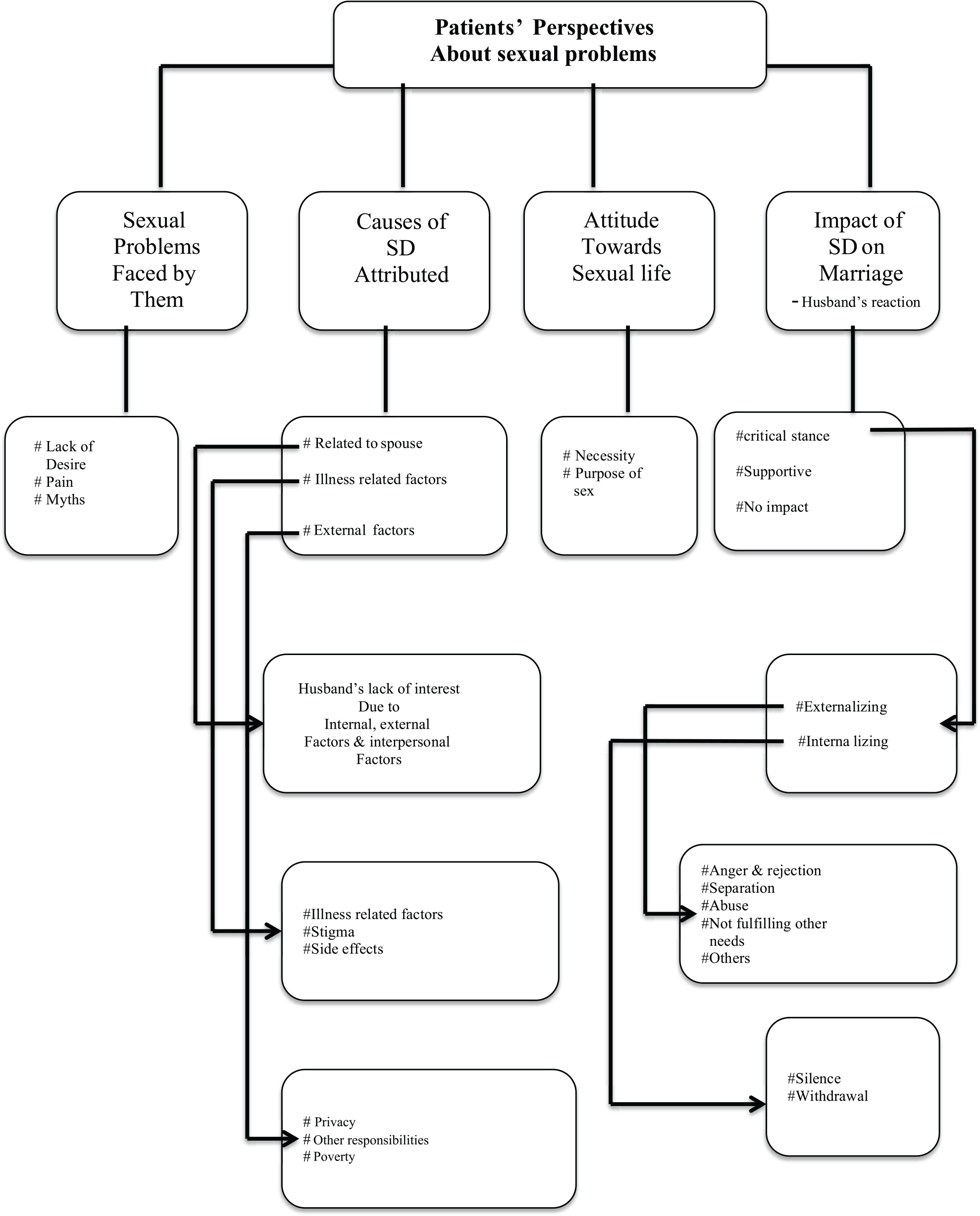
Patient’s Perspective About Sexual Dysfunction
4 main themes arrived in this aspect:
Sexual problems faced by the patient Causes of SD attributed by the patient The attitude of women toward their sexual life Impact of SD on marital relationship/spouse
Sexual Problems Faced by the Patients
3 themes emerged describing the sexual problem. Each theme is elaborated with examples
Lack of interest/arousal Pain Myths concerning sex
Lack of Interest/Arousal
They reported that they have the least desire for sex. The thoughts about sex do not occur to them. Many of them said that it has been the same for many years. They also reported that they never remember having so much interest in sex.
