
Abstract
Abstract
In recent years, with increasing awareness and reports of child sexual abuse, government and nongovernment agencies working in the areas of child and adolescent health, education, welfare, and protection are increasingly looking to implement initiatives on child safety and psychosocial health, both from preventive and curative perspectives. It is critical, however, to recognize that the child sexual abuse programming needs to take into consideration the age and the developmental stage of children. Childhood encompasses the period from 0 to 18 years; however, sexuality-related issues of adolescents are vastly different from younger children. While the adolescent sexual rights’ debates (for adolescents) to engage in physical intimacy and sexual behavior or not may continue, most childcare workers unanimously agree on adolescents’ need for sexuality awareness and education. Adolescent sexual issues range from sexual abuse to mutually consenting romantic and sexual relationships and engagement in sexually inappropriate behaviors with young children; for the last-mentioned point, adolescents also come into conflict with the law. This article discusses the need for public health and community-based approaches to address this range and complexity in adolescent sexuality, also sharing concrete field-based, pilot-tested methodologies and resources to work on this issue.
Shifting Landscapes in Adolescent Sexuality and Related Mental Health Issues
It was only in the 1980s, when the human immunodeficiency virus (HIV) pandemic occurred and adolescents were identified as one of the vulnerable groups, and the discourse on adolescent health and sexuality was propelled into public health discourse. Much research was done on adolescent sexual behavior, mainly to understand adolescent sexual-risk behaviors in the context of pregnancy, sexually transmitted diseases and HIV, condom use, and sexual violence. Thus, the approach taken to adolescent sexuality was largely one that was negative, assuming adolescent sexual behavior to be dangerous and undesirable. However, over the last few decades, there has been a conscious attempt on the part of at least some researchers to take a different view of adolescent sexuality, ie, one that does not assume adolescent sexuality to be dangerous or pathological. 1
The concept of “normative adolescent sexuality development” includes positive adolescent sexuality,2, 3 as well as the developmental nature of adolescent sexuality, ie, what it means to be a healthy sexual adult. While normative is defined as the average or expected behavior of individuals within a group or community, the concept of normative sexuality development does not suggest a “right” age or time to begin sexual activity; it refers, instead, to the qualities of sexual development, namely, the development of healthy sexual attitudes, behaviors, relationships, based on the understanding that adult sexual behaviors stem from adolescent learning, and experience in this area. 1 Additionally, the shift from the term “sexual development,” which largely refers to physiological aspects of sexuality, to the term “sexuality development” also indicates how the nature of adolescent sexuality work has changed. 4
In India, reports on sexual and reproductive needs of young people highlight issues that have implications for gender and sexuality life skill education in adolescents. According to these reports, first time sexual activity for many occurs at a young age. Despite laws on early (child) marriage and harmful traditional practices, marriage continues to take place in adolescence in many communities. Sexual relations are often unsafe and for many young women, unwanted or forced. Married young women, particularly adolescents, are more at risk of sexual violence. Evidence also reflects that young women, particularly adolescents, are at greater risk of unplanned or unwanted pregnancies than adult women; consequently, more adolescents seek abortions. 5 All these issues indicate the need for building supportive environments for adolescents and young people, with a particular focus on age and gender disparities and related inequalities.
Indeed the Nirbhaya incident that happened in 2012, which resulted in changes in the Juvenile Justice Act, by way of introducing a transfer system for adolescents aged 16 to 18 years for commission of heinous crimes, might appear to have had serious implications for children/adolescents in conflict with the law; however, the incident is also indicative of the state of women’s safety and attitudes toward women, thus reiterating the need for education and awareness on gender equality and gender-based violence issues, especially amongst adolescents and youth. According to the Verma committee report 6 which draws from the chapter on “Re-Thinking Masculinities” by Seshadri and Chandran, 7 patriarchy is perpetrated through socialization of children, who internalize these socialization processes to then live out traditional gender roles: “Boys are conditioned to believe that power and violence resides unchallenged in their bodies and girls are brought up to uphold notions of traditional values and virtues to protect family honor.”
The Verma Committee report also draws a study on the issue of gender-based violence in schools to speak of the need for a gender-sensitive framework for understanding violence in schools and that gender-based violence can be broadly grouped into two categories:
(a) Explicit gender (sexual violence), which includes sexual harassment, intimidation, abuse, assault, and rape and (b) implicit gender violence, which includes corporal punishment, bullying, verbal, and psychological abuse, teachers unofficial use of pupils for free labor and other forms of aggressive or unauthorized behavior which is gender specific.