Mrs. M, 36: “From the time of our marriage, I had very less interest only.”
Mrs. MM, 28: “I am not getting any sexual feelings at all.”
Pain
Pain during or after intercourse was another major concern among the patients.
Mrs. V, 28: “Whenever we do it, I have pain and immediately my happiness goes off. I can’t enjoy further. Since this has been happening regularly…I think that is one of the reasons why I am not interested.”
Myths Concerning Sex and Sexual Interest in a Woman as Taboo
Patients had many myths related to sexual intercourse and practices. These were related to the action itself or the consequences of it. These myths may have been conceived and colored by cultural factors. Some of the myths are interlinked with the illness also.
Mrs. K, 32: “If we both start talking again and having a relationship, that may worsen my illness.”
Mrs. A, 3: “In a family, only the husband should initiate such things... It’s a shame for a female to go and ask the husband.”
Causes of the Sexual Problems According to the Women
4 subthemes emerged under this category:
Factors related to spouse Illness-related factors Impact of the illness External factors
Factors Related to Spouse
Again this had auxiliary themes
Mrs. P, 29: “His interest in sex is also less.” Mrs. A, 30: “As I started gaining weight, he started hating me.”
Mrs. U, 38: “Now he has married another woman also. After that, he completely lost interest.…. So, when he wanted to marry that another woman I didn’t oppose. Let him be happy.…” Mrs. A, 30: “But once he drinks, he will be interested to have sex…but…I hate that smell. I will feel like vomiting and will get a headache.” Mrs. P, 29: “He is always busy in his business; there are lots of problems in that. He struggles a lot to face them, so he is also not breaking his head about this.” Mrs. M, 36: “He drives vehicles to far places. When he comes back, he will be very tired and sleep off.”
Mrs. P, 29: “We don’t talk much about this unless he feels like having it... he would call me and tell me something about it…otherwise, we don’t talk about it.”
Mrs. V, 28: “Sometimes the pain will be very severe…. But he will never understand. The more I complain about the pain, the more harshly he would do. I hate it.”
Mrs. V, 28: “He laughed and mocked when I said that you gave a letter to the gynecologist for my pain…. He doesn’t consider that as a problem…He won’t take me to that doctor.”
Illness-related Factors
Women reported that illness had a great impact on sexual issues. These were attributed to the illness itself, the stigma associated with the illness, and the side effects of medication.
Impact of the illness
Mrs. P, 29: “The first time when my mind got upset, I could not do anything related to this (sex)…”
Mrs. K, 32: “Since the time I became ill and admitted here… He came and saw me once. After that, he doesn’t speak to me. Suddenly he stopped talking to me. I think that he does not like me since I am having this mental illness. He told that he feels ashamed to take me out because I was talking to myself…and laughing to myself.”
Mrs. U, 38: “The moment I finish my works and take tablet I would be half asleep. And I don’t have time to think about this issue.”
Mrs. G, 35: “Only after taking tablets.... These tablets had made me like a toy. I always want to lie down…whether I sleep or not.”
External Factors
There are external factors, which the patients attribute as the possible causes for their sexual issues. It either affected the patient alone or the couple as a whole. The following themes emerged in this aspect.
Mrs. V, 28: “Whenever we do the sexual act, my son is disturbed, gets up and cries. I am scared that he may see us in that state.” Mrs. K, 32: “My husband says that we both should not even sit together in children’s presence.” Mrs. V, 28: “Sometimes my husband would call me. I would be busy with some work…no one is there to help me. So, I will refuse.” Mrs. U, 38: “My mother in law…she is 80 years old. I have to take care of her. Recently she had a fracture also…so I am attending to her needs. My 3 brothers in law and their families…. We all live together. My sister in law also lives nearby. On Sundays when the children have holidays… all of us assemble. On other days also we have plenty of work, which fits into the time. Totally there are 9 children…. You can imagine how much of work we would have.”
Mrs. G, 35: “When I don’t have money to pay for my son’s school, will I be thinking about these issues?”
Impact of Sexual Problems on the Marital Relationship
The following 3 themes emerged:
Critical stance Understanding and supporting No impact at all
Critical Stance
According to most of the women, husbands reacted negatively toward the patient’s lack of interest. They either externalized it by being angry or irritable or internalized it by being sad and upset.
Mrs. V, 28: “Always he is irritated towards me…. If I try to ask further, he would walk out or shout at me….” Mrs. V, 28: “Nowadays he talks about divorce very often. Called my parents and asked them to take me home….” Mrs. K, 32: “Before the admission, he beat me badly. My mom said that I ran out of the house without clothes, that’s why he beat me. Even after going home from the hospital he beat me saying that I have caused a lot of embarrassment in the neighborhood.” Mrs. A, 30: “He calls me by names…… Elephant…buffalo…etc. When he watches television, he would say…look at that woman…. This woman…. How slim they are! When we go out to the town also, he would say that. So, I stopped going out with him. …I don’t even sit and watch television with him.” Mrs. V, 28: “Nowadays, he is not giving enough money for domestic expenditure also.”
Mrs. GA, 24: “Initially he would drink only once in a week…for the past two years, he drinks very often.”
Few of them had not expressed anything toward the wife, but they became sad or withdrawn. Both had happened between the same couples, at different point of times.
Mrs. V, 28: “Off late he is very silent. Not even eating food at home. We converse barely.”
Understanding and Supporting
Though the majority of women reported negative reactions, some husbands were reported as being supportive of the sexual problems.
Mrs. M, 36: “He has never compelled me for sex till now.... He will be looking forward to my permission…. He would tell me that he feels sorry that I am taking medicines, which will make me asleep.”
No Impact at All
Some women reported that their husbands neither expressed support nor took a negative stance. They were silent about these issues. And wives did not know what was in their husband’s mind. They were unsure whether it was due to unconcern about sexual issues or reluctance to discuss it with the wife.
Mrs. G, 35:
Attitude of the Patient Toward Sexual Issues
The attitude of patients toward sexual issues was diverse. However, most of them did not consider it a problem.
Attitude Toward (Normal) Sexuality
Attitude toward normal sexual functioning was almost similar among this particular group that most did not consider sexuality as an important aspect of life. Also, many consider it as a mandate responsibility than a pleasurable activity.
Mrs. K, 32: “I have never thought that it is necessary.” Mrs. G, 35: “I don’t think sex is essential for living.”
Mrs. M, 36: “I am here to fulfill what he wants…. If we have it that’s fine…If we don’t have it also it’s fine.”
Mrs. MM, 28
“Coz it’s my duty to please him, right?”
Attitude Toward Sexual Problems
Although all of them invariably had a low desire and infrequent sexual activity, many of them did not consider it as a problem.
Mrs. MM, 28: “I don’t think about it at all…I never considered it as a big problem”
But a few of them had transiently thought that their SD would have caused problems in the relationship and sought to settle things.
Mrs. V, 28: “Since he is not talking, I thought that he may be upset because I am not co-operating in sexual issues. So, two weeks ago I invited him voluntarily.”
Discussion of Their Sexual Issues With Mental Health Professionals
Mental Health Professionals’ Stance
Most of the patients reported that hardly any of the MHPs ever enquired about sexual issues to them. None of the MHPs had taken the initiative to inquire about sex-related issues with the patient in spite of the patient being on antipsychotic. Even if they had asked about sexual functioning, it was not a detailed evaluation.