The study thus states that “school as a social arena is also marked by asymmetrical power relations” and it therefore functions as an important space for correcting and redefining power relations, by enabling feminine and masculine identities “in a rational, correct, egalitarian, and sensible way.” 7 ”
While empirical evidence reflects the need for gender and sexuality life skills programs and government policies advocate for such programs, schools and other childcare institutions that are involved in health, education, care, and protection of children have not kept pace with the emerging needs and issues of adolescent sexuality. The education system still has not made the shift from sex to sexuality education—sex education focuses on the biology and physiology of sex and sexuality without enabling children and adolescents to examine and make decisions about the emotional, relational, and gendered contexts in which decisions about physical intimacy and sex are made. Life skills education in schools, whether about sexuality or other issues, tend to adopt didactic “moral values” approaches versus experiential approaches and use of creative methods that allow children to examine and analyze situations and information, and make their own decisions in ways that are healthy, happy, and responsible.
Finally, in recent years, public awareness and discourse on child sexual abuse, which may also have resulted in higher reporting of child sexual abuse, has also brought adolescent sexuality issues to the fore. First, the grooming and manipulation processes involved in adolescent sexual abuse dynamics emphasizes the need for sexuality life skills training that empowers adolescents to understand and recognize less overt and more insidious methods of sexual abuse. Second, one of the challenges in child sexual abuse work, including the implementation of The Protection of Children from Sexual Offences (POCSO) Act, 2012, 8 is distinguishing between abuse and mutual consenting relationships when sexuality issues play out in a peer-relationship context. When a sexual relationship between two adolescents is mutual and consenting, it cannot be considered to be child sexual abuse; the decisions they make about physical intimacy, living together, and even marriage in some cases, however, invite POCSO charges on the boy and not the girl (despite her participation in the decision-making processes), thereby reflecting a clear gender bias in the workings of POCSO. Such situations of mutual consent necessitate stronger sexuality decision-making skills in adolescents, making a case again, for gender and sexuality life skills training for adolescents.
Rationale for Use of Life Skills Approaches to Address Community-Based Adolescent Sexuality and Mental Health Issues
The World Health Organization (WHO) defines life skills as “adaptive and positive behavior that enables individuals to deal effectively with the demands and challenges of everyday life.” Core life skills for the promotion of child and adolescent mental health include decisions-making, problem-solving, creative thinking, critical thinking, effective communication, interpersonal relationship skills, self-awareness, empathy, coping with stress, and emotions. 9 In recognition of the importance of life skills and with a view to making it accessible to all children and adolescents, the WHO and other national initiatives advocated strongly for life skills education to be made available in schools, through training of teachers and as part of school mental health programs. 10 The reasons for developing life skills approaches to address community-based adolescent sexuality and mental health needs are four-fold approach, as discussed further:
First, most mental child-health problems (except for those such as psychosis and those caused by organic factors or physiological problems) may also be viewed as life skills deficits. For instance, violent and abusive behaviors result from children’s inability to regulate emotions, negotiate interpersonal relationships, and/or resolve conflicts in alternative or creative ways; thus, the objective of any therapeutic work with such children will be to enable them to acquire the life skills to manage anger and aggression—in other words, to manage emotions, develop creative thinking, problem-solving ability, and conflict-resolution (life) skills. Children in difficult circumstances, in vulnerable community settings, whether living within dysfunctional families or in childcare institutions, are exposed to experiences of deprivation and abuse from early childhood, causing them to develop emotional and behavior problems which may also be viewed as being created by life skills deficits, ie, due to their difficult circumstances, children have not learnt certain life skills, and that results in emotional and behavior problems. These life skills deficits, if not addressed, exacerbate emotional and behavior problems, increasing the risk for more serious and chronic mental health disorders. Severe emotional deprivation and difficult family contexts may have led them to seek out relationships of love and sexuality either with their peers or older adolescents or adults; in such cases, while there is apparent “consent,” they are not always cognizant of the health and psychosocial risks of their sexual behaviors and decisions, and are thus vulnerable to abuse and serious health consequences. Many of these children have received little supervision and have not been engaged in discussions on how to make choices about relationships and sexuality.
Second, in terms of sheer numbers, there is a tremendous challenge in reaching out to address the psychosocial care needs of children in difficult circumstances. Every child comes from difficult and traumatic circumstances; each child is unique in that he/she has his/her own story, and is impacted again, in unique ways. Life skills training approaches take into consideration the fact that children in similar contexts have different processes and outcomes, and conversely, children with the same manifest issues come from different contexts. Given that all children in difficult circumstances require psychosocial assistance and that resources are scarce, providing individual interventions to each child is not possible. Trained personnel, with the knowledge and skills on how to deal with children’s issues, especially with complex and difficult problems, are especially scarce and have resulted in inappropriate and unhelpful responses to children, on the part of caregivers and childcare agency staff. As a result, many children do not receive the assistance that they require, in order to deal with the difficult psychosocial contexts, they are in and come from. Life skills approaches, which generally use group intervention approaches, therefore, ensure that larger numbers of children receive psychosocial assistance to address their emotional and behavior problems by helping children build the life skills that they may lack.
Third, sex education (as it is commonly known) is one of the few forms in which community-based sexuality education is conducted, mainly in schools and (relatively very few) childcare institutions. Sex education is very different from life skills education and training on sexuality and relationship issues; the former merely imparts information about the body and physiological processes of reproduction, usually in a manner that is didactic (teacher to student or parent to child), and the latter may include some discussions of physiology, especially on topics that pertain to health and safety but the emphasis is on the socioemotional component of sexuality. This includes an understanding of emotions, such as attraction, love, and relationship contexts, based on which the recognition of abuse and coercion take place, and also does the learning of skills, such as assertiveness and refusal (saying “no” to sexual overtures if desired), negotiation (for condom use and safe sex), and problem-solving (coping with peer pressure that compels an adolescent to experiment with sexual acts). The life skills approach to sexuality education thus recognizes that sex education needs to be situated in a larger socioemotional context for it to be meaningful and impactful for adolescents.
Finally, in the wake of the child sexual abuse epidemic that has gained much publicity in India, in recent years, a great many agencies have become proponents of the “good touch/bad touch” approach to child sexual abuse prevention and awareness programs which are done at the community level. In this, it appears that the essence of what children need to learn about sexuality and abuse is to learn what “good” and “bad” touch mean—the former referring to any affectionate or neutral touch by another person and the latter referring to any touch that is sexual in nature. Such an approach completely disregards person, time, place, and context. Life skills approaches to sexuality do not advocate the use of “good touch and bad touch” or “safe and unsafe touch” approaches to sexual abuse prevention. This is because the so-called bad touch can feel good and right to adolescents; in certain situations, especially where abuse entails lure and manipulation or complex grooming processes, children and adolescents can find it exceedingly difficult to distinguish between “good and bad touches.” Also, promoting sexual touch as “bad touch” negatively impacts the development of affirmative sexuality, ie, children and adolescents should not associate sexuality as being “bad or negative” as this will have other harmful consequences to their relationships, health, and happiness in the future.
Materials for Intervention: A Life Skills Manual on Gender, Sexuality, and Relationships
For Whom It Was Developed and How?
This life skills series (The Community Child and Adolescent Mental Health Service Project has also developed an Adolescent Life Skills Series on Socio-Emotional Development [also available on the project website:
Note: The Department of Child and Adolescent Psychiatry, NIMHANS, has been implementing a community-based child and adolescent mental health service project with support from Department of Women and Child Development, Government of Karnataka. Aiming to provide direct services and capacity building in primary health care centers, government schools, anganwadis, and childcare institutions, it is based on the premise that in the Indian context, there is a vast gap between child and adolescent mental health needs and resource availability, with the few available resources being concentrated in tertiary-care health facilities; and that children in difficult circumstances, who are at the greatest risk of mental health morbidity, often have the poorest access to quality psychosocial and mental health assistance
It was piloted, refined, and revised following its use with over a 100 children belonging to various categories of vulnerable children, namely, street and working children, orphan and abandoned children, children infected/affected with HIV, and children affected by gender and sexuality vulnerabilities.
The series is for use by all persons who work with children, including teachers, counselors, child protection staff, and special educators, ie, persons working with children in education, health, and welfare agencies. It has been developing for use with neuro-typical (ie, children without intellectual disabilities) children ages between 13 and 17 years. While the Project piloted this largely with children’s groups, several of the methods have been developed through use with individual children in childcare institutions and in tertiary care settings, such as the NIMHANS, in the following context of depth therapeutic work with adolescents who
have been sexually abused, have run away to “marry” or be in mutually consenting romantic and sexual relationships, come into conflict with the law due to sexually inappropriate behaviors (often with alleged offences related to sexual abuse of young children).
The life skills series is thus to be used with all children, whichever vulnerable subgroup they belong to as gender, sexuality, and relationship issues are relevant to them; in particular, the manual needs to be used with adolescents who
have been sexually abused, so that they learn to be safe in the future; have engaged in mutually consenting romantic relationships, including physical intimacy; have engaged in sexual offences, ie, those who may have sexually abused peers or young children and may have been charged for the same under POCSO (and are in the observation home and/or in other childcare agencies such as schools and child mental health agencies).