Mrs., 32:
Mrs. M, 36:
Patient’s View About the MHP’s Stance
Again, the response was diverse, that a few wanted the MHPs to discuss, a few did not want to discuss, and a few were impartial.
Mrs. V, 28: “This is the only place I come. So, if doctors working here help me that will be better. I think they can help me in solving these problems.”
Mrs. K, 32: “I expect that doctors should talk about it. I have not spoken to anyone freely like this. Not only about this…. I don’t have anyone to talk about anything. So, this hospital is the only place where I can talk to someone freely.”
Mrs. GA, 24: “Doctors are anyway third persons, they should not know about such high personal issues. I don’t think they can help also.”
Reason’s for Patients not Volunteering the Information
None of them had ever voluntarily informed the sexual issues they had. They gave different reasons for the same. And in this, two themes were found, among which one is related to their feelings and the other one related to their fear of negative evaluation from the MHP.
Reluctance and Shyness
They were feeling shy or uncomfortable in discussing this issue. Though there wasn’t any particular reason for this, it was evident that they were convinced about it.
Mrs. U, 38: “It’s something which I don’t feel like discussing.”
Mrs. MM, 28: “Very difficult for me. I have an uneasy feeling... Sometimes male doctors only see me… how can I talk about it?”
Patient’s Fear of Negative Evaluation from the MHP
A few of them were not volunteering information about the sexual issues because of the fear of negative evaluation.
Mrs. U, 38: “They may think something bad about me.”
Mrs. M, 36: “But it’s a family matter. Immediately I can’t share this to the doctor. If I tell them, they may think “What? This woman is bad…openly sharing her family matters to me? …. They may also wonder how my character will be….”
Patient’s Expectation of the Interview if It Happens
A few of them who wanted the discussion to happen had some specifications which were mostly related to the following.
Patients’ Perspectives About Their Sexual Problems
Patients’ Perspectives Regarding Discussions with the MHP
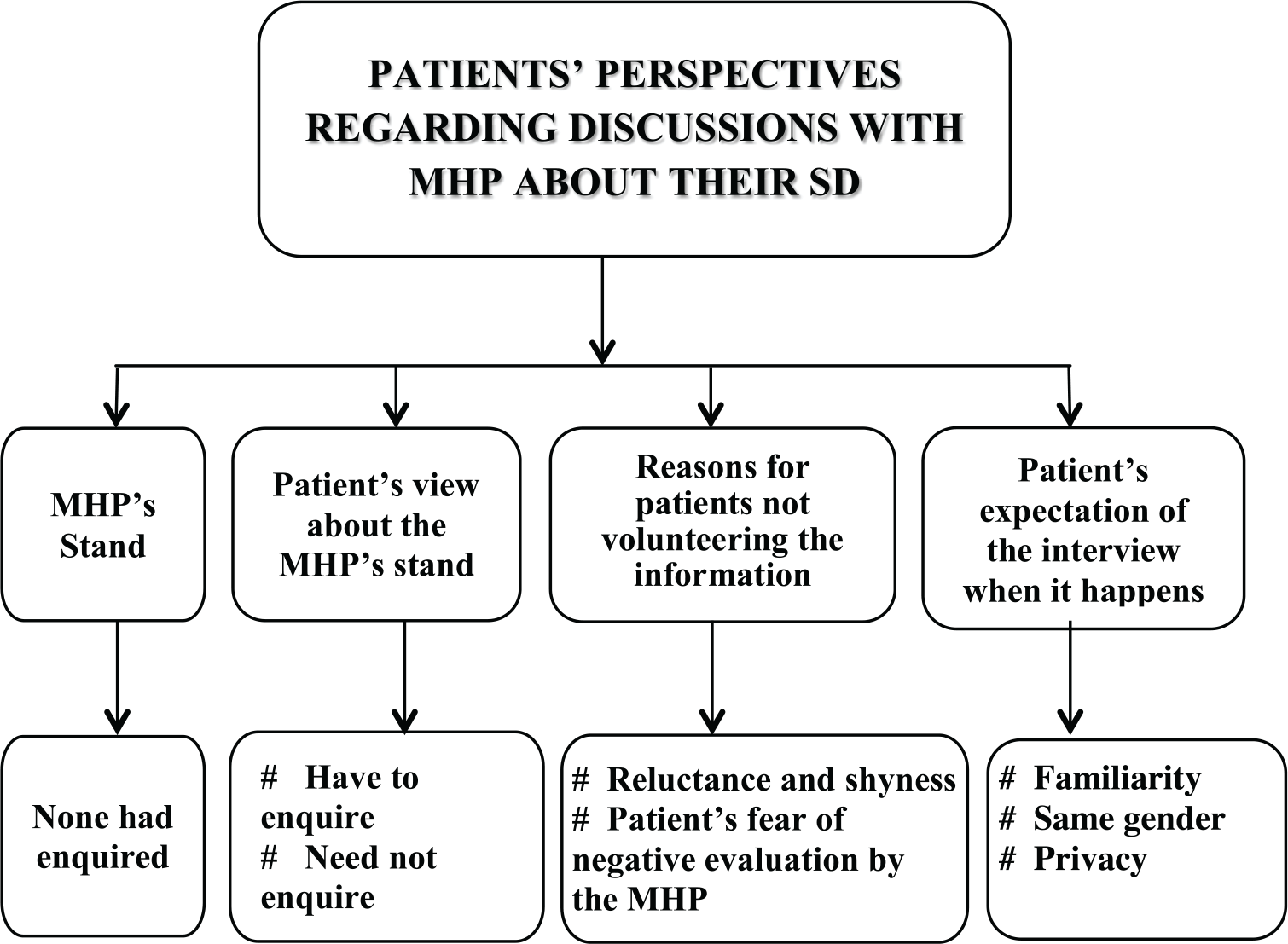
Gender of the MHP
Many of them wanted only the same gender clinician to talk with them, though few said that it doesn’t matter.
Mrs. M, 36: “But only females should talk. When males talk, I will be shy.”
Mrs. G, 45: “How can we ever talk to males about such things? That will be bad.”
Need Some Familiarity