However, by definition, all children are meant to acquire life skills, so these modules are for use for not only curative purposes, ie, to address specific sexuality- and relationship-related problems that children may be confronted with but also for preventive purposes, ie, to prepare children to make appropriate decisions in the area of gender, sexuality, and relationships in the immediate and distal future. In other words, given the universal importance of sex and sexuality to human beings from a vulnerability perspective, as well as in preparation for the future, and in the interests of a happy, healthy, and responsible (sexual) life for all; this series should be implemented with all adolescents, no matter which subgroup they come from.
Objectives of the Gender, Sexuality, and Relationship Life Skills Series
This life skills series manual was developed with the following specific objectives:
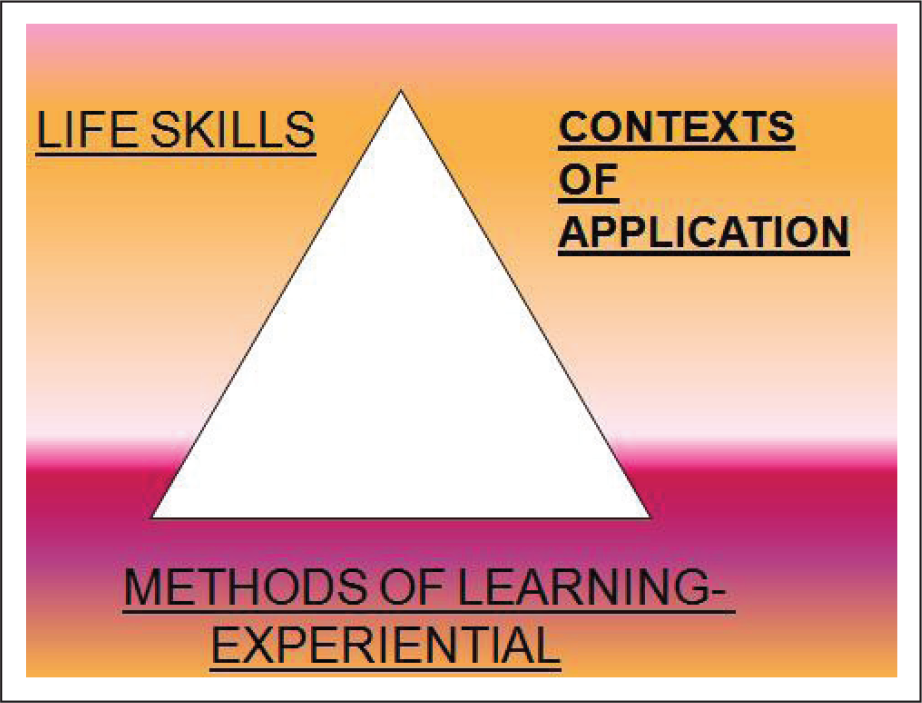
To allow for sharing of experiences and narratives children’s daily realities and past experiences so as to take perspectives on them for the future. To address life skills domains (as outlined by the WHO) covering the broad areas in which children need to acquire skills in order to address their situations and experiences. To enable children to develop specific skill sets through the various creative and process-based activities. To thus triangulate life skills, contexts of application (situations/experiences), and methods of learning (experiential activities), as shown in the figure above.
The domains and skills may be generic but allow for problem-specific themes to emerge. Also, unlike some manuals that advocate a skill-based approach, focusing on the learning of a life skill, this series takes a context-based approach. This is because a specific area, such as dealing peer pressure in the context of sexuality, may require the use of many life skills, such as assertiveness, negotiation, problem-solving, and decision-making. Also, a single life skill, such as decision-making, may apply in several contexts relating to sexuality, such as running away, delaying of marriage, use of protection, etc. Therefore, the approach, taken in this series, ensures that the learning of life skills is more relevant to children’s real-life contexts and the necessary healing, behavior, and health transformations that need to occur.
Finally, the series are laid out such that they provide a detailed but minimum standard level of assistance and intervention in a systematic manner. While they may not always be a substitute of in-depth individual therapeutic work and other curative methods, they provide children with a holding space, a platform to express their emotions and views, share their experiences, and reflect and take perspective on life and relationship–sexuality situations, past, present, and future.