Patients felt that they need some familiarity to discuss these issues. They feel that they can’t talk about it to an unknown person.
Mrs. M, 36: “We can’t talk about this to unknown persons. I know you well that’s why I am talking with you freely.”
Need of Privacy
Patients expressed that the interview should take place in strict privacy.
Mrs. V, 28: “It should be in complete privacy like this. In OP often someone will come and open the door….”
Discussion
The discussion proceeds under the following headings pertinent to the aim of the study. Part 1 will discuss about patients’ attributions about sexual issues and Part-2 will deal with factors-affecting discussion about sexual issues between MHP and patients.
Part 1
Many of the women had sexual issues such as pain, loss of arousal, feelings, or interest. And the causes of sexual issues attributed by the patients diverged. Though this study was done on a group of patients suffering from schizophrenia, many of the findings may be applied to normal population also. Many of them had factors unrelated to the illness, which contribute to their sexual problems.
In India, where marriage is seen as a union of two families rather than two individuals, other roles and responsibilities cannot be avoided. And most of the women accept it and adapt to it. Although the joint family system is almost at its demise, still some families live together due to various reasons. In such a setup, the expectations kept on a woman are higher and often compared with other females of the same roof. Automatically, women prefer to fulfill those roles and sex-related issues are neglected.
In people belonging to lower socioeconomic status, privacy-related issues contribute to lower frequency of sexual intercourse, and doing it with the fear of being noticed by children. This problem can be settled in those houses where more than one room is available. Others accustom to it and live.
Also, the culturally ingrained taboos related to sex are very common such as not to talk about sex, not to discuss with anyone including the husband. This eliminates the possibility of having a source of ventilation to such sensitive issues. Myths such as “woman from the good family should not have a desire for sex” indicate the status of sex education and awareness programs that exist in the country. Also, patient’s myths that “having sexual intercourse will lead to the relapse of the illness” indicate the failure of adequate psychoeducation from the mental health system. Cultural influences are very much evident in taboos like “women should not initiate or invite her partner for having sex.”
Poverty is the evil base of all, and sexuality had not been exempted from it. Statement of a woman that she is more worried about tomorrow’s financial needs than her sexual problems shows how automatically the sexual needs take a backseat.
Sexuality is an intricate link between two people. Hence, any factor affecting the spouse will affect the partner as well. It was very evident from the excerpts that many factors related to the husband affect the sexual function of the females. In clinical interviews, this aspect is completely ignored most of the times. Also, the scales assessing sexual functioning pay the least attention to factors such as the health of the spouse, interest of the spouse, etc. Until all these factors are kept in mind and assessed, a comprehensive sexual history may not be obtained.
Schizophrenia is an illness already causing so much turmoil in the patient’s life. The stigma associated with it victimizes the patient in many ways. The nature of illness per se and the side effects caused by the medications sometimes shoves the spouse to distance himself from the patient. Yet a few women reported that their spouses don’t force them to have sex. Unless otherwise we interview the spouse, the reason behind this will be a mystery. There are high possibilities that spouses may also harbor some myths and taboos related to illness and sexuality.
In routine history-taking of schizophrenia, our focus of assessment ends once we find the occupational functioning of the patients. But in our study, patients who don’t have positive symptoms and maintain the clinical remission have this dysfunction. As reported by many women, they lose their self-esteem by explicit criticism by the spouse. They start internalizing those and live with it. Many women undergo abuse, violence, and rejection. As Thara et al reported, many are living with the husband yet the quality of marital life remains poor. 16 As it was evident in this study, the communication and intimacy between the couple remain very low. Many a time, wives were left with confusion about what’s going on in the husband’s mind. Although we get an overview of these factors in the quantitative assessments, these in-depth interviews help us to understand the real status of a woman living in the community with schizophrenia. The negative reactions she receives from the spouse, children, and extended family are sickening. Hence, routine assessments should include a few questions about the quality of marriage and the emotional atmosphere at home.
Surprisingly, none of the women considered sexual problems as important. None seem to realize that it is a basic biological drive similar to other drives. For most of the women, sex did not play any imperative role. Is this the real scenario? Or is it because of the impact of illness, which has caused a decline in interest related to all the aspects of life? Or these women are in denial that they are not bothered about them? The answers to these questions may need more systematic exploration.
This leaves us with many questions that have to be answered in future studies. Definitely, the information derived from this qualitative study has thrown a light on the aspects that the quantitative study had not covered. So, each is contributory. Such mixed studies in research will help us to understand better and to formulate more research questions and scales, which have more inclusive domains.
Part 2
Only 1 or 2 of the MHPs had enquired about sexual issues in this group. This reflects the reluctance of MHP to discuss it. It can be attributed to various factors such as the clinician’s poor knowledge in this area, time constraint, lack of privacy in busy outpatient departments, or the personality factors of the clinician. All health professionals should receive adequate training in handling sexual issues as a routine.
Most of the patients felt comfortable in discussing this aspect with the same gender clinician. Even Indian researchers suggest that having a married female as an investigator is an asset in reducing the cultural barrier and encouraging female patients to be free in explaining their sexual difficulties. 17 So preferably opportunities should be provided for such facilities. And in our country, where public hospitals are crowded enough, provisions should be there for discussing these issues in privacy. Some forms can be given to those who are in the waiting hall, which can help to indicate such specific needs.
This is the first qualitative study from India looking into the perspectives of patient’s with schizophrenia and SD. Yet measures like respondent validation could not be done to improvise the quality of the study due to various reasons.
Conclusion
The qualitative findings support the results of our quantitative study 15 that marital and relationship factors play a crucial role in a woman’s sexuality. Any woman who has problems with sexuality has to be assessed in various viewpoints, including medical, psychological, interpersonal, and sociocultural. Marital quality and relationship factors which receive the least importance in both clinical practice and in research need to be given due attention. This will definitely take us to the next level in the concept of recovery in schizophrenia
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.