Components of This Life Skills Series: How It Is Organized for Use
The series is organized into two sections. Section A includes a set of activities on gender, because learning about appropriate sexual behaviour is predicated on an understanding of gender roles and responsibilities, including gender stereotyping and discrimination issues. Thus, section B, on relationship and sexuality issues, is predicated on an understanding of gender issues.
The activities in section B, on relationship and sexuality issues, focus on addressing the above-described contexts of vulnerability that adolescents find themselves in, as well as the limitations of the “good touch/bad touch” approaches, by first acknowledging adolescents’ desire for love, attraction, and need for engagement in sexual activities—in fact, it takes a rights-based approach to sex and sexuality, implementing the activities on the premise that adolescents are at a developmental stage wherein they have love–romance–sex needs and that they have the right to have these needs met. However, the issue is how they make decisions about meeting their romantic and sexual desires, and these decisions cannot be made randomly or whimsically.
The series has thus developed what is called a “window approach” to provide a framework for decision-making, a window approach means not speaking directly about abuse prevention (which may be the final objective and therefore the last discussion in the series) but “opening each window” one by one to introduce different but related concepts of personal safety and abuse: starting with (acknowledgement of) love/attraction and physical pleasure, it moves on to examining and understanding concepts of privacy, consent, and boundaries; learning about health and safety; and finally to consider relationship contexts (roles and expectations of others, and activities we do with various people by virtue of our relationship with them). Adolescents learn to use each window and concept individually and then collectively to arrive at decisions about sex and sexuality behaviors.
Each module focuses on a single topic but which may have many aspects to its learning and understanding—as outlined in its objectives. Therefore, each module or a single topic may consist of up to three to four activities. Each activity first describes the “methods and materials,” it will use, and then lays out the process or the steps to be followed on how to implement the activity; the process is followed by “discussion” which provides questions for discussing and processing the activity and summarizing thoughts and learning derived from the activity. While the modules are best used in chronological order, they can also be used as stand-alone modules, in case the facilitator urgently requires to address one or another issue first. This series is accompanied by a set of materials, including film clips.
Concluding Thoughts
The framework and activities in the above-described life skills series on gender, sexuality, and relationships are based on the premise and view that adolescents have sexual rights and that they have the right to make a choice on engagement in romantic and sexual relationships. It is important for facilitators to take this perspective as well. We are aware that different people/facilitators have different personal views on the “right” age for adolescents to engage in physical intimacy and romantic relationships, or that many may not consider it appropriate for a 16-year-old adolescent to be engaged in physical intimacy; we acknowledge and respect the concerns of such childcare workers and facilitators. However, it is imperative for counselors and facilitators to be completely open and nonjudgmental in their discussions on decision-making on sexuality and relationship issues. Doing otherwise and imposing one’s own ideological and moral standpoints will only appear coercive (and nonprogressive) to adolescents, who will then either hide their concerns or not communicate their questions and concerns openly.
While many agencies attempt to impart life skills (and state that they arrange for life skills group activities with children) on issues, such as sexuality and relationships, they appear to follow didactic positions, adopted as a result of their personal opinions and viewpoints. This contradicts the essence of life skills promotion work, which entails that all individuals participate equally in the production of knowledge, and that this is a continuous dialogue, and that learners are the subject, not the object, of the process. What this means is that life skills development is not about articulating one’s own positions and convincing adolescents to adopt the same beliefs, but it is about adopting an open stance (despite one’s own experiences and personal opinions) and creating a space for debate and discussion, so that adolescents can examine and analyze a given issue or situation from multiple viewpoints and come to their own conclusions on what might be the best course of action. In this, the use of creative methods, such as stories and narratives, theatre, film, and other art forms, helps create the life situations and contexts (such as marriage, sexuality, and conflict) that form the basis of the discussion.
Ultimately, the sexuality career of each adolescent (or individual) is unique. It is through many complex processes and experiences disseminated over time that an affirmative sexuality identity emerges. The development of this affirmation can occur even when there are negative experiences, such as abuse, provided methodologies are used for both the experiencing, and re-interpretation of the aesthetics, and joyous spontaneity that sexuality should encompass. Public health education approaches to adolescent psychosexual health and behavior change should therefore move away from models that focus only on abstinence, deterrence, or disease, and instead, adopt life skills training approaches that enable adolescents to develop and choose their individual and unique beliefs and value systems with regard to sexuality behavior, and draw their choices and decisions from their lived experiences.
Supplemental Material
The manual and accompanying materials, such as pictures and film clips, are available on the NIMHANS Community Child and Adolescent Mental Health Service Project website:
The direct link to the Gender, Sexuality and Relationships Life Skills Series is
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.